
Abstract
Methicillin-resistant Staphylococcus aureus (MRSA) carrying SCCmec type IV has emerged in hospitals worldwide. The aim of this study was to evaluate phenotypic and molecular characteristics of antimicrobial resistance in MRSA SCCmec IV isolates, presenting different genetic backgrounds, isolated from hospitals in Rio de Janeiro. The antimicrobial resistance of 128 S. aureus type IV isolates from 11 hospitals was characterized by the disk diffusion test and minimum inhibitory concentration (MIC) test. Mutations in parC gene, which encodes ciprofloxacin resistance, and genes associated with macrolide–lincosamide–streptogramin B (MLSb) resistance were also investigated. MRSA isolates belonging to USA400/ST1 (60 isolates), USA800/ST5 (40), USA1100/ST30 (13), and other 11 (15) lineages were mainly resistant to erythromycin (68%), ciprofloxacin (56%), and clindamycin (50%). The highest antimicrobial resistance rates were found among USA400 isolates (p < 0.05). The majority of them (90%) carried only the erm(C) gene and mainly presented two mutation types in the parC gene. The msr(A) gene was most frequently found among USA800 isolates (p < 0.05). Among MRSA type IV isolates from Rio de Janeiro hospitals, multiresistance, including mutations in parC gene, was associated to the USA400/ST1, while the msr(A) gene was associated with USA800/ST5 isolates, highlighting that these lineages could have more potential to persist in a hospital environment.
Introduction
S
Most MRSA SCCmec IV isolates isolated from Brazil4,5 and worldwide 6 are resistant to macrolide–lincosamide–streptogramin B (MLSb) and quinolones. The MLSb resistance in staphylococci involves two mechanisms: alterations on 23S rRNA encoded by the erm genes and an adenosine triphosphate (ATP)-dependent efflux pump conferred by the msr(A) gene. 7 Quinolones resistance in Staphylococcus is also due to an efflux pump, encoded by genes, such as norA and norB, 8 and/or mutations in gyrA, gyrB, parC, and/or parE genes in a region called “quinolone resistance-determining region” (QRDR). 9 Our group verified in a previous study that the erm(A) and erm(C) genes, associated with MLSb resistance, were associated with the SCCmec types III and IV, respectively, in MRSA isolates, indicating that these genes could be good markers of these SCCmec types. 5
In Brazil, infections by MRSA SCCmec IV isolates have emerged in hospitals, and an increased mortality rate has been described. 10 Moreover, these isolates present oxacillin MICs close to the breakpoints, which can make their detection difficult. 11 Among the different SCCmec IV lineages spread in Brazil, sequence type (ST) 1 isolates from the USA400 clone have revealed multidrug resistance mainly to MLSb and quinolones.4,12 However, the molecular investigation of these antimicrobial resistance types is not very well described among MRSA isolates, especially, comparing isolates from different genetic backgrounds. In the present study, we investigated the molecular and phenotypic antimicrobial resistance, highlighting MLSb and quinolone resistance, among SCCmec IV MRSA isolates from different clonal lineages recovered from Rio de Janeiro hospitals.
Methods
Clinical isolates and control strains
One hundred twenty-eight MRSA type IV isolates obtained from different clinical specimens (nostrils n = 54, blood n = 20, wound n = 19, prosthesis secretion n = 10, and other sites n = 25) from patients in 11 hospitals in the city of Rio de Janeiro, between July 2004 and June 2009, were evaluated (Table 1). The SCCmec types detection, 13 the genotypes, 14 and the sequence types 15 were determined as previously described. The clonal complexes (CC) were determined according to eBurst. Ciprofloxacin- and MLSb-resistant MRSA isolates from the lineages of Brazilian epidemic clone-BEC/ST239/SCCmec type III and USA100/ST5/type II, previously identified, were used as control strains to compare with the results of the analysis of MRSA type IV isolates.
HBD, Hospital Barra D'or; HCD, Hospital Copa D'or; HL, Hospital da Lagoa; HLJ, Hospital Lourenço Jorge; HNMD, Hospital Naval Marcilio Dias; HPL, Hospital Perinatal de Laranjeiras; HUCFF, Hospital Clementino Fraga Filho; IFM, Instituto Fernandes Magalhães; INTO, Instituto Nacional de Traumatologia e Ortopedia; IPEC, Instituto de Pesquisa Evandro Chagas; MRSA, methicillin-resistant Staphylococcus aureus; ND, not determined; PB, Hospital Pronto Baby; SCC, staphylococcal cassette chromosome.
Antimicrobial susceptibility tests
The susceptibility to ciprofloxacin, clindamycin, chloramphenicol, erythromycin, gentamicin, linezolid, mupirocin, oxacillin, rifampicin, teicoplanin, tigecycline, trimethoprim/sulfamethoxazole (SUT), and tetracycline (Oxoid, Basingstoke, UK) was determined by the disk diffusion test. 16 The minimum inhibitory concentration (MIC) for ciprofloxacin, clindamycin, chloramphenicol, erythromycin, gentamicin, linezolid, oxacillin, rifampicin, SUT, tetracycline, and vancomycin (Sigma-Aldrich Company, St. Louis, MO) was determined by the broth microdilution method. 17 MICs for mupirocin, teicoplanin, and tigecycline were determined by the E-test® (BioMérieux, Marcyl'Etoile, France).
Detection of the erm (A, B, and C) and the msr(A) genes and mutation analysis in the parC gene (QRDR region) by sequencing
The erm (A, B, and C) and msr(A) genes were detected as previously described.7,18 Mutations in parC gene in ciprofloxacin-susceptible and ciprofloxacin-resistant MRSA isolates were detected by DNA sequencing. PCR amplicons of the gene were obtained according to Schmitz et al. 19 and purified using the commercial system “GTX PCR and band purification” (GE 50 Healthcare, Buckinghamshire, England) according to the manufacturer's specifications. The purified products were sequenced using the automated DNA sequencer ABI3100 (Applied Biosystems, Foster, CA). The sequences obtained were analyzed using the program BioEdit (Carlsbad, CA) and Ugene (Novosibirsk, Russia).
Statistical analysis
The Fisher's exact test and chi-square test were used to compare the data. Significance was established at 5% (p < 0.05).
Results
Clinical isolates and antimicrobial susceptibility
Out of 128 isolates with SCCmec IV evaluated in the present study, 88% were assigned to USA400/ST1/CC1, USA800/ST5/CC5, and USA1100/ST30/CC30 lineages (Table 1). Except for oxacillin, all MIC results were compatible with the disk diffusion test results. All the MRSA isolates were susceptible to linezolid, SUT, teicoplanin, tigecycline, and vancomycin. Resistance was mainly found for erythromycin (68%), ciprofloxacin (56%), and clindamycin (50%; Table 2). USA400 isolates presented higher resistance rates to ciprofloxacin, clindamycin, chloramphenicol, and gentamicin than other lineages (p < 0.05) (Fig. 1). USA1100 isolates were susceptible to all antimicrobials analyzed. Twelve (9%) MRSA isolates showed MIC values of susceptibility to oxacillin (<4 μg/ml), and six (50%) of them were related to the USA1100 lineage. Eight (6%) isolates exhibited MIC = 2 μg/ml for vancomycin.
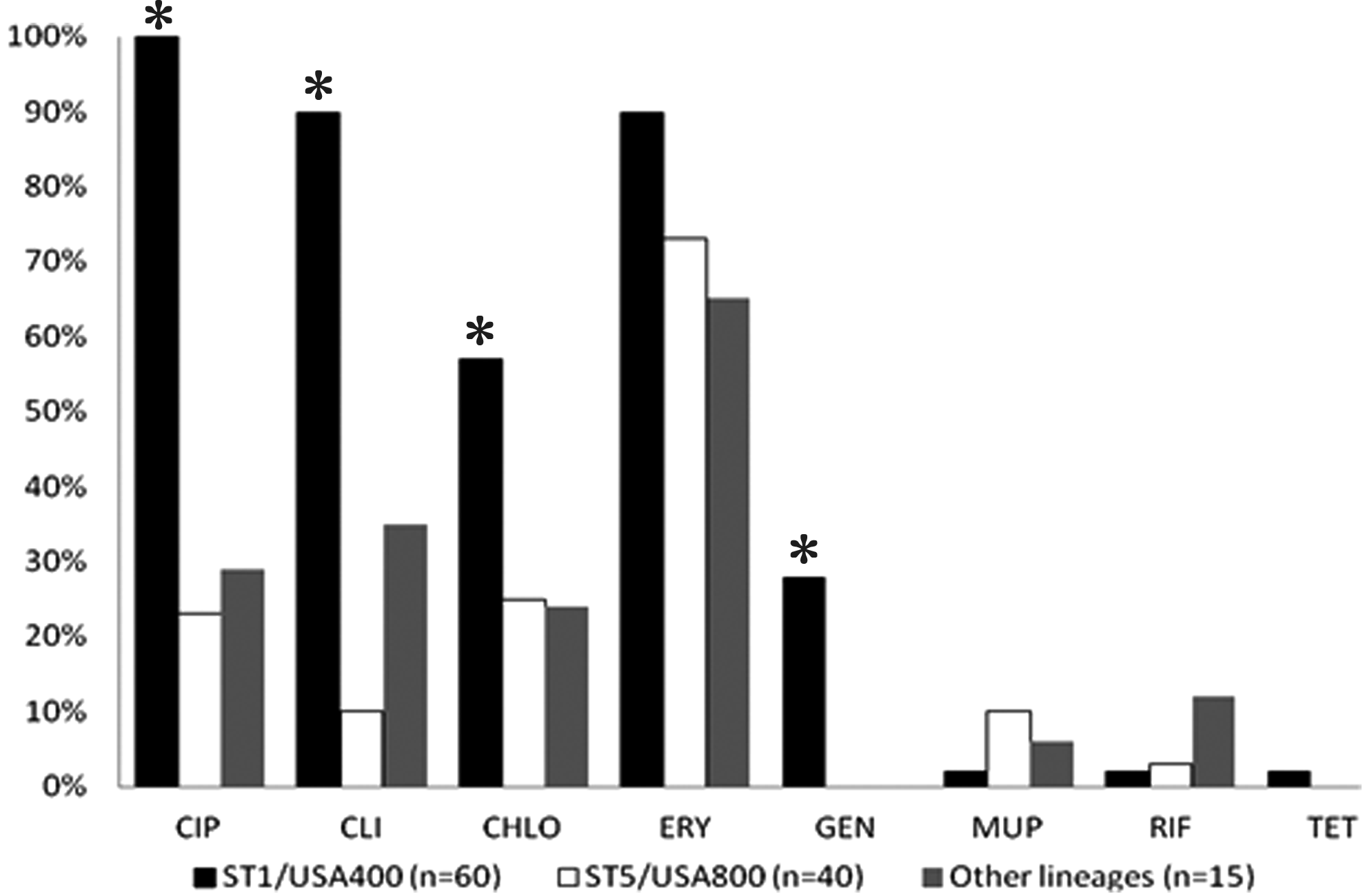
Antimicrobial resistance patterns of 115 MRSA type IV isolates according to clonal lineage. *Significant differences (p < 0.05) for resistance rates among USA400/ST1 isolates in relation to USA800/ST5 or other lineages were verified to ciprofloxacin, clindamycin, chloramphenicol, and gentamicin. Thirteen USA1100/ST30 isolates were susceptible to all antimicrobials tested and were not included in the figure. Chlo, chloramphenicol; Cip, ciprofloxacin; Cli, clindamycin; Ery, erythromycin; Gen, gentamicin; MRSA, methicillin-resistant Staphylococcus aureus; Mup, mupirocin; Rif, rifampin; and Tet, tetracycline.
All results of the microdilution test were compatible with the disk diffusion test, except for oxacillin. Oxacillin MIC was not compatible with the disk diffusion test for cefoxitin to detect MRSA isolates.
I, intermediate; MIC, minimum inhibitory concentration; NA, not applicable; R, resistant; S, sensitive; TMP/STX, trimethoprim/sulfamethoxazole.
Association between MIC values, resistance genes, and S. aureus lineages
Regarding MLSb resistance, the highest MIC values for erythromycin and clindamycin were found among USA400 and ST97 isolates. The erm(C) gene was often found alone in these isolates (p < 0.05; Table 3). All USA400 and USA800 isolates carried at least one MLSb resistance gene. Except for two USA400 isolates, all other isolates that carried the msr(A) gene were USA800 isolates (p < 0.05). Although all USA1100 isolates presented MIC of 0.5 μg/ml to clindamycin and erythromycin, the majority (92%) of them carried at least one MLSB resistance gene.
ST5 and ST30 isolates unrelated to the USA800 and USA1100 clones, respectively.
Cli, clindamycin; Ery, erythromycin; ND, not determined; MLSb, macrolides–lincosamides–streptogramin; ST, sequence type.
Mutations in the parC gene and association with ciprofloxacin MIC values in 18 representative isolates of MRSA SCCmec IV are shown in Table 4. Ciprofloxacin-resistant isolates had at least one kind of the following mutations in the QRDR region (“quinolone resistance-determining region”): serine (Ser)-80 → phenylalanine (Phe)/tyrosine (Tyr) and glutamic acid (Glu)-84 → lysine (Lys). For the five USA400/ST1 isolates with ciprofloxacin MICs >256 μg/ml, the presence of double mutations at Ser-80 → Tyr and Glu-84 → Lys was detected, while the other USA400 isolate presenting CMI of 32 μg/ml had only one mutation, Glu-84 → Lys. Another type of mutation was observed on four ciprofloxacin-resistant USA800/ST5 isolates, Ser-80 → Phe, and all presented low MIC values for ciprofloxacin. Isolates from ST97 with ciprofloxacin MIC values >256 μg/ml showed the same two mutations found among USA400 isolates. All isolates presenting ciprofloxacin MICs ≤1 μg/ml did not show mutations in the parC gene.
Gly, glycine; Lys, lysine; ND, not determined; NA, not applicable; Phe, phenylalanine; Ser, serine; Tyr, tyrosine.
The sequencing of the parC gene of control strains showed that BEC/type III isolates presented the Ser-80 → Phe mutation, regardless of the MIC value. Regarding USA100/ST5/type II lineage, an isolate with ciprofloxacin MIC of 8 μg/ml had the Ser-80 → Phe mutation, whereas isolates with MICs of 128 μg/ml showed both Ser-80 → Tyr and Glu-84 → Lys mutations.
Discussion
MRSA is one of the major causes of healthcare- and community-related infections. In the last decade, infections by MRSA SCCmec IV isolates have emerged in hospitals in many countries. Surprisingly, despite their community origin, many of these isolates from Brazil4,20 and worldwide21,22 already present multidrug resistance. Furthermore, little is known about the molecular resistance to drugs and its relationship with different MRSA lineages. In our study, 128 MRSA type IV isolates of 14 different lineages isolated from Rio de Janeiro hospitals were analyzed for antimicrobial resistance, highlighting the MLSb and quinolone resistances. We confirmed the resistance to these drugs and verified that some resistance genes and specific mutations in the parC gene could be considered resistance markers for certain Brazilian MRSA type IV lineages.
Although the MLSb antibiotics and quinolones can be used as an alternative for treatment of staphylococcal infections, the resistance to these drugs has already been observed in about 50% of the staphylococci isolates.23,24 In the present study, we verified that 50% or more of isolates were resistant to ciprofloxacin, erythromycin, and clindamycin, confirming the results of studies conducted by other authors in Brazil 20 and worldwide21,22 with MRSA type IV isolates. However, in general, the studies do not show the relationship between resistance to drugs and clonality of the isolates. Our study showed that USA400/ST1 isolates were significantly more resistant to clindamycin and ciprofloxacin, and also showed high resistance to erythromycin. Silva-Carvalho et al. 20 analyzed 150 MRSA isolates from patients of two hospitals at Rio de Janeiro and also showed that 56% of isolates from this lineage were resistant to three or more non-β-lactam antimicrobials. Antimicrobial resistance among USA400 isolates seems to be more evident among Brazilian isolates. In Canada, the USA400 lineage remains predominant in some provinces and has showed susceptibility to quinolones and MLSb drugs. 25 In Italy, high resistance rates among SCCmec IV isolates were also found. However, the authors evaluated isolates from the USA300 lineage, which is more frequently isolated in hospitals from that country. 22 Also, in the present study, USA800/ST5 and USA1100/ST30 isolates were susceptible to the majority of antimicrobial agents tested, a fact that agrees with the data shown among isolates from Switzerland. 26
The decreased susceptibility to MLSb and quinolones found in our study was further investigated by the detection of genes related to resistance to these drugs. We verified that USA400/ST1 isolates carried mainly the gene erm(C) alone, and this association was significant. Although the association between MRSA type IV isolates and the erm(C) gene had already been observed by other authors, 5 MRSA lineages were not evaluated by them. It is possible that the greater resistance among USA400/ST1 isolates is related to the presence of this erm gene alone in the isolates of this lineage, since the three USA400/ST1 isolates presenting both erm(A) and erm(C) genes showed erythromycin and clindamycin MIC values <0.5 μg/ml. This relationship can refer to isolates from our region or even to the study period. Further studies are necessary to support these findings.
In the present study, the msr(A) gene that encodes an efflux pump related to MLSb resistance was found in 20% of the MRSA isolates and, except for two isolates, only USA800/ST5 isolates carried this gene. According to Teodoro et al., 5 unlike the erm genes, the msr(A) gene is associated with a low level of resistance to erythromycin, as was seen in this study for the USA800 isolates. Gul et al. 27 found the msr(A) gene in 17% of 225 MRSA isolates, whereas Teodoro et al. 5 detected this gene in 12% of the MRSA type IV isolates. However, these authors did not describe the MRSA lineages on their studies. Nevertheless, González-Domínguez et al. 28 when analyzing community-onset MRSA isolates from Spain found that the spa type 067 was linked to the presence of msr(A) gene. Therefore, further studies are needed with a larger sample size to confirm our results.
Mutations in “hot spot” regions of parC gene, called QRDR can confer high-level resistance to fluoroquinolones. 9 In the present study, we observed that no ciprofloxacin-susceptible isolates showed mutations in the QRDR region, while all isolates resistant to this antibiotic had at least one mutation type. Interestingly, among the USA400/ST1 isolates with ciprofloxacin MIC values higher than 256 μg/ml, two types of mutations (Ser 80 → Tyr and Glu 84 → Lys) were detected. On the contrary, the other isolate of the same lineage presenting a low MIC of 32 μg/ml had only the mutation Glu 84 → Lys. Similarly, all USA800/ST5 isolates presented only one type of mutation (Ser 80 → Phe). Although these isolates had presented a different mutation, the ciprofloxacin MIC values also were low, between 4 and 16 μg/ml. Sanfilippo et al. 9 reported that all the S. aureus with two types of parC mutations had ciprofloxacin MICs higher than those with only one mutation type, similar to our results. However, the authors did not characterize the clonality of the isolates. It is possible that there is an association between the MIC values and the number of mutations in the parC gene, as well as the clonality of S. aureus isolates that can also be involved in this relationship. Further studies are needed to show this association.
In the present study, 12 (9%) MRSA isolates showed MICs for oxacillin lower than 4 μg/ml, and half of them belonged to the USA1100/ST30 lineage. The occurrence of low MIC values to oxacillin in MRSA isolates can be found in Brazilian strains, especially, among community-acquired USA1100/ST30 isolates. 29 However, it is more difficult to find among hospital isolates. This fact can be a problem for clinical routine laboratories as they may mistakenly identify methicillin-resistant isolates as sensitive. 11
This study showed that among MRSA type IV isolates from Rio de Janeiro hospitals, multiresistance, including double mutations in the parC gene of quinolone resistance, was associated to the USA400/ST1 lineage, while the msr(A) gene was related to USA800/ST5 isolates. These data can explain why certain clonal lineages seem to present more potential to persist in the hospital environment.
Footnotes
Acknowledgments
This study was supported by grants from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ); Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq); Coordenação de Aperfeiçoamento Pessoal de Nível Superior (CAPES); Fundação Universitária José Bonifácio (FUJB); and Programa de Núcleos de Excelência (PRONEX).
Disclosure Statement
No competing financial interests exist.