
Abstract
The increasing prevalence of infections due to multidrug-resistant (MDR) gram-negative bacteria constitutes a serious threat to global public health due to the limited treatment options available and the historically slow pace of development of new antimicrobial agents. Infections due to MDR strains are associated with increased morbidity and mortality and prolonged hospitalization, which translates to a significant burden on healthcare systems. In particular, MDR strains of Enterobacteriaceae (especially Klebsiella pneumoniae and Escherichia coli), Pseudomonas aeruginosa, and Acinetobacter baumannii have emerged as particularly serious concerns. In the United States, MDR strains of these organisms have been reported from hospitals throughout the country and are not limited to a small subset of hospitals. Factors that have contributed to the persistence and spread of MDR gram-negative bacteria include the following: overuse of existing antimicrobial agents, which has led to the development of adaptive resistance mechanisms by bacteria; a lack of good antimicrobial stewardship such that use of multiple broad-spectrum agents has helped perpetuate the cycle of increasing resistance; and a lack of good infection control practices. The rising prevalence of infections due to MDR gram-negative bacteria presents a significant dilemma in selecting empiric antimicrobial therapy in seriously ill hospitalized patients. A prudent initial strategy is to initiate treatment with a broad-spectrum regimen pending the availability of microbiological results allowing for targeted or narrowing of therapy. Empiric therapy with newer agents that exhibit good activity against MDR gram-negative bacterial strains such as tigecycline, ceftolozane-tazobactam, ceftazidime–avibactam, and others in the development pipeline offer promising alternatives to existing agents.
Introduction
I
Adapted from Centers for Disease Control and Prevention. 25
BSIs, bloodstream infections; CRE, carbapenem-resistant Enterobacteriaceae; MDR, multidrug resistant.
The objective of this article is to review the epidemiology of MDR gram-negative infections in the United States, their consequences for patients and healthcare systems generally, and the implications for treatment of patients hospitalized due to various infections commonly caused by gram-negative organisms. Newer, recently approved antimicrobial agents and compounds in the late-phase development that are potentially of value in treating MDR gram-negative infections are also reviewed.
Mechanisms of Resistance: An Overview
Mechanisms involved in the development of antimicrobial resistance may be intrinsic, acquired, or adaptive. 46 Intrinsic resistance arises from the characteristics of a particular microorganism such as the possession of an outer membrane with low permeability and constitutive efflux pumps for excluding antimicrobial agents.5,46,83 Acquired mechanisms result from the incorporation of new genetic material such as plasmids, transposons, integrons, and naked DNA by microbes that were originally susceptible to antimicrobial agents, while adaptive mechanisms involve an increased ability of bacteria to resist the antimicrobial activity as a result of alterations in gene and/or protein expression due to prior exposure to an environmental trigger or subinhibitory concentrations of antimicrobial drugs. 46 Adaptive resistance mechanisms may be either plasmid mediated or chromosomally mediated and their location on transferrable genetic elements facilitates their spread to other bacteria of the same or different species.72,79
The most common resistance mechanisms employed by gram-negative bacteria are illustrated in Fig. 1 and include the production of various inactivating lactamase enzymes, decreased influx of antimicrobial agents into the organism due to a reduction in the number of protein entry channels (porins) that facilitate their uptake, and enhanced efflux of antimicrobial agents due to increased expression of cytoplasmic efflux pumps.46,65,79,84,151 -Lactamase enzymes are classified according to their molecular structure using the Ambler classification method. 8 Kanj and Kanafani provide a comprehensive review of the Ambler β–lactam classification system, including Ambler class A enzymes (e.g., TEM- and sulfhydryl variable [SHV]-type broad-spectrum β-lactamases, extended-spectrum β-lactamases [ESBLs] of the TEM, SHV, and cefotaximase [CTX-M] types, and Klebsiella pneumoniae carbapenemase [KPC]); Ambler class B enzymes (e.g., New Delhi metallo-β-lactamase [MBL]); Ambler class C enzymes (e.g., AmpC cephamycinases); and Ambler class D enzymes (e.g., oxacillinase [OXA]-type ESBLs and carbapenemases).65,110,114
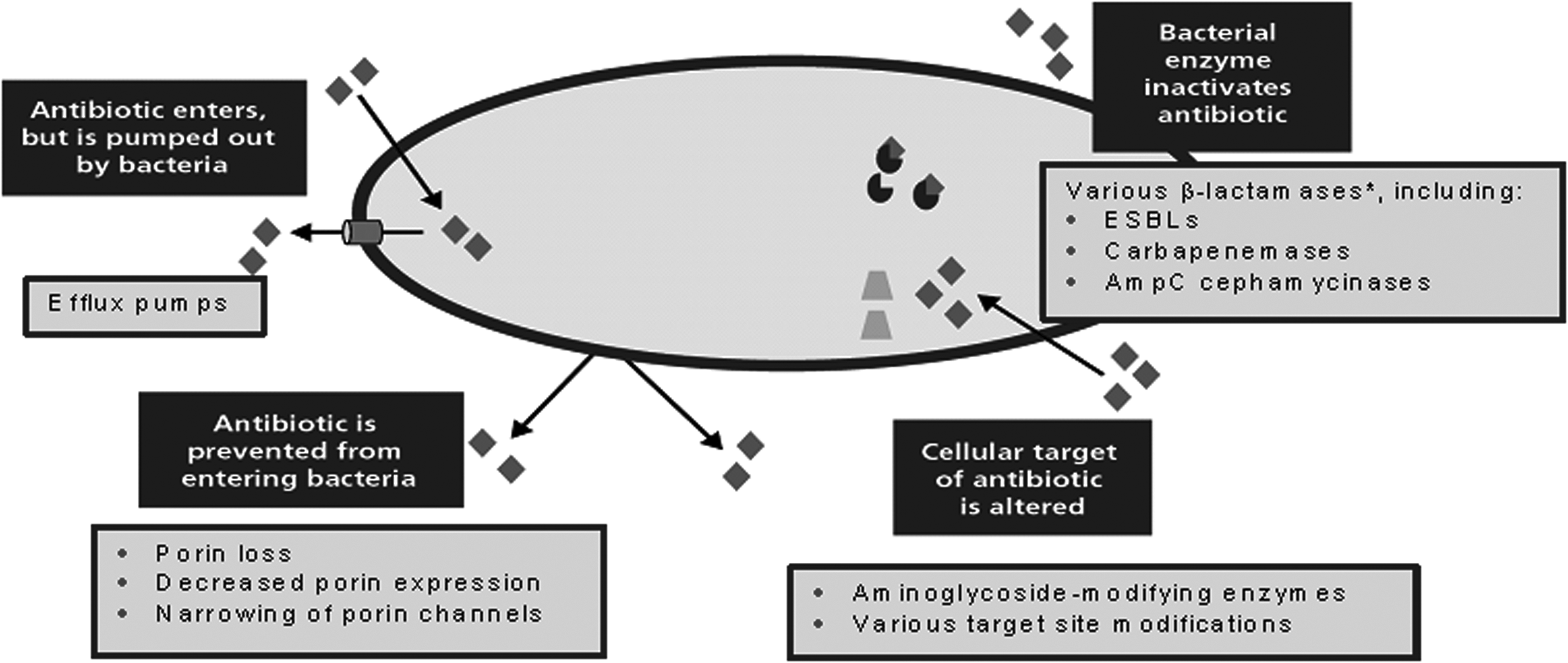
Common resistance mechanisms employed by gram-negative bacteria. *See text for other inactivating β-lactamases. ESBL, extended-spectrum β-lactamase.
Epidemiology of MDR Gram-Negative Infections
Evidence suggests that the prevalence of MDR gram-negative bacteria is increasing worldwide.47,64,107,125,137 Numerous risk factors can increase the likelihood of infection with resistant organisms, including: (1) prior antimicrobial therapy, especially with a broad-spectrum agent, in the preceding 90 days; (2) current hospitalization for 5 days; (3) a high prevalence of resistant organisms in a hospital environment; (4) immunosuppressive therapy; and (5) specific risk factors such as hospitalization for 2 days in the preceding 90 days, residence in a nursing home or long-term care facility, chronic dialysis within the preceding 30 days, home wound care or intravenous infusion therapy, and a family member with a resistant pathogen (Table 2). 9 Currently, there is a move to weigh some individual factors differently to others, and ongoing investigations are evaluating which factors place patients at greatest risk. In a recent study of risk factors associated with MDR pathogens in hospitalized patients, 20 age >60 years, a Karnofsky score <70, hospitalization in the past year, and recent antimicrobial therapy were identified as major risk factors.
Gram-negative organisms frequently associated with antimicrobial drug resistance include Klebsiella pneumoniae, Escherichia coli, Pseudomonas aeruginosa, Proteus mirabilis, Acinetobacter baumannii, and Enterobacter spp.16,22,49,64,75 In particular, ESBL- and KPC-producing Enterobacteriaceae and MDR strains of P. aeruginosa and A. baumannii have emerged as particularly serious concerns.21,25
Among these organisms, K. pneumoniae, which is one of the most frequently isolated organisms in intensive care unit (ICU) infections, has become the most common carbapenem-resistant bacterium in the United States. 121
Data reported to the National Healthcare Safety Networks at the CDC in the United States during the 2-year period (2009–2010) indicated that nearly 20% of the pathogens from all reported healthcare-associated infections were MDR phenotypes, including extended-spectrum cephalosporin-resistant K. pneumoniae and Klebsiella oxytoca (2%), E. coli (2%) and Enterobacter spp. (2%), and carbapenem-resistant P. aeruginosa (2%), K. pneumoniae/oxytoca (<1%), E. coli (<1%), and Enterobacter spp. (<1%). 125 MDR gram-negative pathogens have been reported from hospitals throughout the United States and are not limited to a small subset of hospitals. 125 A study of the frequency of ESBL phenotypes among Enterobacteriaceae identified in 72 US hospitals in 2012 found that among 5,739 isolates of E. coli, Klebsiella spp., and P. mirabilis, the national prevalence of ESBL phenotypes was 12.2%. 22 The organism with the highest prevalence of ESBL phenotypes was K. pneumoniae (16.0% compared with 11.9% for E. coli isolates, 10.0% for K. oxytoca, and 4.8% for P. mirabilis), and the regions with the highest prevalences of ESBL phenotypes among Enterobacteriaceae were the Mid-Atlantic (23.2%), South Atlantic (19.9%), and West South Central (16.2%) regions, while the West North Central region (4.4%) had the lowest (Table 3). 22
Data from Castanheira et al. 22
All isolates of E. coli, Klebsiella spp., and P. mirabilis collected.
ESBL, extended-spectrum β-lactamase.
ESBL-producing E. coli have also been found to be common in community settings in the United States. A study undertaken in 2009 and 2010 reported that more than a third of community-onset ESBL-producing E. coli isolates reported by five US academic and community hospitals and their affiliated clinics occurred in patients with no discernible healthcare-associated risk factors and were epidemiologically defined as community associated. 38 In a US hospital-based study that analyzed data reported by 2,039 hospitals to the National Healthcare Safety Network in 2009–2010, carbapenem resistance among Klebsiella spp. and E. coli was observed in 12.5% and 2.3%, respectively, of catheter-associated urinary tract infections (UTIs), and 12.8% and 1.9%, respectively, of central line-associated bloodstream infections (BSIs). 125 Percentages of resistant strains among other gram-negative organisms to carbapenem antimicrobials, third- or fourth-generation cephalosporins, and fluoroquinolones recorded in this study are shown in Table 4.
Data from Sievert et al. 125
CAUTI, catheter-associated urinary tract infection; CLABSI, central line-associated bloodstream infection; UTIs, urinary tract infections.
A 10-year study that analyzed microbiology data from 217 US hospitals over the period 2000–2009 noted that the prevalence of MDR P. aeruginosa isolates (i.e., those resistant to three drug classes) was ∼15% higher compared with carbapenem-resistant Enterobacteriaceae (CRE) isolates in both pneumonias and BSIs. 154 Over the 10-year period of this study, there was a net rise in the prevalence of MDR P. aeruginosa as a percentage of all P. aeruginosa isolates in both types of infections. In the case of pneumonias, the rise was from 19.2% in 2000 to 21.7% in 2009, while for BSIs it was from 10.7% in 2000 to 13.5% in 2009. 154
Data from the Study for Monitoring Antimicrobial Resistance Trends (SMART) surveillance program have shown that the global incidence of ESBL-producing isolates of E. coli increased from 9.2% in 2002 to 21.2% in 2010. 59 Some ESBLs and carbapenemases have become associated with bacterial strains that exhibit important epidemic spread and are potentially capable of spreading across countries and continents. 84 In 2001, K. pneumoniae strain 11978 was isolated in Turkey with an OXA-48 class D carbapenemase, 112 a -lactamase usually found in A. baumannii. Among strains of A. baumannii, carbapenem (doripenem) resistance rates have been reported to be increasing in Europe as well as the United States; in 2011, more than 50% of isolates in ≥4 European countries (Italy, Greece, Spain, and Portugal) were resistant. 21 In Southeast Asia (Cambodia), a study of patients with BSIs hospitalized between 2007 and 2010 found that 49.7% of Enterobacteriaceae isolates (91 of 183) were cefotaxime resistant and ESBLs were present in 97.8% of these isolates. 144
Consequences of the Increasing Prevalence of MDR Gram-Negative Infections
Increasing rates of resistance among gram-negative bacteria to multiple commonly prescribed antimicrobial agents have generated concerns about therapeutic options to treat these infections, 107 particularly as the rate of development of new antimicrobial drugs to combat the threat they pose has been slow in the past. 16 This has been reflected in considerable mortality rates among patients with resistant gram-negative infections, for example, among those with infections due to CRE (notably K. pneumoniae and E. coli) in whom mortality rates are twofold higher than among patients with infections due to carbapenem-susceptible Enterobacteriaceae. 44 In 2013, the CDC estimated that more than 2 million illnesses in the United States were attributable to antimicrobial drug resistance, and there were 23,000 deaths. Among patients with healthcare-associated infections due to MDR strains of Acinetobacter spp., ESBL-producing Enterobacteriaceae, and P. aeruginosa, mortality rates ranged from 6.5% to 6.8%. 25
In addition to increased mortality rates, MDR gram-negative infections are also associated with a higher economic burden due to their greater severity and increased resource utilization, for example, longer hospital/ICU stays and increased hospital and antimicrobial therapy costs in comparison with patients with infections due to antimicrobial-susceptible organisms.42,77,94,98 Costs associated with multidrug resistance are substantial and result not only from direct treatment costs but also increased lengths of hospital stay (Fig. 2). 127 Recently, the Obama Administration announced plans to provide funding of up to US $1.2 billion for a multipronged approach to combat antimicrobial resistance with a focus on the development of new antimicrobials, new diagnostic tests, and improved surveillance, including the creation of new bacterial DNA databanks and requirements for hospital tracking and reporting of antimicrobial drug use. 139 The Administration also pledged to decrease the widespread use of antimicrobials to boost growth in animals raised for meat production. Although the US Food and Drug Administration (FDA) has recommended similar measures in the past, livestock producers were not required to comply. New changes would make it illegal to sell antimicrobials to livestock producers without a veterinarian's prescription.

Influence of multidrug resistance on the
Factors That Have Contributed to the Increased Antimicrobial Drug Resistance Among Gram-Negative Bacteria
Factors that have contributed to the persistence and spread of MDR gram-negative bacteria include the following: (1) overuse of existing antimicrobial agents in the community, which has led to the development of adaptive resistance mechanisms by bacteria; (2) the lack of good antimicrobial stewardship such that use of multiple broad-spectrum agents has helped perpetuate the cycle of increasing resistance; (3) the lack of good infection control practices; and (4) a dearth of novel antimicrobial agents being approved in the last decade.69,72 Unregulated antimicrobial drug use in veterinary medicine and animal husbandry has also had a significant impact on the development of resistance. About 80% of antimicrobial drugs sold in the United States are used in food animals. 24 Many of our current medical practices and treatments directly contribute to increases in infections overall, including increased use of prophylactic antimicrobials (which increases the risk of resistance), more invasive procedures, increased use of vascular access and other devices, and more immunosuppression for oncologic and rheumatologic conditions.
The development of adaptive resistance mechanisms by certain bacterial strains has resulted in the spread of resistance genes between bacteria of the same or even different species.72,79 Adaptive resistance mechanisms of growing importance among gram-negative organisms include production of the CTX-M family of ESBLs, plasmid-mediated AmpC -lactamases and K. pneumoniae carbapenemases in Enterobacteriaceae, and OXA- and metallo-carbapenemases in Acinetobacter spp. 88 In the case of P. aeruginosa and A. baumannii, resistance to multiple drugs is usually due to a combination of -lactamase production, an increased efflux pump activity, and outer membrane modifications, or to a single potent mechanism. 151 P. aeruginosa, which has decreased susceptibility to most antimicrobials due to low outer membrane permeability, has demonstrated an ability to rapidly mutate and adapt to changing environmental conditions and stresses, which leads to the development of phenotypes that are resistant to multiple classes of antimicrobial drugs.17,82
Implications for Clinical Practice in Hospitals
The dilemma for clinicians: which hammer to hit what nail?
The increasing prevalence of MDR gram-negative bacteria poses a therapeutic challenge for clinicians managing seriously ill patients hospitalized with acute infections because the potential presence of these organisms increases the likelihood that inappropriate initial antimicrobial therapy will lead to treatment failures, adverse patient outcomes, and increased healthcare costs. In this regard, overuse of empiric broad-spectrum antimicrobial drugs in an attempt to avoid adverse patient outcomes may have the undesired effect of increasing the likelihood of antimicrobial drug resistance. 69
In individual patients hospitalized with acute infections, the overriding principal of management is timely administration of optimal antimicrobial therapy to achieve a satisfactory outcome and decrease the risk of morbidity and mortality, while minimizing the likelihood of developing resistance. 69 Ideally, cultures should be obtained from patients before starting antimicrobial treatment (see CDC guide to collecting cultures 27 and antimicrobial susceptibilities tested by the Clinical and Laboratory Standards Institute [CLSI]-recommended procedures 32 ), but it may not be possible to delay treatment while awaiting the culture results in seriously ill patients. If treatment needs to be started before the results of susceptibility testing are known, current recommendations for initial management of patients with acute infections suspected to be due to gram-negative organisms include the following: (1) consideration of the underlying disease (i.e., its severity and whether it is a type of infection in which MDR gram-negative bacteria are likely); (2) establishing whether the patient has had any previous bacterial colonizations (the treatment of which may have increased the likelihood of resistant organisms); (3) ascertaining hospital-specific antimicrobial resistance trends; and (4) early administration of empiric antimicrobial therapy based on these considerations, which can be subsequently tailored when susceptibility results are available.69,72,78
Depending on the suspected causative organism, an appropriate empiric regimen in an individual patient may include the combination of a broad-spectrum or antipseudomonal cephalosporin plus an aminoglycoside, a -lactam/-lactamase inhibitor combination agent an aminoglycoside, or a carbapenem an aminoglycoside 72 ; once susceptibility results are available, the treatment regimen can then be narrowed. Although combination regimens may lead to increased costs and adverse drug effects, the rationale for using a combination regimen initially is, first, to utilize the potential for synergism between two drugs; second, to prevent or delay the emergence of resistance; and third, to broaden the antimicrobial coverage when the risk of MDR organisms is high by using two drugs that have different mechanisms of action and different mechanisms by which resistance may occur.65,138 However, when selecting empiric therapy in an individual patient, outbreaks of resistance to individual drug classes need to be borne in mind, for example, the recently reported outbreaks of CRE.44,129 This is a significant concern as increasing use of carbapenem-based regimens as first-line therapy could lead to the emergence and spread of CRE, for which there are limited effective treatment options.
Consideration can also be given to the use of newer agents when selecting empiric antimicrobial therapy for a patient in whom MDR gram-negative bacteria are suspected, for example, using one of the newer -lactam/-lactamase inhibitor combinations to combat resistance due to -lactamase-producing organisms. Two newer -lactam/-lactamase inhibitor combinations that may offer additional therapeutic options in patients with suspected MDR gram-negative infections are the broad-spectrum antipseudomonal cephalosporin ceftolozane in combination with the well-established -lactamase inhibitor tazobactam and the broad-spectrum antipseudomonal cephalosporin ceftazidime in combination with the novel non–-lactam/-lactamase inhibitor avibactam, although clinical experience with these newer -lactam/-lactamase inhibitor combinations is currently limited. Alternatively, a second-line agent such as tigecycline (which has an activity against several MDR gram-negative organisms), minocycline (which is active against A. baumannii), or one of the older polymyxin drugs (e.g., polymyxin B or colistin) could be considered. 72 The polymyxins have been little used in the past due to their neuro- and nephrotoxicities, but have returned to clinical practice in recent years due to the increased incidence of pathogens resistant to other antimicrobial agents. 47 Although there is a lack of adequate pharmacokinetic/pharmacodynamic data to guide their dosing in target organ infections, these drugs are active against many gram-negative organisms, including P. aeruginosa, A. baumannii, Klebsiella spp., and E. coli,43,104 and they have been used with some success in the treatment of systemic infections due to MDR strains of these organisms, although at the frequent expense of associated toxicity.51,66,67,96 Increasing resistance to polymyxins has been reported in some regions (e.g., the Mediterranean and Southeast Asia), but resistance to these drugs is generally <10%. However, heteroresistance associated with exposure to suboptimal dosages is an emerging threat, 43 and resistance to colistin among MDR organisms such as P. aeruginosa, A. baumannii, and K. pneumoniae has now been reported.19,81
Antimicrobial treatment of common infections potentially involving MDR gram-negative bacteria
Urinary tract infections
UTIs are among the most common infectious diseases encountered in healthcare settings. They are a major cause of hospital admissions and may be associated with significant morbidity and mortality.61,108 The most common causative organism is E. coli, which is responsible for around 80% of UTIs worldwide, followed by Klebsiella spp. and Proteus spp. 57 UTIs are considered uncomplicated if they occur without structural or neurological abnormalities, or complicated if they occur in the presence of factors predisposing to persistent or relapsing infections, such as foreign bodies (e.g., calculi, indwelling catheters), renal failure, obstruction, and urinary retention due to neurological disease. 79 Because complicated UTIs may be caused by a wide variety of bacteria, including MDR strains, their management is more difficult compared with uncomplicated infections. 80
Over the last decade, the frequency of resistance among gram-negative uropathogens has been steadily increasing, mainly due to widespread use fluoroquinolones and the spread of organisms that produce ESBLs such as CTX-M enzymes, AmpC -lactamases, and carbapenemases.79,108 In the United States, the prevalence of ESBL-producing Enterobacteriaceae among nosocomial uropathogens is around 3% on an average, but rates of up to 25% have been reported. 79 While most ESBL-producing pathogens seen a decade ago were Klebsiella spp., ESBL-producing E. coli are now commonly isolated as well. Indeed, strains of E. coli that produce CTX-M ESBLs, which are often pathogenic and may result in bacteremia, are becoming increasingly prevalent worldwide.57,108
The increased prevalence of resistant gram-negative bacteria has meant that the choice of available agents for treating UTIs is diminishing, particularly if susceptibility testing indicates that the causative organism is resistant to commonly used oral agents such as trimethoprim, fluoroquinolones, and amoxicillin–clavulanic acid.57,108 In an individual patient, the choice of therapy depends on the severity and site of the infection, the presence or absence of complications, local antimicrobial susceptibility patterns, and whether the susceptibility of the causative organism is known or unknown.79,108 However, identifying patients who are likely to have an infection due to MDR organisms is challenging. Also, use of inadequate treatment is likely to increase the level of resistance at both a community level and for the individual patient, which could potentially lead to the development of a more severe infection. 57
In uncomplicated cystitis, fosfomycin and nitrofurantoin can be appropriate as they have good efficacy and low rates of resistance101,134; however, these agents are not appropriate if pyelonephritis is a consideration. In patients with complicated UTIs, the possibility of a resistant organism should be suspected at the outset and treatment selected accordingly. 79 Appropriate antimicrobial choices for empiric therapy of UTIs are shown in Table 5. To avoid adverse patient outcomes, initiation of treatment should not be delayed and should be continued for 7–10 days in patients with complicated lower UTIs, or up to 14 days in patients with upper UTIs. If clinical improvement does not occur within 24–48 hours of starting treatment, the antimicrobial regimen should be reviewed and other treatment instituted based on the results of susceptibility testing.79,108 Relapses of UTIs (i.e., early recurrence of the infection with the same organism) suggest the presence of an upper UTI or a possible complicating condition. 79
When the hospital antibiogram is supportive.
Pneumonias (hospital acquired, ventilator associated, healthcare associated, and community acquired)
Hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and healthcare-associated pneumonia (HCAP) remain important causes of morbidity and mortality in hospitalized patients. 9 The guidelines of the American Thoracic Society and Infectious Diseases Society define HAP as pneumonia occurring at least 48 hours after hospital admission, which was not incubating at the time of admission; VAP as pneumonia that arises 48–72 hours after endotracheal intubation; and HCAP as pneumonia occurring in patients who were hospitalized for at least 2 days within 90 days of the infection occurring, who were residents of a nursing home or long-term care facility, who received intravenous antimicrobial therapy, chemotherapy, wound care within the past 30 days, or who attended a hospital or hemodialysis clinic. 9 It has been recognized that patients with HCAP are heterogeneous and not all risk factors convey the same associated resistance patterns. In a retrospective cohort study of patients with HCAP, which sought to further categorize the risks for pneumonia due to drug-resistant pathogens, 280 of 639 patients (45%) were identified as having a resistant organism. The authors devised a scoring system (4 points for recent hospitalization, 3 for long-term care facility stay, 2 for long-term hemodialysis, and 1 for ICU care) and found that the proportion of patients with antimicrobial-resistant bacteria was highly correlated with the total score: <3 points, <20%; 3–5 points, 55%; and ≥6 points, >75%. 124 When this was applied in a treatment algorithm, low-risk HCAP patients (0–1 risk factors) fared as well as patients with community-acquired pneumonia (CAP) who were treated with CAP therapy, that is, a fluoroquinolone or macrolide plus a β-lactam antimicrobial agent. However, high-risk patients (≥2 risk factors) were treated with HCAP therapy comprising an antipseudomonal β-lactam plus a fluoroquinolone or an aminoglycoside plus vancomycin or linezolid. 97 Although mortality is lower in patients with CAP (3–10%) than in those with HCAP (19.8%), HAP (18.6%), or VAP (29.3%), CAP is still an important cause of morbidity and mortality in hospitalized patients.11,70
In determining a patient's risk and likelihood of resistant pathogens, the time of onset of HAP and VAP is an important factor. Early-onset HAP and VAP (i.e., occurring within the first 4 days of hospitalization) is more likely to be caused by antimicrobial-sensitive bacteria and have a better prognosis, whereas late-onset pneumonia (i.e., occurring after 5 days) is more likely to be caused by MDR pathogens and associated with increased morbidity and mortality. 9 HAP, VAP, and HCAP may be caused by a wide spectrum of bacteria and may be polymicrobial in origin. The most commonly implicated gram-negative pathogens in these pneumonias are P. aeruginosa, Klebsiella spp., E. coli, Acinetobacter spp., and Enterobacter spp.9,63 Although the most frequently implicated gram-negative organisms in patients with CAP are Enterobacteriaceae, Haemophilus influenzae, and Legionella pneumophila, 11 patients who are hospitalized with CAP often have infections due to less common pathogens that are usually hospital associated, such as Pseudomonas and Acinetobacter spp. 93
In recent years, rates of MDR pathogens in hospitalized patients with pneumonia have increased dramatically, the frequency of which varies from hospital to hospital, in different patient populations, and with prior exposure to antimicrobial agents, emphasizing the need for local surveillance data. 9 The most common MDR pathogen causing HAP is P. aeruginosa, but MDR strains of Klebsiella spp., Enterobacter spp., Acinetobacter spp., and E. coli are also increasing in frequency. 9 In the case of VAP, the most common MDR gram-negative bacteria include ESBL- and carbapenemase-producing Enterobacteriaceae, P. aeruginosa, and A. baumannii. 55
Diagnosis of pneumonia is by clinical features (e.g., cough, fever, sputum production, pleuritic chest pain), radiographic findings, and cultures of respiratory secretions. The diagnosis needs to exclude other potential sources of infection, determine the severity of the condition, and reveal other specific conditions that could influence the likely pathogens. 9
Early antimicrobial therapy of pneumonia is imperative because delays in instituting appropriate treatment have a negative impact on the outcome and may be associated with increased mortality.7,9,116,130 For patients with HAP, VAP, and HCAP, the current US guideline emphasizes early institution of adequate dosages of antimicrobial agents to minimize consequent morbidity and mortality, but also avoidance of excessive antimicrobial treatment by de-escalation of the initial therapy based on microbiological cultures and the patient's response and by keeping the duration of therapy to the minimum effective time. 9 Initial empiric therapy (Table 6) should be based on whether the patient has early-onset HAP, VAP, or HCAP (occurring <5 days after hospitalization) or late-onset disease (occurring 5 days after hospitalization), as early-onset pneumonia is less likely to be due to MDR pathogens. 9 While patients in the late-onset group require broad-spectrum therapy, those in the early-onset group, who usually have a better prognosis, may not need broad-spectrum therapy because their infection is more likely to be caused by susceptible bacteria (unless they had received prior antimicrobial therapy or had been hospitalized within the past 90 days). 9 In an individual patient, selection of appropriate antimicrobial therapy needs to take into account the variable bacteriology from one hospital to another, different sites within a hospital, and from one time period to another. Combination therapy should be considered for those likely to be infected with MDR pathogens. 9 Procalcitonin has been a useful adjunct in de-escalating antimicorbial usage and in gauging situations that do not require antimicrobial therapy such as distinguishing bacterial versus nonbacterial causes of pneumonia and sepsis.30,31 In addition, concomitant strategies to modify risk factors should also be implemented (e.g., effective infection control strategies, hand disinfection, monitoring procedures, early removal of invasive devices, etc.).9,40,140
Occurring within first 4 days of hospitalization.
Occurring ≥5 days after hospitalization.
Refer to Table 2 for risk factors for MDR pathogens.
A respiratory fluoroquinolone may be substituted in penicillin-allergic patients.
Aztreonam may be substituted in penicillin-allergic patients.
CAP, community-acquired pneumonia; HAP, hospital-acquired pneumonia; HCAP, healthcare-associated pneumonia; ICU, intensive care unit; VAP, ventilator-associated pneumonia.
For hospitalized patients with CAP who were residents of nursing homes or other long-term care facilities, treatment should be as for patients with HCAP because pneumonias in these patients mirror those of patients with hospital-acquired infections. 93 Selection of treatment for patients hospitalized with CAP should also be based on consideration of the most likely pathogens and local susceptibility patterns. 11 Treatment should be continued for the minimum duration adequate for the patient, but in general should be for a minimum of 5 days and not stopped until the patient has been afebrile for 48–72 hours. 11
In individual patients, treatment should be modified on the basis of the clinical response and culture results. If clinical improvement is observed after 48–72 hours, consideration can be given to de-escalating the antimicrobial therapy or discontinuing it (if possible). However, if there is no improvement after 48–72 hours, the possible presence of other unsuspected pathogens, specific complications, other sites of infection, or a noninfectious diagnosis needs to be considered. 9
Bloodstream and central line-associated infections
BSIs are common in North America and account for nearly 80,000 deaths annually. 147 Among patients with BSIs, those with central-line associated infections (i.e., occurring when a central line has been in place for 2 days in the absence of another identifiable source of BSI) are very common and are a major contributor to healthcare costs. 147 In the United States, 250,000 catheter-related BSIs are estimated to occur each year, and about 80,000 cases occur in ICUs annually. 105 Clinical sepsis, that is, a systemic response to the infection with the presence of some degree of organ dysfunction, is among the most common reasons for ICU admission. Currently, sepsis is believed to be the third most common cause of death in the United States after heart disease and malignant diseases. 95
Although gram-positive bacteria still cause the majority of bacteremias, gram-negative organisms account for a significant and increasing percentage. In the SENTRY Antimicrobial Surveillance Program, the rate of gram-negative BSIs identified during the period 1997–2002 was 35% in North America, while in Latin America it was 44%, and in Europe 43%. 14 The most common gram-negative pathogens isolated in patients with these infections are E. coli, Klebsiella spp., and P. aeruginosa (Table 7).3,123,128,147 As with UTIs and pneumonias, MDR strains are becoming a major threat to the care of patients with these infections. 113 Hospitalized patients who die of severe sepsis attributed to gram-negative bacteria have been found to have significantly greater rates of resistance to their initial antimicrobial regimen than patients who survive, indicating the importance of early initiation of effective antimicrobial therapy and rapid determination of antimicrobial susceptibilities. 103 Diagnosis requires two sets of blood cultures and careful examination to detect a likely source of infection. For suspected catheter-related BSIs, catheter cultures should be performed as soon as the catheter is removed.102,147
Prompt initiation of empiric antimicrobial therapy (Table 8) is imperative (within 1 hour of recognition in cases of severe sepsis) because a delay in initiating therapy has been associated with increased mortality. 95 In patients with septic shock, a critical factor is the duration of hypotension before initiation of effective antimicrobial therapy as each hour of delay in administering antimicrobial therapy after the first hour of documented hypotension has been found to be associated with an average decrease in survival of 7.6% over the ensuing 6 hours. 71 Factors that influence the initial choice of therapy include the severity of the infection, its likely source (e.g., from the urinary tract or intra-abdominal sites), the likely pathogen, local antimicrobial resistance patterns, and the presence of risk factors for resistance.95,147 For patients with catheter-related BSIs, empiric antimicrobial therapy to cover MDR gram-negative pathogens such as P. aeruginosa should be administered to severely ill patients (including neutropenic patients) and those known to be colonized with such organisms. 102
Community-acquired, hospital-acquired, or healthcare-associated.
When culture results are available and the causative organism has been identified, streamlining of the antimicrobial regimen to the most effective narrowest spectrum agent available or de-escalation of the regimen can then be undertaken.102,147 Most patients will require intravenous antimicrobial therapy, which, in the absence of complications, should be given for ≤2 weeks. Those with complications such as infective endocarditis, deep abscesses, or hematogenous seeding of bones and joints require therapy for 4–6 weeks, depending on the pathogen and the adequacy of the response and the source control measures. 147
In patients with catheter-related BSIs, short-term catheters should be removed from those with infections found to be due to gram-negative bacilli. Long-term catheters should be removed from patients with severe sepsis, thrombophlebitis, endocarditis, infections continuing despite more than 72 hours of therapy to which the pathogen is susceptible, or infections due to P. aeruginosa. 102
Intra-abdominal infections
Intra-abdominal infections (IAIs) are often polymicrobial in origin and result from the growth of pathogenic organisms in normally sterile regions of the abdominal cavity. 100 The most common clinical features of IAIs are diffuse or local pain and fever, although their presentation in the elderly and immunosuppressed patients may be atypical. 126 The diagnosis of an IAI should be suspected in a patient exhibiting signs of a systemic inflammatory response and gastrointestinal dysfunction. While uncomplicated IAIs affect a single organ, do not spread to the peritoneum, and do not involve anatomic disruption of the gastrointestinal tract, complicated IAIs extend into the peritoneal space and may lead to an intra-abdominal abscess or diffuse peritonitis. 122 The latter are difficult to manage because drug-resistant gram-negative bacteria are increasingly being isolated in these infections, 12 and they often result in substantial morbidity and mortality in affected patients. 41 Prompt initiation of appropriate antimicrobial therapy is therefore vital in patients with complicated IAIs to prevent subsequent morbidity and mortality. 122
Gram-negative bacteria commonly isolated from patients with IAIs include E. coli, K. pneumoniae, K. oxytoca, E. clocae, P. aeruginosa, and P. mirabilis.12,100 In a SMART study of 6,080 isolates obtained from patients with IAIs in North America from 2005 to 2010, significant increases in rates of ESBL-producing E. coli and K. pneumoniae (the 2 most frequently isolated pathogens) were found in 2010 in comparison with 2005 (7.3% and 13.1%, respectively, in 2010 vs. 1.7% and 3.2% in 2005). 12 Particularly in high-risk patients (i.e., those with higher Acute Physiology and Chronic Health Evaluation [APACHE] II scores, poor nutritional status, cardiovascular disease, and inability to control the source of the infection), 132 who are at greater risk of MDR organisms, blood and intra-abdominal cultures are important to guide antimicrobial therapy in patients with IAIs. 122
The goal of antimicrobial therapy for IAIs is to limit dissemination of the infection if a source control procedure (e.g., drainage of ongoing enteric contamination) is carried out and eliminate any remaining organisms. 100 The antimicrobial regimen needs to be effective against the common gram-negative bacilli and also the obligate anaerobes encountered in these infections. 100 In an individual patient, the choice of empiric antimicrobial therapy (Table 9) should be based on the most likely pathogen and should take into account local and regional resistance patterns among the most commonly isolated pathogens.12,122 As soon as the pathogen has been identified, treatment can be narrowed to the most appropriate agent. In general, antimicrobial therapy should be continued until fever and leukocytosis have resolved. 100 Typically, patients with complicated IAIs are treated for 5–14 days, although once the microbial inoculum has been eliminated by appropriate source control, there may be little need for prolonged therapy in most cases.
In patients who respond poorly to the initial empiric regimen and have persistent signs of infection (e.g., ongoing fever or leukocytosis), changing the antimicrobial regimen or prolonging the duration of therapy can be considered. However, such patients may have a recurrent IAI that requires an additional source control procedure to achieve resolution of the infection. 100
Skin and soft tissue infections
With the increase in prevalence of skin and soft tissue infections (SSTIs) that has occurred in the United States since the mid-1990s, there has been an increase in hospital admissions due to these infections in recent years.10,115 Patients with SSTIs who should be considered for hospital admission are those who present with fever, pain, advancing erythema, or hemodynamic instability, and those who have failed to respond to previous antimicrobial therapy. 10
In establishing a specific diagnosis, microbiologic cultures are important. 135 Although the most common pathogens causing SSTIs are gram-positive organisms (streptococci and Staphylococcus aureus), gram-negative bacteria (including E. coli, Klebsiella spp., Enterobacter spp., P. aeruginosa, and P. mirabilis) may also be responsible, although less commonly.10,99,115 Gram-negative pathogens are more likely to be found in patients with compromised immune systems, diabetic foot infections, and surgical site infections. In diabetic patients who have severe or chronic infections or have received prior antimicrobial therapy, aerobic gram-negative bacilli are often copathogens. 10 Obligate anaerobes should also be considered in patients with ischemic or necrotic wounds. 10
Management of SSTIs includes early antimicrobial therapy and complete surgical debridement for necrotizing infections, with close monitoring of patients. 10 Appropriate broad-spectrum antimicrobial therapy that provides coverage against the likely gram-positive and gram-negative organisms and, if considered likely, anaerobic bacteria is important to improve patient outcomes. 10 Where coverage against gram-negative organisms is considered essential (e.g., for immunocompromised patients), treatment may include an antipseudomonal cephalosporin, a carbapenem, or a combination of either a fluoroquinolone or an aminoglycoside and an extended-spectrum penicillin or cephalosporin. 135
The response to treatment should be assessed after 48–72 hours. Patients whose condition has deteriorated in this time should be treated more aggressively on the basis of culture results and drug susceptibility testing. 10
Acute exacerbations of chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease (COPD) is common in the United States, with nearly 15 million people diagnosed with the condition. 117 Patients experiencing moderately severe or severe acute exacerbations of COPD, most of which have a bacterial, viral, or mixed bacterial–viral etiology, are likely to require hospitalization because they have greater risk factors for a poor outcome and, in severe cases, risk factors for P. aeruginosa infection. 4 The most common bacterial causes of acute exacerbations of COPD are S. pneumoniae and the gram-negative organisms H. influenzae, Haemophilus parainfluenzae, and Moraxella catarrhalis. Less common causes are P. aeruginosa and Enterobacteriaceae.4,53 In elderly patients and those with bronchiectasis, the pathogens isolated from sputum samples are often MDR strains. 4
According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, empiric antimicrobial treatment should be administered to patients with COPD who require mechanical ventilation (invasive or noninvasive) and those who exhibit increased sputum purulence with either increased dyspnea or an increased sputum volume. The choice of initial antimicrobial therapy should be based on an assessment of whether the episode is a “simple” or “complicated” exacerbation, and on local bacterial resistance patterns.4,53 For those with “simple” exacerbations (i.e., without complicating risk factors), amoxicillin, second- or third-generation cephalosporins, doxycycline, extended-spectrum macrolides, or trimethoprim–sulfamethoxazole may be appropriate. 4 However, those with “complicated” exacerbations (i.e., with risk factors for a poor outcome, such as age >65 years, underlying comorbidities [especially cardiac], severe lung disease [FEV1 <50%], frequent exacerbations [four per year], or antimicrobial therapy within the past 3 months), 13,148 should be treated with a respiratory fluoroquinolone such as gemifloxacin, levofloxacin, or moxifloxacin, or with a -lactam/-lactamase inhibitor combination.
The usual duration of antimicrobial therapy for acute exacerbations of COPD is 5–10 days. If an infectious episode does not respond to the initial treatment, a sputum culture and antimicrobial sensitivity tests should be performed to guide further therapy. 53
Importance of infection control measures and antimicrobial stewardship
Infection control measures are important to reduce the transmission of MDR gram-negative organisms in hospitals and acute care facilities. These measures include implementing the CLSI guidelines for early detection of resistant organisms, hand-hygiene educational programs for healthcare personnel, risk factor identification to guide personal protective equipment and procedures, and isolation of patients when resistant infections are detected.28,137 Acute care facilities have established protocols whereby epidemiology and infection control personnel are immediately alerted if resistant organisms are identified. 28 In such instances, infection control measures should be strictly enforced and surveillance cultures repeated periodically until no new cases are identified. 28
In addition, appropriate antimicrobial stewardship programs to ensure effective treatment (including appropriate drug selection, dosing, route of administration, and duration of therapy) are also important to optimize patient outcomes and minimize the unintended consequences of antimicrobial drug use. 36 Because resistance patterns can vary from center to center, good multidisciplinary antimicrobial stewardship is important to continuously evaluate bacterial resistance patterns in individual institutions (e.g., the likelihood of an increased prevalence of CRE as a consequence of the use of carbapenem-based regimens as first-line empiric therapy) and assess the potential for synergism among antimicrobial agents to determine the most effective regimens. 67 In a recent study in patients with gram-negative bacteremia, active stewardship intervention coupled with active alerting of positive blood culture data was found to have a positive impact on the time to implementing appropriate antimicrobial therapy, length of hospital stay, and mortality in comparison with no formalized stewardship intervention. 111
To help ensure the effectiveness of hospital antimicrobial stewardship programs, the checklist of core elements recommended by the CDC is a useful guide. 26
Potential of Newer Antimicrobial Agents in Acute Gram-Negative Infections
A number of newer antimicrobial agents that are potentially beneficial in the treatment of patients hospitalized with acute infections likely to be caused by MDR gram-negative organisms have become available recently or are in the late-phase development. This section reviews the antimicrobial activities of these newer agents and the available clinical and bacteriological data supporting their use in acute gram-negative infections in hospitalized patients.
Newer agents currently approved
Tigecycline and intravenous minocycline
Tigecycline, a novel glycycline antibacterial agent, overcomes several common mechanisms by which bacteria develop resistance and possesses an extended spectrum of activity that includes MDR organisms.37,51,52 It is generally considered a bacteriostatic agent and its mechanism of action is by inhibition of bacterial protein translation by binding to the 30S ribosomal subunit.51,52 Tigecycline is active against most Enterobacteriaceae irrespective of species and against carbapenem-resistant A. baumannii, 37 but P. aeruginosa strains are less susceptible.35,52 Although low rates of nonsusceptibility to tigecycline in vitro were noted among E. coli in a northern European study (<1%), other Enterobacteriaceae showed higher rates (e.g., 7% with Enterobacter cloacae, 9% with K. pneumoniae, and 23% with Serratia spp.). 106
The role of tigecycline in the treatment of seriously ill patients remains uncertain. 52 In addition to low concentrations in the urine (which limit its usefulness in the treatment of UTIs), no activity against P. aeruginosa, and a low threshold for the development of resistance, there are concerns over its safety, which have resulted in a boxed warning being issued by the FDA (see further below). In a noncomparative clinical study involving patients with serious infections (complicated IAIs, pneumonias, skin/skin structure infections, and bacteremias) due to various resistant gram-negative bacteria, including A. baumannii, K. pneumoniae, E. coli, and Enterobacter spp., intravenous tigecycline produced clinical cures in 72.2% of the microbiologically evaluable population and microbiological eradication in 66.7% of patients. 142 In a study in patients with severe complicated IAIs in whom E. coli was isolated in 41.8% of cases, intravenous tigecycline, either as monotherapy or in combination with a variety of other antimicrobial agents, achieved a clinical response rate (i.e., a cure or no further antimicrobial treatment required) of 77.4%. 41
A study that compared intravenous tigecycline and imipenem/cilastatin given for 2 weeks in Chinese patients with complicated IAIs due to either gram-negative aerobic bacteria or gram-positive aerobic and anaerobic bacteria reported clinical cure rates with the two treatments of 81.7% and 90.9%, respectively. 29 In another comparative study of intravenous tigecycline and imipenem/cilastatin in patients with HAP due to both gram-negative bacteria (including K. pneumoniae, A. baumannii, E. coli, E. cloacae, P. aeruginosa, and Serratia marcescens) and gram-positive bacteria, clinical cure rates of 62.7% with tigecycline and 67.6% with imipenem/cilastatin were achieved. 48
An analysis of pooled data from eight phase 3 clinical trials of intravenous tigecycline versus comparators in patients with secondary bacteremias caused by gram-negative and gram-positive bacteria showed that clinical cure rates were nonstatistically higher with tigecycline than with its comparators (81.3% with tigecycline vs. 78.5% for the comparator drugs). 50 However, another published analysis of 15 comparative clinical trials of tigecycline versus other treatments reported a higher relative risk (RR) of mortality of 1.29 (95% confidence interval [95% CI] 1.02–1.64) with tigecycline versus its comparators, and there were also higher risks of clinical failure (RR 1.16; 95% CI 1.06–1.27), microbiological failure (RR 1.13; 95% CI 0.99–1.30), and septic shock (RR 7.01; 95% CI 1.27–38.66) with tigecycline. 150 Although the cause of the mortality difference between tigecycline and its comparators has not been established, the FDA's boxed warning stipulates that tigecycline should be reserved for use in situations when alternative treatments are not suitable. 141
Ceftolozane–tazobactam
This combination -lactam/-lactamase inhibitor antimicrobial agent has recently been approved for the treatment of complicated IAIs (in combination with metronidazole) and complicated UTIs. It comprises the antipseudomonal cephalosporin ceftolozane (CXA-101), which has a high activity against P. aeruginosa and stability against resistance mechanisms exhibited by this organism for other -lactam agents, and the well-established -lactamase inhibitor tazobactam. 120 The antipseudomonal activity of ceftolozane results from its ability to evade multiple resistance mechanisms, including efflux pumps, reduced uptake through porin channels, and modification of penicillin-binding proteins. Tazobactam increases the activity of ceftolozane against ESBL-producing Enterobacteriaceae and some anaerobic species. 152
In an in vitro study, ceftolozane–tazobactam proved more active than ceftazidime, cefipime, and meropenem against P. aeruginosa (including MDR and XDR strains), and it demonstrated a greater activity against Enterobacteriaceae than many currently available cephalosporins and piperacillin–tazobactam.45,120 The development of resistance to ceftolozane–tazobactam among strains of P. aeruginosa has been reported to be slower than resistance to other antipseudomonal agents, and it remained active against mutants resistant to ceftazidime, ciprofloxacin, and meropenem. 18
A phase 2 clinical study of 121 hospitalized patients with complicated IAIs that compared ceftolozane–tazobactam (1.5 g 8-hourly intravenously [IV]) plus metronidazole (0.5 g 8-hourly IV) with meropenem (1 g 8-hourly IV) using a randomized, double-blind design reported a clinical cure in the microbiologically evaluable patient populations of 88.7% with ceftolozane–tazobactam plus metronidazole and 95.8% with meropenem. In patients with E. coli, K. pneumoniae, and P. aeruginosa infections, ceftolozane–tazobactam plus metronidazole achieved microbiological success rates of 89.5% for E. coli infections and 100% for K. pneumoniae and P. aeruginosa infections. 89 A subsequent phase 3 study (the ASPECT-cIAI trial) in a larger number of hospitalized patients with complicated IAIs (n = 806) extended the findings of the earlier phase 2 study and concluded that ceftolozane–tazobactam plus metronidazole was noninferior to meropenem in treating these infections. 131 The phase 3 study also had a randomized, double-blind design and used similar dosages to those administered in the phase 2 trial. In the microbiological intention-to-treat (MITT) population, clinical cure rates at the test-of-cure visit were 83.0% (323/389) with ceftolozane–tazobactam plus metronidazole and 87.3% (364/417) with meropenem. 131 However, in patients diagnosed with ESBL-producing Enterobacteriaceae, clinical cure rates were higher with ceftolozane–tazobactam plus metronidazole than with meropenem (95.8% [23/24] vs. 88.5% [23/26], respectively), and they were also higher than with meropenem against highly resistant strains positive for CTX-M-14/15-type enzymes (100% [13/13] vs. 72.7% [8/11], respectively). 131
In patients with complicated lower UTIs or pyelonephritis, a multinational, randomized, double-blind trial (ASPECT-cUTI) in which ceftolozane–tazobactam (1.5 g 8-hourly IV) was compared with high-dose levofloxacin (750 mg once daily IV), both given for 7 days, ceftolozane–tazobactam provided better clinical cure and microbiological eradication responses than levofloxacin. 145 Composite cure (i.e., clinical cure and microbiological eradication) rates in the microbiological modified ITT (mMITT) study populations were 76.9% (306/398) with ceftolozane–tazobactam and 68.4% (275/402) with levofloxacin. Subgroup analyses indicated that composite cure rates were significantly higher with ceftolozane–tazobactam than with levofloxacin in patients with ESBL-producing uropathogens (62.3% [38/61] vs. 35.1% [20/57], respectively), complicated lower UTIs (67.1% [47/70] vs. 47.3% [35/74], respectively), and patients 65 years of age (70.0% [70/100] vs. 53.5% [53/99], respectively). 145
Ceftazidime–avibactam
This combination -lactam/-lactamase inhibitor agent has also recently been approved for the treatment of complicated IAIs (in combination with metronidazole) and complicated UTIs. Avibactam (NXL104, AVE1330A) is a non—lactam -lactamase inhibitor with a novel reversible mechanism of action 39 that inhibits serine -lactamases by forming a covalently bound enzyme complex. 74 Although it has little intrinsic antibacterial activity, avibactam in combination with the broad-spectrum cephalosporin ceftazidime is able to restore the activity of the latter against Enterobacteriaceae that produce extended-spectrum or AmpC -lactamases and against most Enterobacteriaceae that produce KPC and OXA-48 carbapenemases.2,85 In 2012, ceftazidime–avibactam was found to be active against most -lactamase-producing Enterobacteriaceae isolated in US hospitals. 22 Avibactam also improves the activity of ceftazidime against MDR P. aeruginosa, 2 but not against Acinetobacter spp. 73 Significant bacterial killing/efficacy has been demonstrated with ceftazidime–avibactam in a number of experimental infection models, including sepsis, thigh infection, pneumonia, and kidney infection models, and in a rabbit model of meningitis due to Enterobacteriaceae that were nonsusceptible to ceftazidime. 73
Thus far, only a limited number of clinical studies of ceftazidime–avibactam have been published. In a phase 2, randomized, double-blind clinical trial that compared ceftazidime–avibactam (2.5 g 8-hourly) plus metronidazole (0.5 g 8-hourly) with meropenem (1 g 8-hourly) in patients with complicated IAIs predominantly due to E. coli, a favorable clinical response at the test-of-cure visit in the microbiologically evaluable population was achieved in 91.2% (62/68) of patients with ceftazidime–avibactam plus metronidazole and 93.4% (71/76) with meropenem. Among 43 patients with ceftazidime-nonsusceptible pathogens, favorable microbiological response rates in the two groups were 96.2% (25/26) and 94.1% (16/17), respectively. 90
A phase 2, randomized, double-blind trial that compared ceftazidime–avibactam (0.625 g 8-hourly IV) with imipenem–cilastatin (0.5 g 6-hourly) in hospitalized patients with complicated UTIs predominantly caused by E. coli reported favorable microbiological responses at the test-of-cure visit in 70.4% (19/27) of the microbiologically evaluable population with ceftazidime–avibactam and 71.4% (25/35) with imipenem–cilastatin. Among 18 patients with ceftazidime-resistant pathogens, favorable microbiological response rates in the two groups were 85.7% (6/7) and 81.8% (9/11), respectively. 143
Newer agents in late-phase development
Meropenem-RPX7009
The carbapenem agent meropenem in combination with the serine -lactamase inhibitor RPX7009 is under development for the treatment of serious bacterial infections due to gram-negative pathogens that produce serine enzymes, in particular KPC-producing strains of Enterobacteriaceae. Although RPX7009 alone has no antibacterial activity,39,54 it potentiates the effect of meropenem. In an in vitro study comparing the activity of the meropenem-RPX7009 combination and meropenem alone against KPC-producing K. pneumoniae isolates, the combination inhibited 83.0% and 92.0% of isolates, respectively, at minimum inhibitory concentrations (MICs) of 1 and 4 g/ml, whereas meropenem alone inhibited only 3.0% and 24.0% of isolates, respectively, at the same concentrations. 23 An in vivo infection model (mouse thigh infections) showed that meropenem-RPX7009 produced significant bacterial killing against all strains of CRE tested. 119
The first clinical studies of meropenem-RPX7009 are investigating its efficacy, safety, and tolerability in patients with complicated UTIs and acute pyelonephritis (AP). 33
Imipenem–cilastatin plus relebactam (MK-7655)
Relebactam (MK-7655), a piperidine analog -lactamase inhibitor that inhibits both class A and class C -lactamases in vitro, has been shown to restore the activity of imipenem against imipenem-resistant Pseudomonas and Klebsiella spp. at clinically achievable concentrations. 15 Based on its in vitro and in vivo activities and favorable pharmacokinetic and toxicity profiles, relebactam was selected for clinical development in combination with imipenem and the renal dehydropeptidase inhibitor cilastatin. In an in vitro study, dose-dependent potentiation of the activity of imipenem by relebactam was noted against KPC-producing Enterobacteriaceae. In addition, relebactam augmented the activity of imipenem against P. aeruginosa strains in general and against imipenem-resistant P. aeruginosa strains due to loss of outer membrane porin D (OprD) protein. 87 Synergy with imipenem against four imipenem-resistant bacterial strains—a KPC-producing K. pneumoniae isolate and three P. aeruginosa isolates with OprD deletions—has also been observed. 60
The first clinical studies of imipenem–cilastatin plus relebactam are investigating the safety, tolerability, and efficacy of this combination versus imipenem–cilastatin alone for the treatment of complicated UTIs and IAIs. 33
Eravacycline (TP-434)
Eravacycline is a novel fluorocycline compound that exerts a broad spectrum of activity against MDR gram-negative and gram-positive organisms, including tetracycline-resistant Enterobacteriaceae that produce ESBLs or carbapenemases. 56 Its activity appears to be largely unaffected by common tetracycline-specific resistance mechanisms.56,136 In a study of its antibacterial activity against hospital and community pathogens, eravacycline proved to be active against MDR bacteria, including strains expressing ESBLs and mechanisms conferring resistance to other antimicrobials, including carbapenems. 136 A comparison with tigecycline showed that MIC90 values for eravacycline were at least twofold lower than those of tigecycline against the majority of gram-negative organisms tested, including A. baumannii, K. oxytoca, P. mirabilis, and Proteus vulgaris. 136 In another study, eravacycline was active against MDR gram-negative pathogens isolated from patients treated at New York City hospitals in 2013–2014, including strains expressing KPC and OXA-type carbapenemases and A. baumannii isolates. 1
A pharmacokinetic study of intravenous eravacycline in healthy adults found that concentrations of the drug in epithelial lining fluid and alveolar macrophages were 6-fold and 50-fold greater, respectively, than those achieved in plasma, suggesting that it may be of value in respiratory infections. 34 In the only clinical study reported to date, eravacycline administered intravenously at dosages of 1.0 and 1.5 mg/kg/day for a minimum of 4 days was as effective in terms of clinical and microbiological end points as ertapenem 1 g daily in hospitalized patients with complicated IAIs. 133
Plazomicin
Plazomicin (ACHN-490) is a next-generation aminoglycoside derived from sisomicin that is currently at phase 3 of development. 153 It is active against both gram-positive and gram-negative bacteria, including strains harboring aminoglycoside-modifying enzymes (the most common mechanism of resistance to this class of drugs), and may offer a treatment option for infections caused by strains resistant to other aminoglycosides.6,153 Plazomicin has been found to have a potent in vitro activity against aminoglycoside-nonsusceptible E. coli and an equivalent activity against ESBL-producing and non-ESBL-producing E. coli and K. pneumoniae. 146 It has also demonstrated an activity against most strains of CRE (except those harboring 16S rRNA methylases), 86 and against A. baumannii and P. aeruginosa.76,109
Clinical trials of plazomicin are currently investigating its efficacy and safety in patients with BSIs due to CRE (compared with colistin) and in patients with complicated UTIs and AP (compared with intravenous levofloxacin). 33
Antiendotoxin therapy (polymyxin B direct hemoperfusion)
Because endotoxin is a potent mediator of sepsis, and high levels are found in ∼50% of patients with septic shock, it is an attractive target against which to develop therapies to aid in the management of sepsis.62,68 A novel targeted strategy for endotoxin removal that has been evaluated in some countries is polymyxin B direct hemoperfusion (PMX-DPH) in which polymyxin B, which has the ability to bind and neutralize endotoxin, is adsorbed on polystyrene-derived fiber in a hemoperfusion device that can then be used to filter blood externally through an extracorporeal circuit.68,118 Clinical studies of this approach in patients with septic shock have shown that PMX-DPH therapy results in improvements in hemodynamics, oxygenation, and renal dysfunction and reduces mortality. 118
Currently, a multicenter, randomized, controlled clinical trial (the EUPHRATES trial) is evaluating the efficacy of PMX-DPH therapy in patients with septic shock and confirmed endotoxemia (as measured by the endotoxin activity assay) in 50 ICUs in the United States and Canada. 68
Conclusions
The rising prevalence of MDR strains of gram-negative bacteria, particularly among Enterobacteriaceae (especially K. pneumoniae and E. coli), P. aeruginosa, and A. baumannii, in the last decade constitutes a serious threat to global public health. Infections caused by these organisms are becoming increasingly more problematic in hospitalized patients, particularly as there has been a paucity of new compounds targeting these pathogens in recent years. In addition to higher death rates, MDR gram-negative infections are associated with an ever-growing socioeconomic burden due to the increased resource utilization required for their management.
In the hospital setting, good multidisciplinary antimicrobial stewardship, whereby bacterial resistance patterns and the potential for synergism among antimicrobial agents are continuously being evaluated, is necessary to determine the most appropriate treatment regimens for MDR gram-negative infections. When a high risk of MDR gram-negative organisms exists in a seriously ill hospitalized patient, a prudent strategy for initial empiric antimicrobial therapy is to select a broad-spectrum regimen comprising drugs that have different mechanisms of action and different mechanisms by which resistance can occur, to broaden the antimicrobial coverage and utilize the potential for synergism. Subsequently, the initial empiric regimen can be tailored when susceptibility reports are available.
Although their places in therapy have yet to be conclusively established, several newer antimicrobial agents that have added to the limited armamentarium available for treating resistant gram-negative infections in the hospital setting have become available recently or are at a late phase of development. Recently introduced agents include the glycycline agent tigecycline, the antipseudomonal cephalosporin ceftolozane in combination with the well-established -lactamase inhibitor tazobactam, and the broad-spectrum cephalosporin ceftazidime in combination with the novel -lactamase inhibitor avibactam. These agents all exhibit an activity against MDR gram-negative bacterial strains and have considerable potential in the treatment of patients hospitalized with acute infections potentially caused by these organisms.
Footnotes
Acknowledgments
The research and preparation of this article was funded by Forest Laboratories, LLC. The authors had full control over content, material, writing, and editing and take full responsibility for the article. The authors received no payment for this article. Writing and editorial support for preparation of the article was provided by The Medicine Group.
Disclosure Statement
Dr. E. Cerceo is on the advisory board for Cempra, Inc. and is a consultant for Forest Laboratories. Dr. Dietzelweig is on the advisory board/speaker bureau/conducted research for Jannsen and Bristol-Myers Squibb. He is on the advisory board for Daiichi Sankyo, has conducted research for Otsuka, and is a consultant for Forest Laboratories. Dr. B. Sherman is a consultant for Forest Laboratories, and is on the Advisory Boards of Merck, Cempra, Sanofi-Aventis, and Theravance. Dr. A.N. Amin is a consultant or speaker for Forest, Cempra, and Cubist.