
Abstract
Plasmid-mediated AmpC β-lactamases (PMACBLs) in Enterobacteriaceae encode resistance to third-generation cephalosporins, and these can mediate carbapenem resistance when associated with porin loss. However, no standardized phenotypic method is available for detecting these enzymes in the clinical microbiology laboratory. Limited data are available concerning the frequency of PMACBLs in Enterobacteriaceae in Brazil. This study was conducted in response to an increased cefoxitin (CFO) resistance rate of 3.7% in Escherichia coli isolates from urine samples from patients with suspected urinary tract infections during 2010. We collected 2,266 E. coli isolates prospectively during January 2012. A total of 109 (4.8%) isolates were nonsusceptible to CFO. These strains were further examined using multiplex PCR for the presence of genes encoding PMACBLs and using inhibitor assays with CFO and ceftazidime (CAZ) disks with and without phenylboronic acid. Pulsed-field gel electrophoresis was used to evaluate clonal dissemination. Genes encoding PMACBLs were detected in 1.8% of the isolates from inpatients and 0.46% of isolates from outpatients. The most prevalent gene was blaCMY-2 and blaCMY-4 was also detected. The phenotypic analysis showed 100% sensitivity and specificity for CMY-2 and CMY-4 when CFO-resistant isolates with a minimum zone diameter difference of 5 mm for CAZ or CAZ and CFO were considered positive. Although most of the isolates were nonclonal, one clonal group with two isolates was observed. Thus, the most frequent PMACBL in E. coli from São Paulo, Brazil is CMY-2, and both clonal and plasmid-mediated dissemination occur.
Introduction
I
AMC, amoxicillin-clavulanic acid; APBA, 3-aminophenylboronic acid; CA, clavulanic acid; CAZ, ceftazidime; CLOX, cloxacillin; CPD, cefpodoxime; CRO, ceftriaxone; CTT, cefotetan; CTX, cefotaxime; EDTA, ethylenediamine tetraacetic acid; CFO, cefoxitin; PBA, phenylboronic acid; PTZ, piperacillin-tazobactam; SN, sensitivity; SP, specificity.
In Brazil only two reports of PMACBL detection in E. coli are available.2,31 One of these studies was undertaken in Rio de Janeiro to evaluate E. coli strains collected from chicken carcasses from August 2010 to April 2011 and the authors reported the detection of the blaCMY-2 gene in 19 isolates. 2 The other study was conducted in São Paulo, and described the detection of carbapenem-resistant isolates. 31 In both studies only a 462 bp fragment of a 1,146 bp gene was sequenced and frequency was not calculated.
There is one report of blaCMY-2-like detection in Salmonella enterica 32 and one publication from São Paulo describing a Klebsiella pneumoniae strain producing a CMY-2-like enzyme, 4 but none of these publications determined the full blaCMY gene sequence. There was also a prevalence study that was not successful in finding PMACBLs in clinical isolates from patients at a university hospital located in the city of Rio de Janeiro. 12
This study was prompted by an analysis of the susceptibility profiles of E. coli isolates from patients attending a large private laboratory in São Paulo, the largest city in Latin America. From January 2006 to December 2010, a sustained increase in the frequency of CFO-resistant E. coli was observed. While that rate was 0.03% among 91,400 E. coli isolates from 2006 to 2007, the rates were 0.35%, 0.70%, and 0.65%, in 2008, 2009, and 2010, respectively. Among all clinical samples tested, the highest CFO resistance rate 3.7% in 2010 was observed among E. coli isolates cultured from urine samples collected from patients with suspected urinary tract infections. Because no methodological changes were implemented, the main hypothesis for the cause of this increase was the spread of clones or genes located in transposons or integrons through transfer on plasmids. The objectives of this study were to determine the relative frequency of PMACBLs among E. coli isolates from urine samples from patients with suspected urinary tract infections, to evaluate a possible phenylboronic acid (PBA)-based phenotypic confirmatory test for PMACBLs using multiplex PCR and DNA sequencing as the gold standard and to evaluate the occurrence of clonal dissemination.
Materials and Methods
Bacterial strains
From January 2nd to February 1st 2012, a total of 2,266 urine cultures, one per patient, were positive for E. coli at a large private laboratory from São Paulo, Brazil. Among these, 2,153 cultures were obtained from outpatients and 113 were obtained from inpatients admitted to seven different private hospitals. Among the 2,266 E. coli isolates, 109 isolates (4.8%) were intermediate or resistant to CFO, as determined using the Vitek2 system (bioMérieux), and were included in this study. Species identification was achieved through the production of pink colonies on ChromID CPS agar (bioMérieux) and through mass spectrometry using the Vitek MS system (bioMérieux).
PMACBL detection using the disk diffusion method
Enzyme blocking was evaluated after adding PBA (Sigma-Aldrich) to 30 μg CAZ and CFO disks (Oxoid). The PBA solution was prepared after dissolving 240 mg of PBA in 3 ml of DMSO, followed by the addition of an equal volume of reagent-grade water. The disks were prepared immediately before use by adding 10 μl of PBA solution. A bacterial suspension with a turbidity equivalent to 0.5 McFarland standard was prepared from cultures incubated for 18–24 hr and plated on Mueller–Hinton agar (Becton-Dickinson). After the evaporation of excess suspension, CFO and CAZ disks with and without PBA were applied. After 18–24 hr of incubation at 36°C ± 1°C, the diameters of the inhibition zones were measured, and the differences between the values were calculated. Susceptibility to CFO, ertapenem, imipenem, and meropenem were evaluated by disk diffusion in accordance with the Clinical and Laboratory Standards Institute.6,7
Detection of genes encoding PMACBLs using multiplex PCR
Multiplex PCR reactions were performed as previously described, 11 except primers rrs27FW 5′ AGAGTTTGATYMTGGCTCAG and rrs1492RV 5′ GGTTACCTTGTTACGACTT 24 were included at a final concentration of 0.2 μM to target the 16S rRNA genes as an internal control in each reaction, and Platinum® Taq DNA polymerase (Invitrogen) was used. Hafnia alvei C4171841, Aeromonas caviae 82251942, Morganella morganii D4141434, Citrobacter freundii D4042263, and Enterobacter asburie D4040536 were used as controls for the detection of genes encoding ACC, MOX, DHA, CMY, and LAT or the ACT and MIR enzymes, respectively. The FOX-1 E. coli control strain for genes encoding FOX enzymes was kindly provided by Dr. Ana Gales.
Pulsed-field gel electrophoresis
The pulsed-field gel electrophoresis (PFGE) was performed as described previously, with minor modifications. 34 The plugs were cut in half, placed into a 96-well microdilution plate containing 200 μl of 1X enzyme buffer, and incubated for 30 min at room temperature, followed by digestion with 3 μl of Xbal (Invitrogen) for 4 hr at 36°C ± 1°C.
The plugs and the size marker lambda phage concatamers (NewEngland Biolabs) were loaded onto a 1% agarose gel. Electrophoresis was carried out in a CHEF-DR III system with a 5 sec initial pulse and a 35 sec final pulse; a 19 hr run time and 6 V/cm2 voltage at a 120° angle. After the run, the agarose gel was stained with GelRed for 30 min and visualized under ultraviolet light. The profiles were compared using BioNumerics software version 6.0 (Applied Maths) with the UPGMA method to calculate Dice's similarity index with 1% tolerance and optimization. Strains were defined as having a clonal relationship if their profiles possessed a minimum similarity index of 85%. 14 The profiles were also compared visually and classified according to Tenover's criteria. 37
Two epidemiologically unrelated E. coli strains (C1101689 and C1210549) were included as controls.
Full PMACBL genes sequencing
Genomic DNA was extracted from 18 to 24 hr cultures using the Illustra Bacteria Genomic Prep Mini Spin Kit® (GE Healthcare). One microliter of DNA solution was added to a 50 μl PCR reaction containing 1X PCR buffer (150 mM Tris- HCl and 500 mM KCl, pH 8.0), 0.2 mM of each deoxynucleotide, 1.5 mM MgCl2, 0.16 mM of each primer, and 1 U of Platinum Taq DNA polymerase (Invitrogen). The primers pairs used in this study were published previously (ISEcp1-3′-cmy-F-c 5′AAAAATGATTGAAAGGTGGT and CIT-MR-cmy-rv-d 5′TTTCTCCTGAACGTGGCTGGC 27 ) or designed for this study using the Primer-BLAST program and GenBank deposit number AY58120716: JS-cmy-blc-F 5′GCGGTGAAACCCTCAGGAAT and JS-blc-cmy-RV 5′AACCAGGAATGCAGCCGTAA; JS-cmy-blc-F2 5′CCAGCATTGGTCTGTTTGGC and JS-blc-cmy-RV2 5′TCGCCGGTGAAATAGGCTTT; JS-CMY-2-1-25-FW 5′ATGATGAAAAAATCGWTATGCTGCCG and JS-CMY-2-1139-20-RV 5′AGCTTTTCAAGAATGCGCCA. Amplifications were performed with a single cycle of 3 min at 94°C, followed by 35 amplification cycles consisting of 30 sec at 94°C, 30 sec at 55°C, 1 min at 72°C, and a final extension for 7 min at 72°C. The amplicons were purified using the GFX PCR DNA and Gel Band Purification Kit (GE Healthcare) and sequenced using the same primers and the BigDye Terminator version 3.1 Cycle Sequencing kit (Applied Biosystems®) in a 3130xl Genetic Analyzer (Applied Biosystems). The contigs were assembled using SeqMan Pro version 8.1 (DNAStar) and subsequently translated and compared with the sequences available in GenBank using the BLAST program.
Results
Frequency of genes encoding PMACBLs
When the 109 isolates that were not susceptible to CFO were examined using multiplex PCR, 12 isolates had amplification products with an estimated size of 538 bp, which is compatible with the blaCMY-2-like or blaLAT genes. In all other isolates tested, only amplicons of ∼1,492 bp (16S rRNA gene) were observed. Two isolates were obtained from inpatients and 10 isolates were obtained from outpatients. Considering the total number of 2,153 outpatients and 113 inpatients, the frequency of genes encoding PMACBLs was 0.46% in E. coli isolates from outpatients and 1.8% in E. coli isolates from inpatients. When the DNA sequences were translated and compared with the sequences available in GenBank, 11 isolates were confirmed to have the blaCMY-2 gene, while the blaCMY-4 gene was detected in only one isolate (C1310573). Two DNA sequences, one for blaCMY-2 and one for blaCMY-4, were deposited at GenBank under accession numbers KJ488945.1 and KJ496347.1, respectively.
The best sensitivity and specificity for CMY-2 and CMY-4 detection are achieved using CFO resistance as a screening method in combination with CAZ disks with PBA
All 109 isolates that were classified as not susceptible to CFO by the Vitek2 system were examined via disk diffusion using CFO and CAZ disks with and without PBA. A total of 32 CFO-intermediate isolates and 11 CFO-resistant isolates, as determined by the Vitek2 system, were found to be susceptible by disk diffusion. All of these isolates were negative when tested using multiplex PCR. Seven isolates (6.4%), one resistant, three intermediate and three susceptible to CFO by disk diffusion, were found to be negative for PCR and have an inhibition zone diameter enhancement ≥5 mm with CFO with added PBA (Table 2). These isolates were considered to have upregulation of the chromosomally encoded AmpC. Using PCR as the gold standard for PMACBL detection, the best sensitivity, specificity, negative predictive, and positive predictive values (100%) were achieved by combining CFO resistance (inhibition zone diameter ≤14 mm) with an inhibition zone enhancement ≥5 mm after the addition of PBA solution to 30 μg CAZ disks (Table 1). Using CFO resistance and an inhibition zone enhancement ≥5 mm after the addition of PBA solution to 30 μg CFO disks as the criteria to identify CMY-2 and CMY-4 resulted in 95.0% specificity (Table 2). All 109 isolates were susceptible to carbapenems.
PMACBL, plasmid-mediated AmpC β-lactamases. ≥5 mm and <5 mm refer to inhibition zone diameter differences when comparing results obtained with and without addition of PBA.
All (n = 109) refers to the isolates that were nonsusceptible to CFO by Vitek2 testing.
PMACBL dissemination in São Paulo, Brazil, occurs by both clonal spread and plasmid dissemination
Most patients infected with AmpC-producing E. coli were female (83%), but this proportion was similar to that observed for the whole population studied (91%). Patient age ranged from 4 to 100 years with a median of 69 years (Fig. 1). All PMACBL-producing E. coli were evaluated by PFGE. When the profiles were compared, most of the isolates had a Dice's index below 85% and had seven or more band differences and were consequently interpreted as unrelated. One clonal group with two isolates with a 94.4% similarity index and a single band difference was detected. Of note, those isolates were isolated from patients in home care who had previous admissions to different hospitals (Fig. 1).
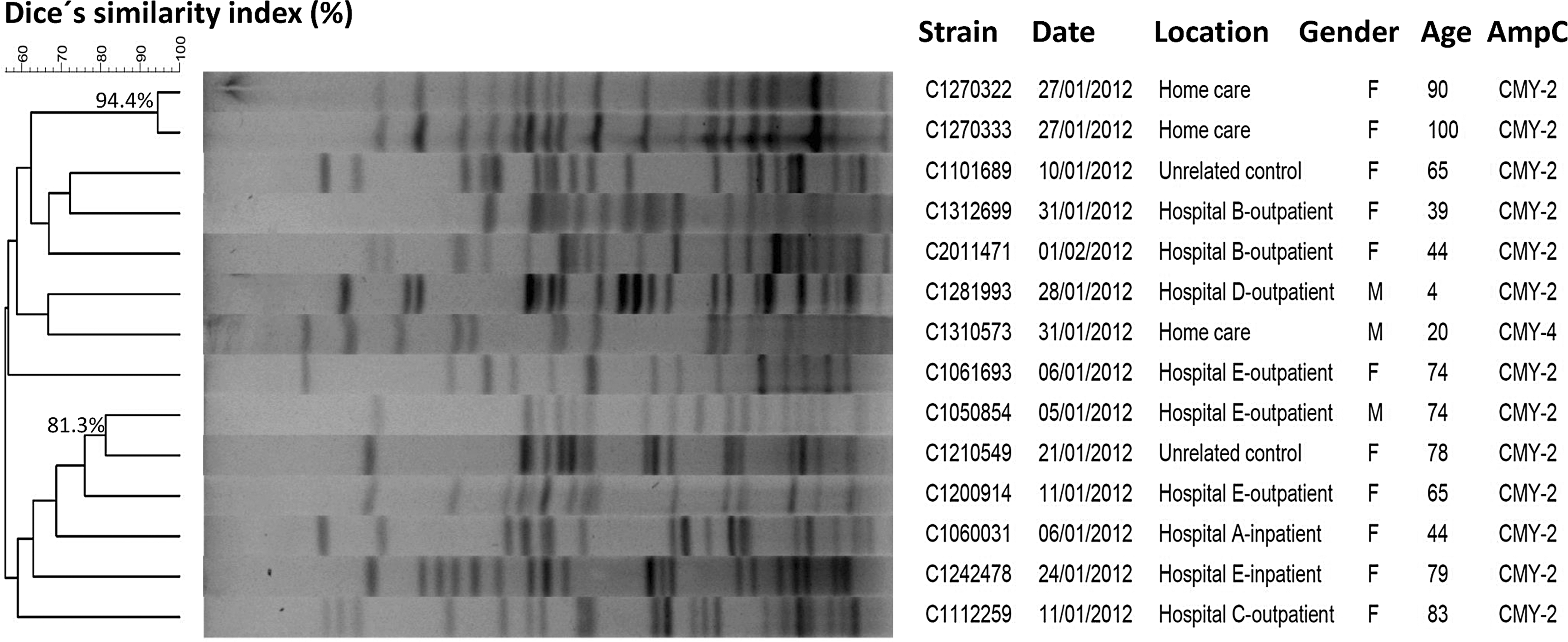
Pulsed-field gel electrophoresis profile of CMY-producing Escherichia coli after digestion with XbaI. Patient age is expressed in years.
Discussion
In this study, we detected a frequency of 0.46% for PMACBL production in E. coli isolates from urine samples from outpatients with suspected urinary tract infections and a frequency of 1.8% in E. coli isolates from inpatients from São Paulo, Brazil. In contrast, the frequency of ESBL-producing E. coli was 3.5% in samples from outpatients and 6.9% in samples from inpatients, as detected by the Vitek2.
The difference between the PMACBL frequencies observed in this study and those previously reported in Brazilian studies4,12 (0% and 0.75%) likely reflect the differences between samples. Notably, in the study that was performed in Rio de Janeiro, 12 only 42 E. coli isolates from various clinical samples were studied, in contrast with this study, in which only isolates from urine samples were analyzed. In addition, in the study performed in São Paulo, the frequency refers to all Enterobacteriaceae species cultured from blood cultures. 4
The frequencies of PMACBLs obtained in this study are lower than those reported in other countries in Latin America. Cejas et al. 5 reported that 0.9% of E. coli produce CMY-2 in Argentina, while Leal el al. 22 reported that 2.7% of E. coli isolated from urine samples produce PMACBL in Colombia, and Marcano et al. 26 reported that 4.3% of Enterobacteriaceae produce PMACBL in Venezuela. The differences between this study and the available data from Latin America may reflect the samples analyzed and the microorganisms evaluated. Cejas et al. 5 not only identified PMACBLs in isolates from urine samples but also used isolates cultured from other biological fluids and blood from nosocomial and community-acquired infections, whereas Leal et al. 22 used urine samples from patients with pyelonephritis and Marcano et al. 26 used enterobacterial isolates from various infection sites.
An extensive review that included population studies of PMACBL was published by George Jacoby in 200920 and revealed a wide range of frequency values among E. coli isolates throughout the world, with values ranging from 0.09% in Canadian hospitals from 1999 to 200028 to 49% in London from 2004 to 2006. 38
More recently, Denisuik et al. 13 examined a total of 5,451 E. coli isolates obtained from patients in Canadian hospitals, and the frequency of PMACBL producers was 2.9%. Ortega et al. 30 conducted a multicenter study in Spain screening for PMACBLs in E. coli through the expression of resistance to amoxicillin/clavulanic acid. Among the 257 isolates resistant to amoxicillin/clavulanic acid, 19.5% produced these enzymes. The most frequently detected enzymes were blaCMY-2, blaDHA-1, blaCMY-30, and blaCMY-42. Yilmaz et al. 40 conducted a study with 191 E. coli isolates in India, in which the isolates were screened using CFO disks with PBA, and the results were confirmed using multiplex PCR assays. The frequency of PMACBL-producing E. coli was 10.9%. In this study, we used PBA to detect PMACBLs in E. coli isolates susceptible to carbapenems. The main limitation for the detection of PMACBLs in E. coli using PBA or CLOX is the generation of false positive results when E. coli isolates express chromosome-encoded AmpCs; consequently, there is a need to confirm the presence of PMACBLs by PCR. Considering that a high sensitivity and specificity are desirable for diagnostic methods, phenotypic tests were compared with the results obtained using PCR. The best correlation with PCR results was obtained with a combination of resistance to CFO and a difference in inhibition zones between CAZ or CFO and CAZ disks with and without PBA ≥5 mm, leading to high sensitivity and specificity, with positive and negative predictive values of 100%.
Tan et al. 36 found a 94% sensitivity for the detection of PMABLs using CFO disks with added PBA and interpreting as positive those isolates with an inhibition zone diameter ≥4 mm. These results differ from those obtained in this study probably due to the fact that Tan et al. evaluated E. coli, K. pneumoniae, and Proteus mirabilis as a single group, while we determined these values for E. coli alone. Black et al. 1 found 100% sensitivity for PMACBL in a collection of E. coli and K. pneumoniae strains known to produce ACT, FOX, CMY, DHA, MIR, or MOX enzymes, but they used CFO disks with new inhibitors 48-1220 and LN-2-128.
In this work we detected seven isolates (6.4%) with an inhibition zone diameter enhancement ≥5 mm with CFO with added PBA and with a negative PCR result, which were considered to have chromosomally upregulated AmpC. Sequencing of the ampC promoter/attenuator region 8 would confirm the presence of mutations but was not performed in this study or in the studies conducted by Tan et al. 36 and Black et al. 1 Consequently, our findings concerning specificity of the test for PMACBL detection, as the published data, are of limited value.
Although we analyzed a large number of E. coli isolates (∼2,266 strains), one limitation of this study is the initial screening using CFO, as ACC-1, a PMACBL, cannot hydrolyze this antimicrobial; however, we also included isolates intermediate for CFO. An alternative to the initial screening for PMACBLs that would also detect ACC enzymes is nonsusceptibility to amoxicillin/clavulanic acid. 15
The presence of one clonal group was observed using PFGE. The strains that exhibited a clonal relationship were isolated from elderly patients in home care. These patients require hospital care more often; one explanation for finding the same clone in patients from different institutions could be the movement of elderly patients among different hospitals and homecare facilities. Our findings are in accordance with previous publications that reported PMACBL-producing E. coli in elderly patients 17 and clonal dissemination in rehabilitation centers. 19 Our finding that only 2 of 12 isolates had a clonal relation, suggests that AmpC dissemination among E. coli in the city of São Paulo occurs mainly via horizontal plasmid transfer.
In summary, we provided a description of the relative frequency of PMACBLs in Brazil and showed that CMY-2 is the most frequently occurring enzyme in E. coli isolates from urine samples from patients with suspected urinary tract infection. This is the first report from Brazil to determine full blaCMY gene nucleotide sequences. We also demonstrated that clonal dissemination is not the main mechanism of dissemination for PMACBLs in São Paulo. Our results also indicated that using CFO resistance as an initial screening method in combination with CAZ or CAZ and CFO disks with PBA can accurately detect the CMY-2 and CMY-4 enzymes.
Footnotes
Acknowledgments
This work was financially supported by grants from the Fleury Institute and CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior).
Author Disclosure Statement
No competing financial interests exist.