
Abstract
The small-colony variant (SCV) phenotype of Staphylococcus aureus is associated with intracellular persistence and reduced antimicrobial susceptibility, which can lead to therapeutic failure. Since SCVs grow slowly and have a confusing morphology, the identification of infections due to SCV is difficult. We have identified SCVs in two patients who presented with persistent methicillin-resistant Staphylococcus aureus (MRSA) bacteremia complicated by surgical site infections after cardiothoracic surgery. Nine blood isolates were collected from the two patients for species identification, antimicrobial susceptibility testing, and phenotypic and genotypic characterization. Colonies on Columbia blood agar were pinpoint, nonpigmented, nonhemolytic, and reverted to normal colonies after 48 hr of incubation on Schaedler agar. Auxotrophy assays revealed hemin dependence. Susceptibility to vancomycin (minimal inhibitory concentrations 1.0 μg/mL) was confirmed by E-test and broth microdilution test. All the isolates were identified as MRSA by multiplex polymerase chain reaction specific for the mecA, femA, and 16S rRNA genes, and all had the same genotype: Multilocus sequence typing ST5, SCCmec type II, agr type II, and spa type t2460. Moreover pulsed-field gel electrophoresis typing revealed that all nine isolates belonged to the same clone. Mutations in the relA gene were not found, and none of the isolates was identified as hVISA by population analysis profiling-AUC ratio. A high level of suspicion is required to detect SCVs, and although it is not common, the possibility of the SCV phenotype has to be considered in persistent S. aureus bacteremia.
Introduction
S
S. aureus subpopulations with the small-colony variant (SCV) phenotype are especially associated with relapsing or persistent infections,2,5–12 and have been described in many clinical situations, such as chronic osteomyelitis, deep-seated and cutaneous abscesses, endocarditis, brain abscesses, prosthesis-related infections, endobronchial infections, and bacteremia.5,12,13 SCVs are characterized by reduced growth rate, small colony size (about one-tenth of normal phenotype colonies), absence of pigmentation, weak hemolytic activity, and on many occasions, auxotrophy for hemin, menadione, or thymidine.5,14 There is increasing evidence that important features of SCVs contributing to their persistence and to therapeutic failure, such as increased antimicrobial resistance, 15 enhanced ability to form biofilms,10,16 and reduced expression of cytolytic toxins,17,18 result from increased internalization within host cells and persistence within them.11,18
Diagnostic failure is another obstacle to the successful treatment of infections due to SCVs. Because of their small colony size and slow growth rate, SCVs are often overlooked on culture plates, or plates are discarded before a diagnosis can be made.2,11,19,20 SCVs of S. aureus are also often misinterpreted as coagulase-negative staphylococci, due to their absence of pigmentation, weak hemolytic activity, and decreased coagulase production. 11
In this report, we describe the isolation and characterization of SCV methicillin-resistant Staphylococcus aureus (MRSA) from two patients who underwent cardiothoracic surgery and suffered from bacteremia due to surgical site MRSA infection during their admission at the Department of Thoracic Surgery. The bacteremia lasted over a month in both patients, despite appropriate antibiotic and surgical therapy.
Case Report
Case 1
A 77-year-old male patient with a history of hypertension and diabetes was admitted for acute chest pain. Since his initial chest X-ray showed mediastinal widening, a dissecting thoracic aortic aneurysm was suspected. During computed tomography (CT) scanning, the patient suffered a cardiac arrest and underwent emergent surgery for a ruptured thoracic aortic aneurysm. A vascular stent was inserted in the ascending aorta, aortic arch, and descending aorta. He was not screened for MRSA carriage preoperatively.
On the 10th postoperative day (POD), fever was detected, accompanied by local erythema, tenderness, and discharge from the surgical wound. The patient was started on intravenous vancomycin under the impression of surgical site infection associated with vascular graft infection. MRSA was isolated from blood and wound cultures. On POD 12, a follow-up CT scan was performed to re-evaluate the extent of the infection. It revealed focal fluid collection with suspicious peripheral rim enhancement at the aortic arch, which was surgically drained the next day. Results from postdebridement tissue culture also revealed MRSA.
After the debridement operation, the surgical site healed without further apparent complications, but the MRSA bacteremia persisted for 35 days. Defervescence was achieved on the 25th day of antibiotic treatment. Due to the persistent MRSA bacteremia, the antibiotic was changed to linezolid after 28 days of treatment. However, as the patient subsequently developed severe thrombocytopenia, he was changed to vancomycin and rifampin. He received vancomycin and linezolid alternatively for 6 weeks in combination with rifampin, until negative conversion was confirmed. Adequate vancomycin trough levels (>15 μg/mL) were maintained during the vancomycin treatment. Infective endocarditis was not observed and no metastatic infections were evident on repeated examination. Four months after the initial operation, the patient was transferred to a rehabilitation hospital in good clinical condition.
Case 2
A 75-year-old man was hospitalized for dyspnea on exertion. Echocardiography revealed moderate mitral regurgitation and moderate to severe tricuspid regurgitation. He underwent mitral annuloplasty and tricuspid annuloplasty, and Maze operation for concomitant atrial fibrillation. His preoperative nasal swab revealed that he was an MRSA carrier. Fever occurred 11 days after surgery, when the patient complained of retrosternal pain. A CT scan showed localized fluid collection with air density along the anterior mediastinum in the operative bed. Surgical wound debridement was performed for possible postoperative mediastinitis. Blood and wound culture revealed MRSA bacteremia that was susceptible to vancomycin.
On POD 44, we identified newly developed moderate to severe mitral regurgitation, which seemed to be due to detachment of the annular ring without any evidence of valvular vegetation. As the patient was hemodynamically very unstable, suffered an episode of cardiac arrest, and required pacing with high doses of inotropes, the mitral valve was replaced 2 weeks later on POD 61. Although gross pus and valvular vegetation were not present, and no microorganisms grew in tissue culture, blood culture taken through a central venous catheter on the day of the operation revealed recurrence of MRSA bacteremia. Surgical tissues were not submitted for histology. Postoperative bleeding accompanied by mediastinitis called for further mediastinal irrigation and the patient was placed on extracorporeal membrane oxygenation. Despite the use of vancomycin with optimal trough levels (>15 μg/mL), the MRSA bacteremia persisted for 61 PODs, and finally led to death. There was no evidence of infective endocarditis or metastatic infection on repeated examination.
The clinical courses of the two patients, including antibiotics and treatment durations, times of surgery, are displayed in Figure 1.
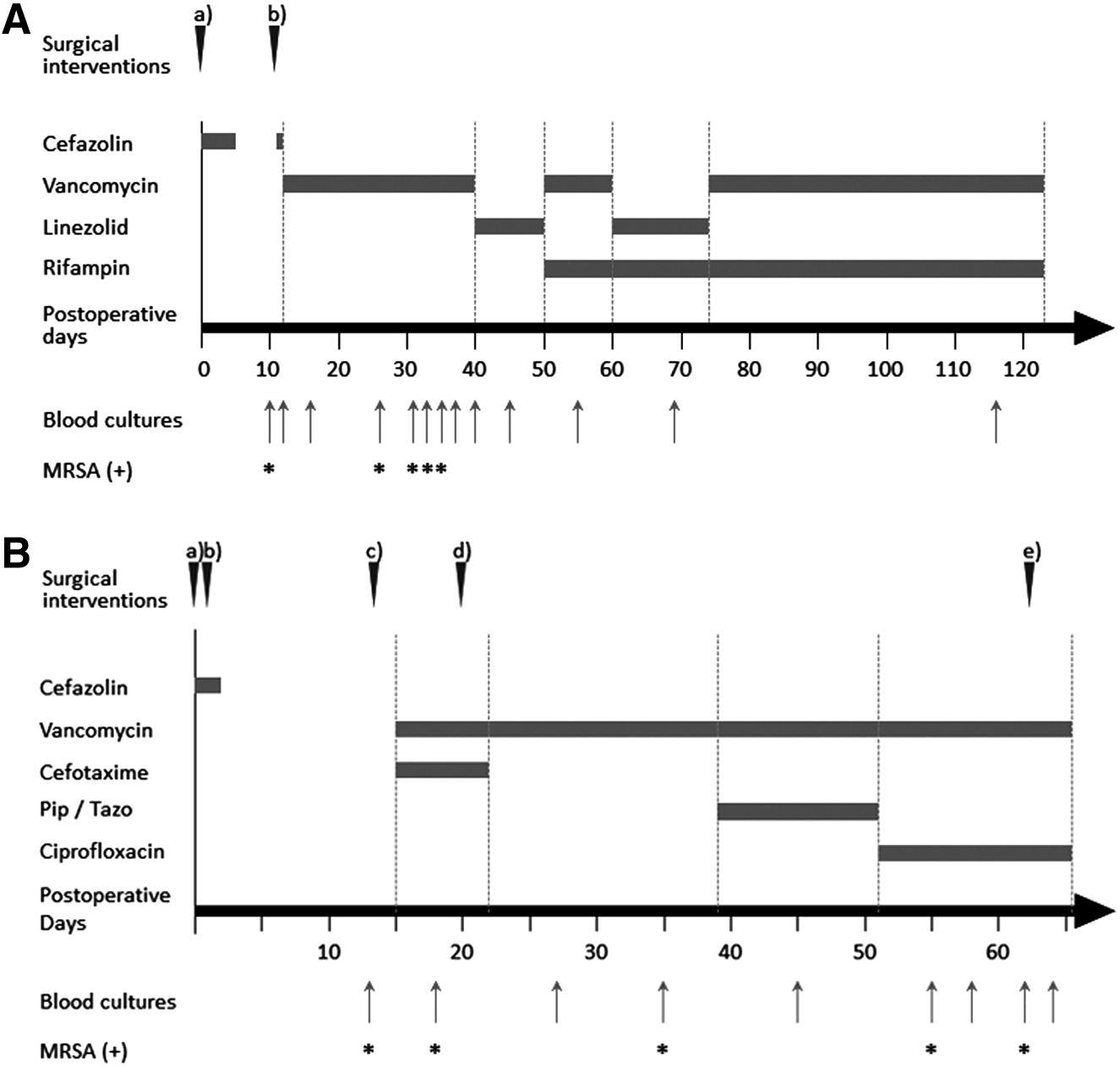
Surgical interventions and antimicrobials administered over time. Inverted arrowheads: times of surgical procedures, arrows: times of blood cultures, *blood cultures that grew methicillin-resistant Staphylococcus aureus (MRSA), Pip/Tazo: piperacillin/tazobactam.
Materials and Methods
All blood isolates from the patients were collected throughout the clinical course for identification and characterization. Species identification by semi-automated methods repeatedly revealed MRSA, however, cultures on Mueller-Hinton agar plates revealed barely any colonies and the colonies on blood agar plates had a morphology distinct from that of normal S. aureus.
Microbiological identification of SCVs
All the blood isolates were identified with the BACTEC (BD, Franklin Lakes, NJ) and VITEK 2 (bioMe´rieux, Marcy L'etoile, France) systems. MRSA was definitively identified off by means of a multiplex real-time polymerase chain reaction (PCR) assay specific for the S. aureus mecA, femA-S. aureus, and 16S rRNA genes, 21 using S. aureus ATCC 29213 as control strain.
The blood isolates were cultured in parallel on Columbia blood–agar and Schaedler agar plates (Becton Dickinson). All the agar plates were incubated at 37°C for at least 48 hr simultaneously in air and 5% CO2. SCVs were suspected phenotypically, if the clinical isolates grown on Columbia agar formed pinpoint, nonpigmented, and nonhemolytic colonies,5,11 whereas the colonies on Schaedler agar had nearly typical morphology.7,19
Auxotrophies for hemin, thymidine, and menadione were tested by the disk method. 7 Disks impregnated with hemin (10 μg/mL), thymidine (100 μg/mL), or menadione (25 μg/mL) were pressed onto Mueller-Hinton agar plates inoculated with a 0.5 McFarland standard of the isolate and the plates were incubated for up to 48 hr. To assess the dependency on CO2, the plates incubated in air were compared with those incubated in 5% CO2. An isolate was considered auxotrophic if it formed normal colonies or showed increased growth around a given impregnated disk relative to other parts of the plate following 24 hr of incubation in air at 37°C. 7
Antimicrobial susceptibility testing
Antimicrobial susceptibility tests were performed with the VITEK 2 system and interpreted according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. 22 Vancomycin minimal inhibitory concentrations (MIC) were tested by broth microdilution and E-test (AB BIODISK, Solna, Sweden), 22 using Mueller-Hinton broth supplemented with hemin (10 μg/mL). The bacteria were inoculated onto Mueller-Hinton agar at a concentration of 0.5 McFarland standards, and after incubation at 37°C in air for 24 hr, susceptibilities were interpreted according to the CLSI guidelines. 22
Population analysis profiling (PAP) to identify heterogeneous vancomycin-intermediate S. aureus (hVISA) was performed according to previously described methods 23 with slight modifications. Mu50 and S. aureus ATCC 29213 strains served as positive and negative controls, respectively. As the isolates grew poorly under standard growth conditions, we used Columbia blood–agar plates supplemented with hemin (10 μg/mL) instead of Brain Heart Infusion agar plates. Vancomycin resistance was determined from population analysis profile (PAP)-area under the curve (AUC) values: PAP-AUC ratios of ≤0.90 indicated vancomycin-susceptibility, those of 0.90–1.3 indicated heterogeneous vancomycin-intermediate resistance, and those of ≥1.3 indicated vancomycin-intermediate resistance. 23
Molecular characterization
The isolates were assessed for relatedness by pulsed-field gel electrophoresis (PFGE) with the SmaI restriction enzyme, 24 and by Staphylococcus protein A (spa) polymorphism typing. 25 Multilocus sequence typing (MLST), 26 multiplex PCR for SCCmec element, 27 typing of the agr locus, 28 and PCR to detect mutations in relA 12 were also performed as described.
To investigate whether an outbreak had occurred, we included two unrelated staphylococcal blood isolates (1 MRSA, and 1 methicillin-susceptible S. aureus) from two other patients with persistent staphylococcal bacteremia, in the PFGE analysis.
Results
We characterized nine isolates from the two patients and all were confirmed to be MRSA by multiplex PCR specific for the mecA, femA, and 16S rRNA genes. SCVs could be suspected based on the appearance of the colonies on Columbia blood–agar and Schaedler agar plates. Auxotrophy studies of all the isolates revealed hemin dependence: growth increased specifically around disks impregnated with 10 μg/mL of hemin. Auxotrophies for thymidine, menadione, and CO2 were not observed.
All the isolates had the same antibiotic susceptibility profile; they were susceptible to chloramphenicol, rifampin, tetracycline, trimethoprim/sulfamethoxazole, teicoplanin, and vancomycin, but resistant to clindamycin, erythromycin, ciprofloxacin, and gentamicin. Vancomycin MIC was 1.0 μg/mL by E-test and broth microdilution test. None of the isolates was identified as hVISA by the PAP-AUC ratio.
All nine isolates belonged to the same genotype: MLST ST5, SCCmec type II, agr type II, spa type t2460. Their SmaI restriction profiles were indistinguishable, indicating that they all belonged to the same clone, while the two unrelated staphylococci gave different band patterns. (Fig. 2) No mutations in the relA gene were identified.
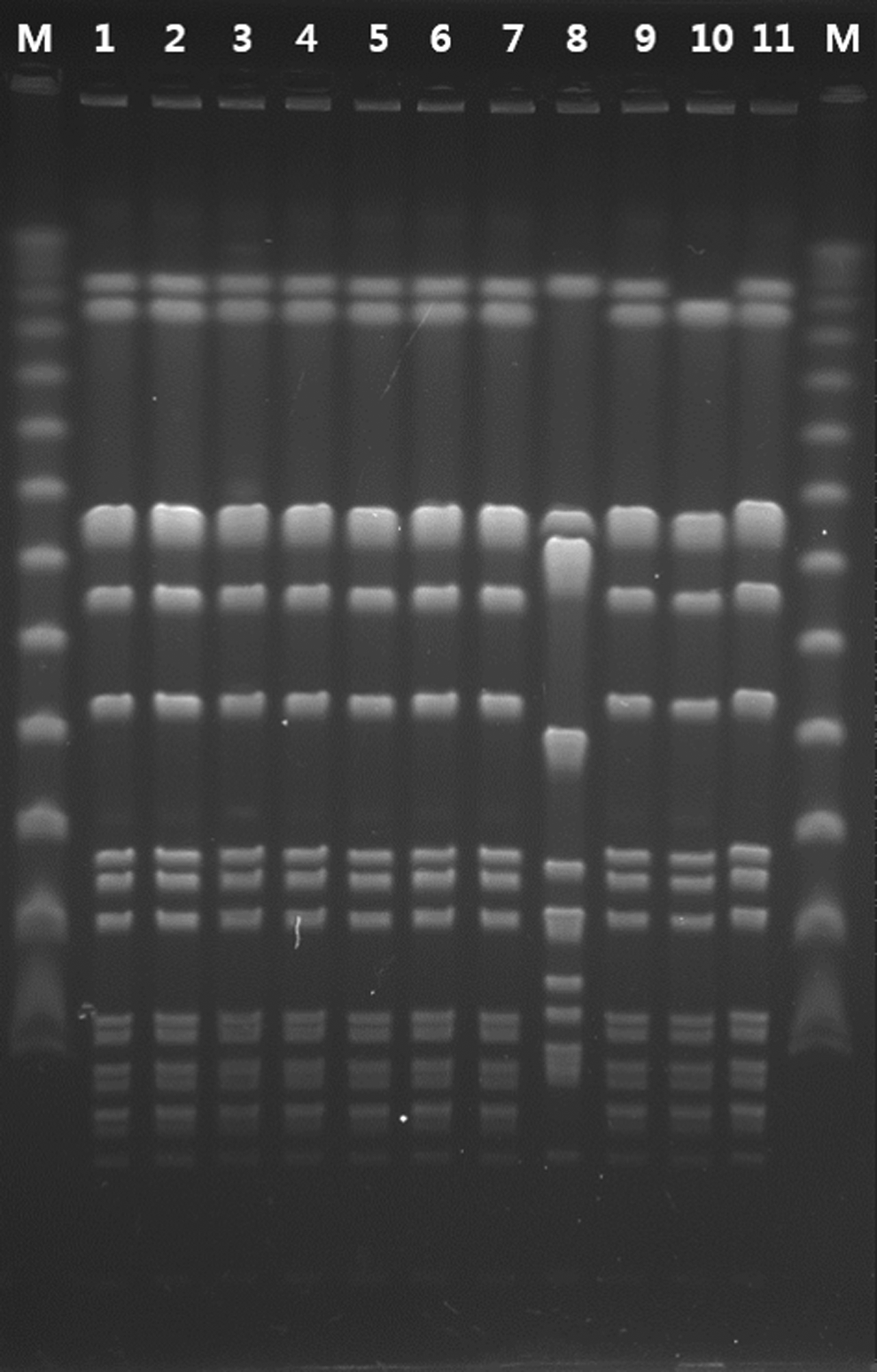
Pulsed-field gel electrophoresis of SmaI-digested DNA from the clinical isolates. M: marker. 1, 3, 4, 5, 7: MRSA isolates from Case 1. 2, 6, 9, 11: MRSA isolates from Case 2. 8: MSSA from a different patient. 10: MRSA from another different patient.
Discussion
SCVs have been increasingly reported in association with persistent infections, including bacteremia.2,5,18 In this study we describe two patients with persistent postoperative MRSA bacteremia in which the primary blood cultures yielded SCVs. The organisms, identified as MRSA by semi-automated methods, had growth patterns distinct from ordinary MRSA when grown on Mueller-Hinton agar. However, this finding was made after completion of the treatment of both patients, so the phenotype of the causative S. aureus was not taken into account during treatment. Despite appropriate medical and surgical therapy, which cleared up the primary surgical site infection (mediastinitis in both patients), the bacteremia lasted 35 and 64 days, respectively, and one of the patients did not survive. As both SCVs were isolated from patients who were admitted around the same time and had the same genotype with identical PFGE patterns, we retrospectively reviewed other S. aureus bacteremia isolates, but found no further SCVs.
Our patients harbored hemin-dependent SCVs in the absence of prolonged prior exposure to antibiotics. In one case, SCV-S. aureus grew in blood cultures obtained before empiric antibiotics were started, and in the other it grew in blood cultures after empirical cefazolin had been given for 5 days for suspected surgical site infection. This situation is reminiscent of the traditional findings of auxotrophic SCVs that have been shown to be selected by prolonged exposure to specific antibiotics and to be associated with defects in electron transport or in the biosynthesis of thymidine5,14,20,29–32
Hemin- or menadione-dependent SCVs have been frequently reported in patients with foreign body-related infections or with osteomyelitis treated with gentamicin beads,6,33 in cystic fibrosis patients who have received prophylactic aminoglycosides,7,14 and also in primary blood cultures of patients who were either on antibiotics or on structural analogs of essential nutrients. 34 The underlying mechanism has been explained as residing in their reduced sensitivity to aminoglycosides due to decreased transmembrane potential.14,15,32 Thymidine-dependent SCVs, which arise as a result of mutations in thymidylate synthase, are often found in association with long-term use of trimethoprim–sulfamethoxazole to which they have reduced susceptibility. 7
The nature of SCV emergence and persistence in the absence of antibiotic exposure has been explained by the intracellular location of the SCVs. 5 It has been suggested that after infecting host cells, pressures to survive intracellularly (by, for example, upregulating bacterial stress response regulator genes or modulating virulence factors) select for mutations causing the SCV phenotype, 29 which results in less damage to host cells due to the reduced virulence and greater resistance to intracellular host defenses.11,12,35 For example, in mixed infections with Pseudomonas aeruginosa, quorum-sensing molecules and respiratory toxins produced by P. aeruginosa appeared to be responsible for the selection of SCVs.35,36 Furthermore, a recent study showed that low pH induced the formation of nonreplicating SCVs, capable of regrowth, 34 and there is evidence that SCVs can be selected by innate host antimicrobial peptides.20,32,37
The SCV-S. aureus bacteremia in both our patients originated from postoperative mediastinitis, which required several episodes of surgical debridement. Therefore, it is possible that the low pH environment of the infected wounds, which are likely to have been poorly oxygenated, lined with fibrin, and densely infiltrated with inflammatory host cells, contributed to the selection of the SCVs. Likewise, exposure to sub-MIC concentrations of innate host antimicrobial peptides in the infected hematoma itself may also have triggered the conversion to SCVs, and the low growth rates of the SCVs may have contributed to their persistence. In addition, as mixed infections are known to account for ≤40% of cases in postoperative mediastinitis, 38 we suspect that mixed infections may also have been implicated in the selection and persistence of the SCV-S. aureus, although no other organisms were isolated from the wounds.
The nature of persistent and recurrent S. aureus infections has been explained by phenotype switching, which is regarded as a defense mechanism against hostile environment, such as those due to antibiotic treatment, nutritional deficiency, or stressful conditions.30,32,39 A recent study showed that SCV subpopulations emerge and expand during exponential growth of S. aureus by phenotype switching in a natural process that does not require any selective pressure, and that further expansion of the SCV populations occurs during growth under selective conditions. 39 Likewise, many clinical SCV isolates were reported to be phenotypically unstable, reverting to a normal appearance when grown under laboratory conditions. 19
Based on these observations, it has been suggested that the genetic changes underlying the SCV phenotype are unstable and inducible themselves. 39 However, our isolates were highly stable and did not revert to a normal appearance even after repeated subculture for over five passages. Because our SCVs, unlike most reported SCVs, arose under poor environmental conditions rather than under antibiotic pressure, we think it is possible that the nature of the mutations responsible for the phenotype may differ from those in other reported clinical strains despite their apparent hemin dependence, although we have not further sequenced the isolates. In the same way, a persistent and recurrent MRSA infection, due to a highly antimicrobial resistant SCV-S. aureus, was recently found to result from mutations in relA rather than the genes usually responsible. 12 This also supports the view that, despite their shared phenotypic and clinical characteristics, SCVs are a heterogeneous group that includes strains with distinct characteristics and underlying causes.13,40
Another important clinical issue is the difficult and often unsuccessful treatment of SCV infections, resulting from their intracellular persistence and phenotypic features leading to resistance to antimicrobials.2,5,32,33,41 There are as yet no universally accepted therapeutic strategies against SCVs, and their heterogeneous nature (common phenotypic features, but different underlying mechanisms) further adds to difficulties in developing a universal antibiotic strategy. Vancomycin is still recommended as a primary antibiotic in the treatment of MRSA infections. 42 However, its activity against SCVs has been shown to be diminished,43,44 and therapeutic failures have also been reported. 45 In a recent study, high doses of vancomycin were even shown to select for the SCV phenotype when SCV and normal phenotype S. aureus coexisted. 44 This raises concern that treatment with vancomycin may result in further expansion of the resistant SCV phenotype, and even promote persistence.
Effective regimens in the literature have often included rifampin, which has intracellular antistaphylococcal activity, 9 or fluoroquinolones, which have high in vitro activity against SCVs. 46 We were unaware of the isolates with the SCV phenotype at the time we began to treat the bacteremia in our two patients and both received vancomycin as first line therapy, plus surgical debridement as necessary. In contrast to patient 2, in whom MRSA bacteremia persisted throughout the clinical course and resulted in death, despite appropriate doses of vancomycin, patient 1 was intermittently changed to linezolid due to persistence of the bacteremia, and he also received concomitant rifampin throughout the later period of his treatment. The MRSA bacteremia was no longer detectable in patient 1 after 35 days, and he recovered from the infection.
Linezolid-based salvage therapy has been reported to be effective in persistent MRSA bacteremia, 47 but its effectiveness against SCVs has not been specifically studied. It is possible that linezolid, which penetrates tissues better than vancomycin, or rifampin with its high intracellular antimicrobial activity, 13 played a role in the successful treatment of patient 1. However, as both were started after clearance of the bacteremia, it is hard to draw any definite conclusions. Furthermore, there is a recent report of the emergence of linezolid-resistant SCV-S. aureus in a patient who had received linezolid for persistent and recurrent MRSA bacteremia 12 ; the issue of antimicrobial resistance has, therefore, to be taken into account.
SCVs pose serious therapeutic and diagnostic challenges to clinicians as a result of their altered phenotypic and metabolic characteristics. A high level of suspicion is required to detect SCVs, and although it is not common, the possibility that they are involved should be considered in persistent S. aureus bacteremia.
Footnotes
Acknowledgments
The authors thank Prof. Julian Gross (Oxford University, UK) for his help in editing this article.
This work was supported by a research grant (Study number 02-2011-027) from Seoul National University Bundang Hospital (Seongnam, South Korea).
Disclosure Statement
No competing financial interests exist.