
Abstract
Staphylococcus aureus small colony variants (SCVs) are associated with chronic and persistent infections. Methicillin-resistant S. aureus (MRSA) SCVs cause more severe infections and mortality rates are higher in comparison with infections caused by MRSA. Our objective was to document the prevalence and phenotypical characteristics of SCVs among MRSA blood isolates. MRSA strains isolated from blood during 1999–2009 were evaluated retrospectively. Among 299 MRSA isolates, suspected colonies were inoculated onto Columbia blood agar and Schaedler agar. Columbia blood agar was incubated in normal atmosphere and Schaedler agar in 5–10% CO2, both at 35°C. If the small, nonpigmented, nonhemolytic colonies on Columbia blood agar were seen as normal-sized, hemolytic, and pigmented colonies on Schaedler agar, they were considered as MRSA SCVs. Six MRSA SCVs were detected. When subcultures were made, four of them reversed to phenotypically normal S. aureus, but two isolates were stable as SCV phenotype. The prevalence of SCVs among MRSA blood isolates was found as 6/299 (2%) with 2 (0.67%) stable. The detection of SCVs among MRSA blood isolates was reported from Turkey for the first time in this study. As the clinical significance of MRSA infections is well documented, evaluation of MRSA SCVs in clinical samples, especially from intensive care patients and those who have chronic and persistent infections are important to consider.
Introduction
S
Prevalence of S. aureus SCVs among clinical samples varies between 1% and 30% in different studies.3,6,7 Association of S. aureus SCVs with chronic and persistent infections has only been deemed suitable in recent years. Since SCVs have increased their potential to intracellular surviving, the isolation of SCV phenotype is usually associated with the persistence of S. aureus in cystic fibrosis (CF) patients.4,8
There is one report of the epidemiology of methicillin-resistant S. aureus (MRSA) SCVs with the description of an outbreak, retrospectively analyzing nine previously identified cases. MRSA SCVs are reported to cause more severe infections and mortality rates are higher in comparison with infections caused by MRSA in this study. 9 Also the prevalence of MRSA colonization was found to be 5%, including seven SCV isolates in a multicenter prospective survey of S. aureus colonization in a CF population. 10 However, the prevalence of MRSA SCVs among blood isolates has not been reported yet. Our objective was to document the prevalence and phenotypic characteristics of SCVs among MRSA blood isolates retrospectively.
Materials and Methods
A total of 299 nonduplicate MRSA strains isolated from blood samples in Hacettepe University Adult Hospital, Clinical Microbiology Laboratory (Ankara, Turkey) during 1999–2009 were evaluated. All isolates were identified as S. aureus by colony morphology, Gram staining, catalase, and tube coagulase tests. The identification and antimicrobial susceptibility tests have been performed by either a Scepter Automated System or a Phoenix™ system (Becton Dickinson and Company) according to the manufacturer's recommendations. According to the CLSI guidelines, disk diffusion testing with 1 μg oxacillin and/or 30 μg cefoxitin disks on Mueller-Hinton agar was used for the confirmation of MRSA isolates. 11 All isolates were then stored at −80°C using Brain Heart Infusion Broth with 15% glycerol until testing for determining the prevalence and phenotypic characteristics of SCVs.
Isolates were inoculated onto Columbia agar with 5% sheep blood (Columbia blood agar [CBA]; Becton Dickinson and Company) and incubated at 35°C for 24–48 hr aerobically. Nonhemolytic, nonpigmented, pinpoint or fried-egg colonies were considered as SCV suspected. These MRSA SCV-suspected colonies were inoculated onto CBA and Schaedler agar (Becton Dickinson and Company) simultaneously. CBA was incubated in normal atmosphere and Schaedler agar in 5–10% CO2, both at 35°C. If the small, nonpigmented, nonhemolytic colonies on Columbia blood agar were seen as normal-sized, hemolytic, and pigmented on Schaedler agar, they were considered as MRSA SCVs. Identification of the isolates consistent with MRSA SCV were confirmed by Gram staining, catalase reaction, tube coagulase result, and agglutination with the latex test (Slidex Staph Plus; bioMerieux). As S. aureus SCVs are slowly coagulase positive, coagulase tubes were held for 24 hr for a positive result. Isolates converting to a normal phenotype after subculturing were considered as reverted SCVs.
Clinical and microbiological data of the patients, from whom the MRSA SCVs were isolated, were retrospectively reviewed accordingly from patients' medical records taken by the physicians.
Results
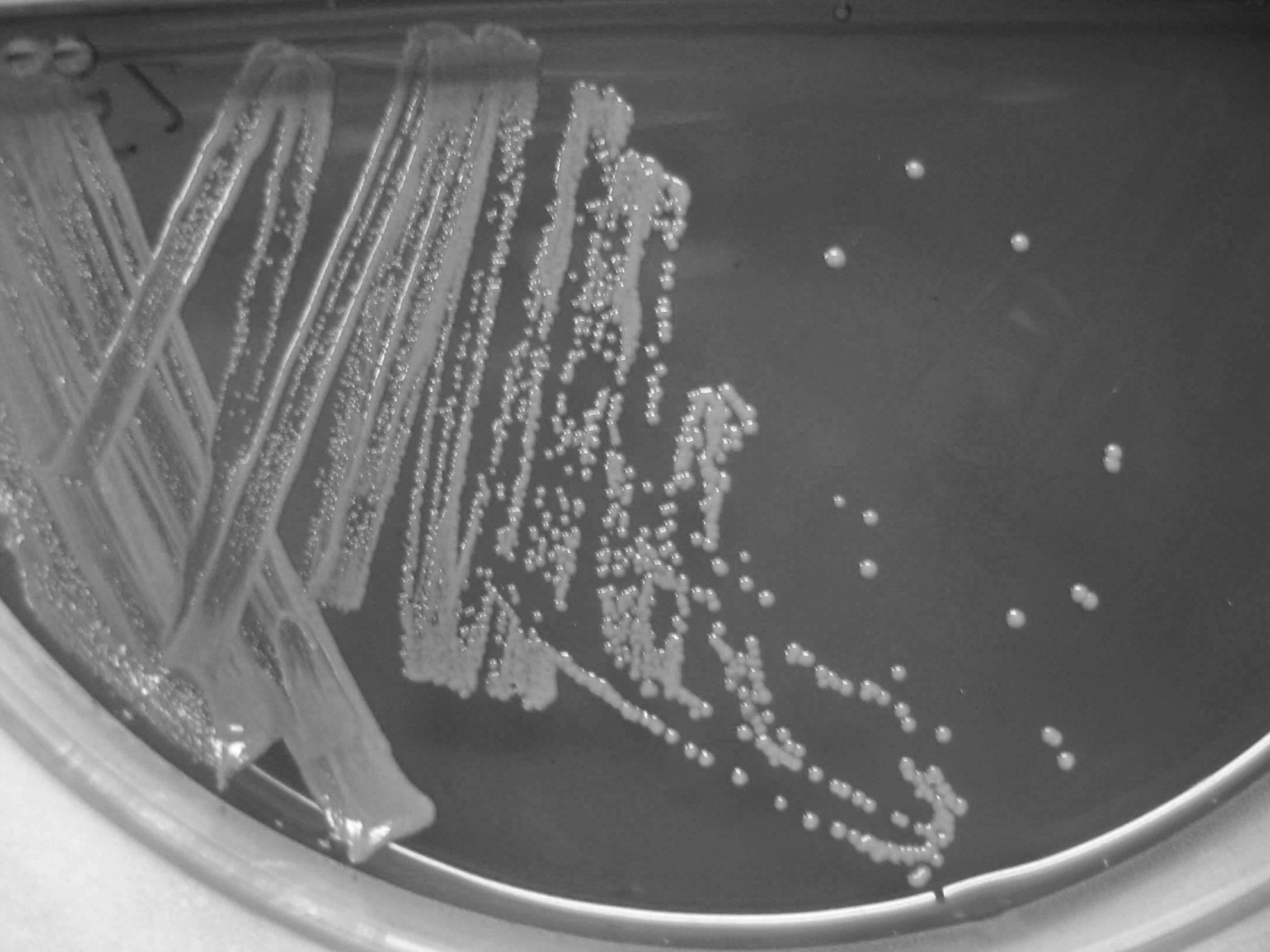
Among 299 isolates evaluated, six MRSA SCVs were detected in the primary culturing after incubation for 24 hr in an aerobic atmosphere. When subcultures were made, four of them reverted to phenotypically normal S. aureus, but two isolates were stable as SCV phenotype. One of the isolates formed pinpoint dusty colonies (Fig. 1) and the other formed small, nonhemolytic, nonpigmented colonies (Fig. 2). Both of the isolates were observed as normal sized, hemolytic and pigmented on Schaedler agar after 24 hr of incubation in 5–10% CO2 at 35°C. The prevalence of SCVs among MRSA blood isolates was found as 6/299 (2%) with 2 (0.67%) stable.

“Pinpoint ” MRSA SCV colonies on Columbia blood agar. MRSA, methicillin-resistant Staphylococcus aureus; SCV, small colony variant.
Small, nonhemolytic, nonpigmented MRSA SCV colonies on Columbia blood agar.
Clinical and microbiological data of the patients, from whom the stable MRSA SCVs were isolated were as follows.
Case 1
An 81-year-old male was admitted to the emergency service with a 3-day history of painful swelling in the left inguinal region. He also had nausea and vomiting concurrently. His medical history was unremarkable. Due to an irreducible and strangulated hernia sac he underwent inguinal hernia operation urgently on December 1999. He had high heart rate and low blood pressure postoperatively. In terms of aspiration, pneumonia developed after the operation, treatment with ampicillin–sulbactam was initiated. Intravenous ciprofloxacin was also added to the treatment. After 20 days he was transferred to intensive care unit due to the need of regular intubation. MRSA, Pseudomonas aeruginosa, and Acinetobacter baumannii were recovered from the bronchoalveolar lavage culture. Thus, antimicrobial therapy regimen was switched to meropenem, amikacin, and teicoplanin. After MRSA isolation from catheter and blood culture, the catheter was removed. Despite treatment with multiple antibiotic regimens and supportive therapy for 4 weeks, his clinical condition worsened and the patient died of septic shock.
Case 2
A 43-year-old man was admitted to the hematology unit for allogeneic bone marrow transplantation for myelodysplastic syndrome on September 2003. Fludarabine chemotherapy was initiated and as his hemoglobin level was 7.7 g/dl, three units of erythrocytes were transfused. He had febrile neutropenia and was started on treatment with cefepime and amikacin as neutropenic fever regimen. He was administered 400 cGy total body irradiation regimen. Hematopoietic stem cell transplantation was performed on October 1, 2003 without additional problems. There was hyperemia around his catheter and intravenous teicoplanin was given for catheter infection on the following day. Blood cultures were taken and MRSA was isolated. Cefepime and amikacin therapy was given when he had neutropenic fever intermittently. He was discharged after resolution of clinical signs on October 2003. He was readmitted to hospital with febrile neutropenia again on December 2003. Intravenous cefepime, amikacin, and acyclovir therapy was administered. After 4 days, he was transferred to the intensive care unit due to the diagnosis of sepsis. Despite broad-spectrum antibiotic and supportive treatment, the patient died as a result of septic shock.
Discussion
In a study evaluating MRSA isolates recovered from blood cultures in Irish hospitals between 1999 and 2003, two MRSA SCVs had been isolated. 12 To our knowledge, this is the first report from Turkey evaluating the prevalence of SCVs among MRSA blood isolates. S. aureus SCV phenotype is usually associated with persistent infections. 8 The prevalence of S. aureus SCVs is found to be higher in CF patients 4 and are independently associated with worse CF respiratory outcomes. 13 We reported recently that the prevalence of SCVs among S. aureus-positive CF patients was 16.2%. 14 Description of an outbreak of MRSA SCVs in an intensive care unit reported that the prognosis was usually worse in patients with MRSA SCVs than those who have MRSA. 9 There are only few case reports of MRSA SCVs in the literature. In the first fatal case due to MRSA SCVs in an AIDS patient, the isolate has been recovered from blood cultures and abscess samples after long-term prophylaxis of TMP-SXT for Pneumocystis jirovecii (carinii) pneumonia. 15 In other two reports MRSA SCVs were identified as the cause of recurrent ventriculoperitoneal shunt-related meningitis and brain abscess, respectively.2,16 It was indicated that MRSA SCVs were identified by using molecular methods in these studies. Proctor et al. described a case of septic arthritis aroused from hip prosthesis that blood cultures revealed MRSA SCVs and persisted for 38 days. 8 The prevalence of MRSA colonization was found in 5%, including seven SCV isolates in a multicenter prospective survey of S. aureus colonization in CF population. 10
We evaluated the presence of SCVs retrospectively among the isolates that had been kept in −80°C and we considered the isolates converting to a normal phenotype after subculturing as reverted SCVs. It could happen that SCVs are induced by cold temperature as indicated in a recent article. 17 Proctor et al. showed that strains that are menadione or hemin auxotrophs were reverted to normal colony forms in the presence of these substances and/or CO2 supplement. 8 A prospective study evaluating clinical CO2-dependent isolates of S. aureus SCVs indicated that all SCVs reverted to a normal morphology after three to six subcultures under anaerobic conditions. 18 As we incubated the subculturing plates on normal atmosphere, we cannot speculate that these revertants may be CO2-dependent S. aureus SCVs. The limitations of the current study are inability for performing auxotrophism tests and molecular confirmation of MRSA SCVs. Identification of S. aureus by testing for the S. aureus-specific nucA gene is well described. 19 The inability to perform minimum inhibitory concentration testing by the broth microdilution method using Brain Heart Infusion Broth is another study limitation. However, identification and antimicrobial susceptibility tests of the isolates have been performed with automated systems in the current study, testing by disk diffusion or by automated methods could be often invalid for S. aureus SCVs. 20
Recently Tuchscherr et al. reported that clinical samples were not stable and the recovered SCVs could rapidly revert to the virulent wild-type form during one subcultivating step in rich medium between 8 and 24 hr. 21 After one or two subculture, four of the isolates reverted to phenotypically normal S. aureus in our study. However, there is not enough data in the literature if the storage in Brain Heart Infusion Broth sufficient to revert the SCVs to the normal phenotype. Onyango et al. reported that exposure of S. aureus to prolonged low temperature induced formation of SCV phenotypes. Upon subculture, SCVs rapidly reverted. 22 In another study, mutation in the major cold-shock gene cspB caused a SCV phenotype. 23 It is not possible for us to define if SCV phenotype induced by cold stress or primary phenotype is maintained by the low temperature in our study. SCVs had not been investigated particularly in routine laboratory practice when MRSA isolates were first obtained.
The microbiological characteristics of S. aureus SCVs were well defined in recent studies.1,4,18,24 As these isolates have uncommon phenotypical features and slow growth, SCVs could be overgrown if normal S. aureus is also present in the specimen. Therefore, they can be easily missed. 25 In our study, both cases had catheter infection after severe clinical conditions like aspiration pneumonia and febrile neutropenia. S. aureus was isolated in both cases, however, a SCV had not been considered as an etiological agent during the isolation period. Probably it was overgrown by the normal S. aureus and overlooked. MRSA SCV identification may have altered the treatment course. Based on in vitro testing, glycopeptides are often considered less active against SCVs.26,27 Furthermore, MRSA SCVs resistant to linezolid or daptomycin were isolated and described as case reports. 28 However, recommendations for differential management of MRSA and MRSA SCVs are not yet been reported and clinical investigations are needed in this area.
The electron transport or thymidine biosynthesis deficiencies may cause the SCV phenotype in S. aureus isolates. 1 The ability to survive intracellularly within nonprofessional phagocytes arises as a result. 29 The deficiencies in SCVs arise from hemB mutation and they are much more resistant to gentamicin compared to the parent strain. 3 Thus, the transformation of S. aureus into a SCV phenotype is attributed to a potent strategy for protecting the bacteria from host defenses and antibiotic effect. 30 S. aureus SCVs have the ability of persisting under antibiotic pressure in vivo. 31 Emergence of SCVs may be induced by the usage of antibiotics such as aminoglycosides and/or trimethoprim–sulfamethoxazole.4,25 S. aureus SCVs may have decreased susceptibility to cell wall-active antibiotics. 8 A stable S. aureus SCV strain within the biofilm has shown to be resistant to the bactericidal action of oxacillin or vancomycin. 26 In vitro exposure to triclosan was reported to select SCVs of MRSA recently and the isolates had reduced susceptibility to penicillin and gentamicin. 32 In our study both isolates were resistant to oxacillin, gentamicin, rifampin, and ciprofloxacin. However, one of the isolates that we tested was susceptible to trimethoprim–sulfamethoxazole, surprisingly. In the previous literature thymidine-dependent S. aureus SCVs have been reported to be resistant to trimethoprim–sulfamethoxazole. 33 Thus, the reason could be that the isolate has no auxotrophism for thymidine, but we did not perform auxotrophism tests in our study.
The clinical characteristics of patients with S. aureus SCVs that were isolated have been reported before.8,18,34 In this study, we described the clinical progress of two patients with MRSA SCVs that were identified. However, the potential relationship between isolates and clinical features were not described as identification of the isolates that were done retrospectively. As the clinical significance of MRSA infections is well documented, evaluation of MRSA SCVs could be done in clinical samples, especially the ones isolated from intensive care patients and those who have chronic and persistent infections.
This first study evaluating MRSA SCVs in Turkey highlighted the need for proper isolation and identification of MRSA SCVs on those who have serious infections. In case of samples sent from patients who received antibiotic treatment for a long period, clinical microbiology laboratories should be particularly attended for S. aureus SCVs and proper methods to detect SCVs should be used. When there is an infection resistant to treatment, persistent, or that is not responding to proper antimicrobial therapy, S. aureus SCVs should be considered. In these situations clinicians should ask the clinical microbiology laboratory to search for S. aureus SCVs. Identification of MRSA SCVs might have an impact on the selection of treatment regimens as MRSA SCVs tend to resist intracellular killing and are more resistant to antibiotics.
Footnotes
Acknowledgments
The authors kindly thank Barbara Kahl for her advice on this article.
Disclosure Statement
No competing financial interests exist.