
Abstract
Irresponsible prescription of antimicrobials (AMs) is the driving factor for the growing antimicrobial resistance (AMR) crisis. In this study, we assessed the knowledge, attitudes, perceptions, and beliefs regarding AMs and AMR together with the prescription habits of physicians in three University hospitals in Alexandria, Egypt. A 40-question survey was used. Physicians were stratified into residents and practicing staff members, and further into various departments. Clinical pharmacists at the University main hospital were included for comparative purposes. A total of 319 questionnaires were completed (response rate = 91.4%). Participants demonstrated fair average knowledge about AMs (4.71 ± 1.29 out of 7), with no significant difference between residents and staff members, whereas clinical pharmacists scored significantly higher on knowledge questions (p < 0.005). Participants showed poor awareness regarding local AMR patterns of Klebsiella pneumoniae and Pseudomonas aeruginosa (13% and 23%, respectively). AMR was perceived as a global (95%), national (97%), and local (85%) problem. High confidence regarding use of AMs was noticed with significantly higher levels among staff members (70.3% vs. 86.7%, p < 0.05). Most participants agreed that the patients' demands (78.5%) and socioeconomic statuses (76.3%) do influence their choices. The most significant knowledge deficit was regarding dosage adjustment in renal patients, and the survey highlighted poor engagement in educational activities, limited awareness of local resistance patterns, and neglect in explaining the side-effects to patients. Patients' demands and socioeconomic statuses were also shown to influence the physicians' decisions.
Introduction
A
Several factors contribute significantly to the progression of AMR in developing countries. These include—but are not limited to—errors in prescription by physicians in the form of: inappropriate selection of AMs, inappropriate dosages or durations, and wrong indications for AM therapy. These factors encourage the emergence of multiple drug-resistant strains of the bacteria, thus widening the scope of the problem. 3 Other factors include self-medication and inadequate measures of infection control, resulting in dissemination of resistant organisms throughout the hospital and community.4,5
In the present study, we assessed the knowledge, attitudes, and perceptions regarding the problem of AMR among the physicians working at Alexandria University teaching hospitals and examined their prescription habits, with the purpose of detecting contributing factors to the local problem of AMR.
Materials and Methods
Study design
Three University teaching hospitals in Alexandria were included in the current study, namely, Alexandria Main University Hospital (AMUH), with a capacity of 1647 beds; Shatby University Hospital [SUH] (specialized in Pediatrics and with 281 beds; Obstetrics and Gynecology with 302 beds); and Hadara Orthopedics University Hospital (HOUH), with a capacity of 319 beds. The hospitals represent tertiary centers in which competent microbiological analysis services are available, however, without any AM committees in any of them. The study was conducted in the form of a cross-sectional (KAP) survey during August and September 2014.
Participants and the survey
The surveys were completed on-site by residents and practicing staff members (including professors, assistant professors, lecturers, and assistant lecturers). Physicians from the departments of Radiology, Anesthesia, Psychiatry, Ophthalmology, and Physical Medicine were excluded due to the rarity with which they prescribe AMs. Participants were visited during working hours (appointments were made when required), and they were requested to hand the completed questionnaires to the researchers immediately. Assistance with completion was provided if necessary. Clinical pharmacists working in the AMUH were also included in the survey for comparative purposes. No incentives were offered for participation.
The distributed questionnaire was based on a similar survey carried out in Peru 6 after translation from Spanish by one of the authors. The minor additions were questions related to: prescribing AMs over the phone; culture and sensitivity testing; the causes of AMR; and suggested interventions to tackle AMR. A pilot survey of 40 participants was conducted before starting the survey to assess its duration, clarity and order of the questions. Several questions were omitted as inappropriate for the local context and to limit the duration of the survey, resulting in a total of 40 questions (Supplementary Table S1; Supplementary materials are available online at www.liebertpub.com/mdr).
Different aspects were evaluated throughout the survey, including the level of medical experience, rate of AMs prescription, beliefs and perceptions related to AMR, sources of information on AMs, confidence regarding their current practices, factors affecting their prescription and the choice of AMs, and the need for interventions and their applicability.
Three hundred and fifty questionnaires were distributed. Participants were sampled in a stratified randomized manner: First, they were stratified into residents and practicing staff members (University staff members sharing in the process of patient care), then into various departments, and finally, randomly selected within each category through an online randomization tool available from: www.randomizer.org.
The Likert scale was used (4 or 5 points). Seven questions were used to assess knowledge, three of which involved problem solving. The awareness of the physicians regarding local AMR rates was assessed through two questions on the resistance of Klebsiella pneumoniae to third-generation cephalosporins and the resistance of Pseudomonas aeruginosa to ciprofloxacin in all types of samples during the period from July 2013 to July 2014. The actual rates of resistance were obtained from the central microbiological laboratory at AMUH.
Ethical approval
Approval from the faculty of medicine, Alexandria University to conduct the survey was obtained. No informed consent was obtained from the participants, and the data were collected in an anonymous manner.
Statistical analysis
Data were analyzed by using IBM SPSS Statistics 22 software. Descriptive statistics, including frequency, percentages, arithmetic mean (
Results
Demographics and occupational characteristics
Out of 350 participants, 319 responded (response rate = 91.14%), of which 46% (n = 148) were residents, 40% (n = 128) were staff members, and 13.5% (n = 43) were clinical pharmacists. Of these, 99% (n = 315) agreed that knowledge and appropriate use of antibiotics is important in their clinical practice, and nearly 60% (n = 188) prescribed antibiotics more than once per day. Table 1 shows the occupational characteristics of the participants in relation to their professional category and the AM prescription rates. Significant associations were found between professional category and working in a certain department (p = 0.001) as well as years of experience (p = 0.001).
The Chi-square statistic is significant at the 0.05 level.
Others include pulmonology, dermatology, otolaryngology, tropical medicine, and medical oncology departments.
Knowledge and awareness regarding AMs and local AMR patterns
From the seven questions answered, the average knowledge score was (4.71 ± 1.29). The questions that had the lowest frequency of correct answers were those assessing the need for dose adjustment in patients with renal impairment, to which only 129 participants (41%) correctly answered that the prescribed dose of Ceftriaxone and Gentamycin needs to be reduced; the question regarding antibiotics that cross the blood–brain barrier, to which only 43% (n = 136) answered “Ceftriaxone”; and finally, the question regarding the antibiotic choice in a case of upper respiratory tract infections (URTIs), which was correctly answered by only 147 participants (47%).
On the other hand, most participants (95%, n = 305) agreed that amoxicillin is a safe drug during pregnancy, 93% agreed that metronidazole has increased activity against anaerobes, 85% (n = 269) correctly answered that no treatment is needed in case of non-febrile diarrhea, and 82% (n = 262) agreed that neither Cephalothin, Cefuroxime nor Ceftriaxone is effective against Methicillin-resistant Staphylococcus aureus. The department with the best knowledge score was the department of Cardiothoracic Surgery (5.57 ± 0.98), followed by the departments of Internal Medicine (5.47 ± 1.3) and Emergency Medicine (5.33 ± 1.15). On the other hand, the lowest score was found among physicians in the department of Neurosurgery (3.58 ± 1.38).
No significant difference in knowledge was noted between residents and staff members except for the question regarding the activity of Metronidazole against anaerobes (p = 0.012), which was more likely to be answered correctly by staff members. On the other hand, a significant difference in knowledge was noted between clinical pharmacists and physicians regarding the need for dose adjustment in renal patients (81% of clinical pharmacists answered correctly vs. only 37% of physicians with p < 0.05). A significant difference was also noted between the two groups regarding antibiotics that cross the blood–brain barrier (p = 0.03), to which only 36% of physicians answered correctly versus 61% of clinical pharmacists. The average knowledge score for clinical pharmacists was higher than that for all other hospital departments (5.6 ± 1.09). No significant difference in knowledge was noted between physicians in the three hospitals studied.
Regarding awareness about local AMR rates, 40% of participants (n = 128) reported that they did not know the level of resistance of K. pneumoniae to third-generation Cephalosporins in their hospital, and only a few (13%, n = 42) were aware that it was very high (>90%). Similarly, nearly 41% (n = 141) did not know the level of resistance of P. aeruginosa to Ciprofloxacin, and only 23% (n = 75) were aware that it was high (50–90%). No significant difference was noticed between clinical pharmacists and physicians regarding awareness about local AMR rates, whereas significant difference was noted in the awareness level between staff (19%) and residents (30%) regarding level of resistance to P. aeruginosa (p = 0.026).
Beliefs and perceptions of the problem of AMR
Almost all participants (98%) agreed that antibiotics were overused in the community in Egypt, whereas 91% stated that antibiotics were overused in their hospital and other hospitals in Egypt. This coincides with their perception that AMR is a global problem (95%), that AMR is a problem at the national level (nearly 97%), and that it is a problem in their daily practice (85%). Regarding the major factor behind AMR, inappropriate indication was the most frequently reported (62.5%) followed by self-medication (17%) (Fig. 1).
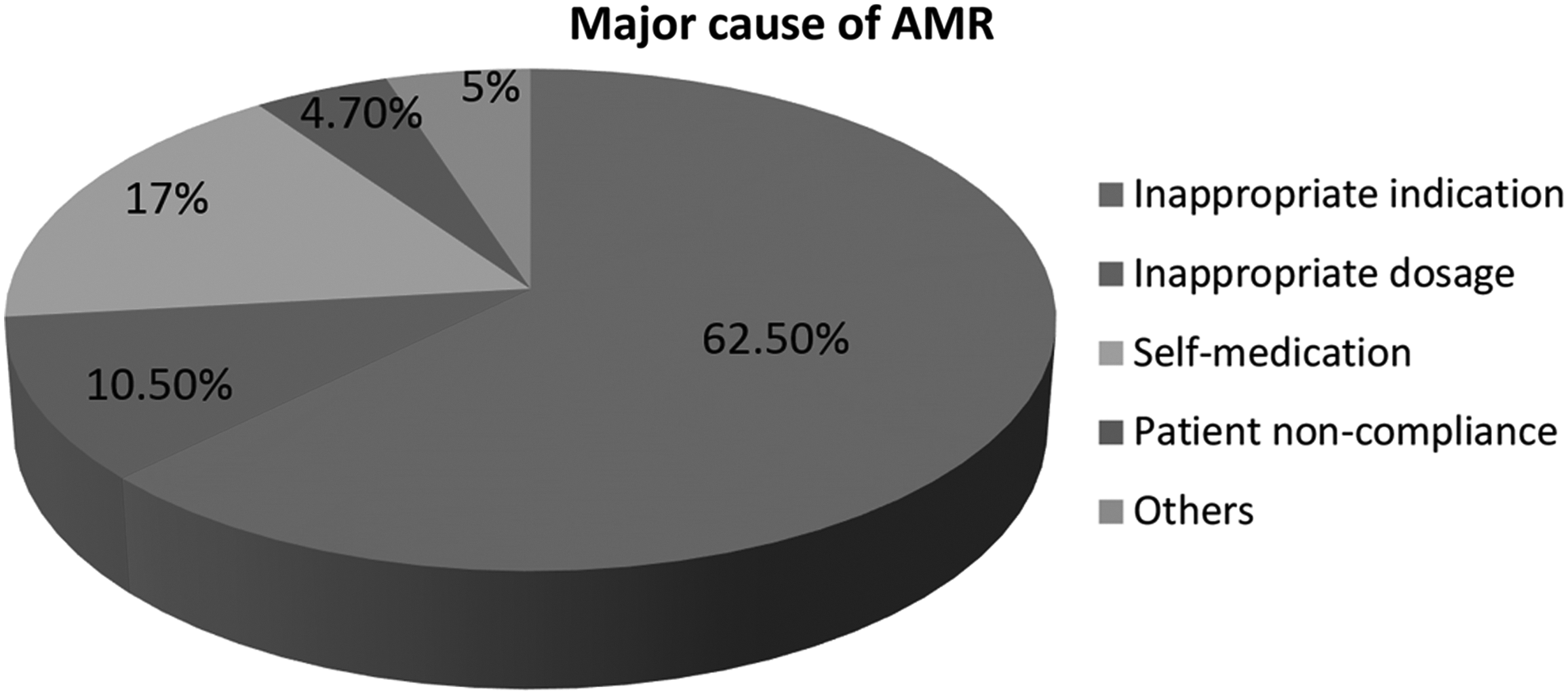
Major cause of AMR. Frequency distribution of responses regarding the major cause behind AMR crisis. AMR, antimicrobial resistance.
Interestingly, 57% of residents (n = 84) and only 43% of staff members (n = 55) stated that it is difficult to correctly select an antibiotic (p = 0.035). No significant difference was found between residents (75.7%) and staff (76.6%) regarding disagreement that no damage is done if antibiotics are prescribed when patients do not really need them.
Confidence and seeking input
Among residents, 70.3% (n = 104) were confident regarding the optimal use of AMs compared with 86.7% of staff members (n = 111), p = 0.001. Such a high level of confidence coincides with the finding that nearly most participants (75%) either never or only sometimes review their choice with a colleague, who, in turn, either never or only sometimes recommends a different AM therapy (reported by nearly 80% of participants).
Continuous education and sources of information
Almost all participants (91.5%) agreed that general knowledge related to AMR should be considered when prescribing antibiotics. Nearly 88% of residents (n = 129) and 84% of staff members (n = 107) attended conferences or lectures less than three times during the previous year, and the vast majority of both (nearly 70%) did not participate in any related courses during the preceding year. Despite this, most residents (68%, n = 100) and staff members (73.4%%, n = 94) believed that they had enough sources for information about AMs. Figure 2 shows frequency distribution between residents and staff regarding usefulness of the different sources of information. A significant difference was found between staff members and residents regarding the usefulness of pocket guides or mobile applications (p = 0.022), which were rated to be more useful by residents. Nearly three quarters of residents (n = 111) and 63.3% of staff members (n = 81) were not familiar with the Sanford guide®. Furthermore, a high percentage of residents (63.7%, n = 93) and staff members (61.7%, n = 79) reported that they were not familiar with any Egyptian national guidelines for AM prescriptions.
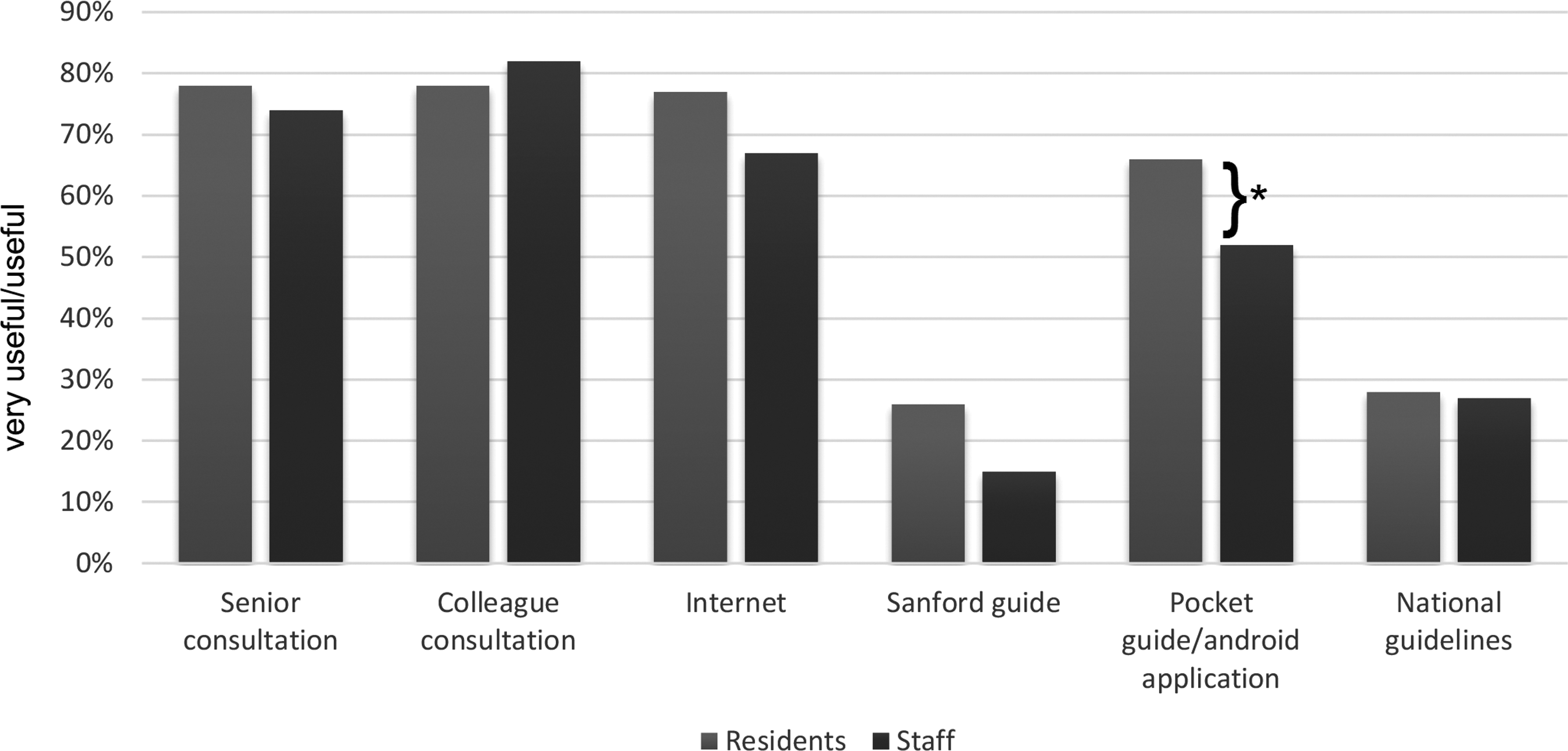
Sources of information. Comparing frequency distribution between residents and staff regarding usefulness of the different sources of information (*p < 0.05).
Practice and prescription habits
Nearly 43% of residents and 48% of staff either never or only sometimes performed culture and sensitivity testing, whereas most of the participants (92.6% of residents vs. 90.7% of staff) either never or only sometimes prescribed AMs over the phone. On the other hand, significant difference was found between staff and residents regarding the explanation of side-effects to patients (p = 0.015); 78% of residents and 64% of staff either never or only sometimes explained the side-effects to their patients. Considering their decision if the prescribed AMs were not efficient, 31% of residents versus 41% of staff members would perform culture and sensitivity testing whereas 27% of residents versus 18% of staff members would empirically select a different antibiotic. Only 42% of participants either always or most of the time read the pamphlets of new medications. Also, 55% agreed that they needed to seek approval before selecting certain antibiotics whereas 16.5% stated that there were no restrictions in their hospital.
Regarding factors that influence their decision, most residents (79%) and staff members (77%) agreed or strongly agreed that a patient's request would influence their decision. Overall, 83% of residents and 70% of staff members agreed or strongly agreed that the socioeconomic class of the patient would influence their decision, whereas only 22% of residents and 26% of staff members stated that expiry or availability of drugs did influence their decision. On the other hand, 42% of residents and 43% of staff members agreed that decreased efficiency of antibiotics is mostly due to poor quality of medications in their hospital.
Acceptability of potential interventions
Almost all residents (93%) and staff (83%) reported that they would like to have educational programs about AMs and AMR. At the same time, 66.5% of residents and 83% of staff agreed that the development of local AM guidelines would be more useful for them than international ones.
Further highlighting the importance of this, participants considered development of local guidelines (26%) and education of physicians (25%) to be the most important preventive measures against AMR (Fig. 3).
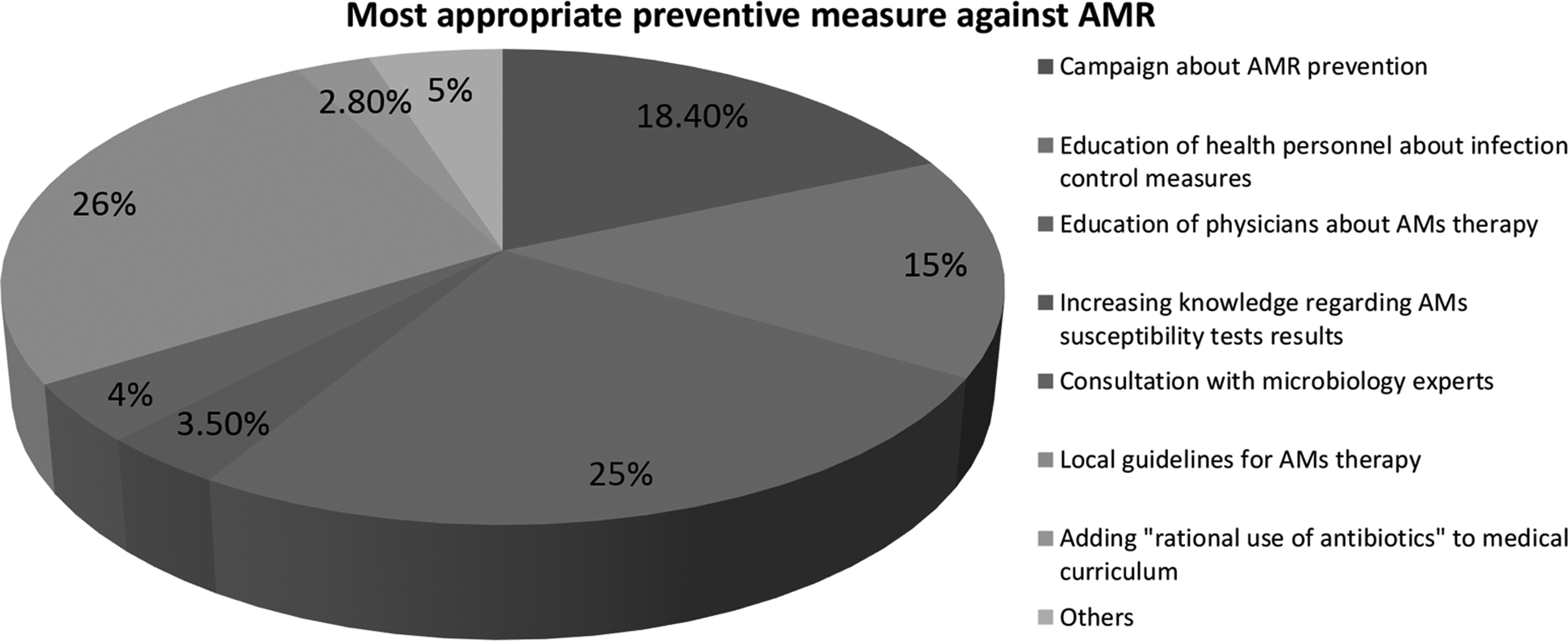
AMR preventive measures. Frequency distribution of responses regarding the most appropriate preventive measure of AMR. AMs, antimicrobials.
Discussion
The threat of AMR has been increasing for decades, with the range of resistant bacteria continuously enlarging. AM misuse is the single most significant factor contributing to the worldwide AMR. Up to 50% of AM prescriptions are either not indicated or inadequately prescribed, thus exerting a biological pressure on bacteria and leading to the development of AMR. 7
According to the World Health Organization (WHO), data from countries in the Mediterranean region are insufficient for efficient policy and strategy making. 1 Although a recent study documented that 60% of AMs used for medical prophylaxis in Egyptian hospitals have no valid medical justification, 8 there is no written national strategy promoting AM stewardship at the present time.9,10 Strategies targeting a sustained change in AM prescriptions mandate alterations of the daily behavior and perceptions of physicians. Studies have shown that physicians' awareness and acceptance of the suggested modifications are required to achieve these changes. Therefore, physicians must recognize the deficiencies in their knowledge, beliefs, attitudes, and daily practices involving AMs. Their perspectives regarding specific interventions should also be investigated to enable the design of realistic approaches.11–13
In this study, we aimed at examining the knowledge, attitudes, beliefs, and perceptions regarding AMs and AMR among physicians from a wide variety of specialties, with variable experience profiles, and who care for in-patients in high-flow tertiary hospitals in Egypt. At the same time, we analyzed their prescription habits and the factors influencing their behaviors in a comparative fashion as the first step for planning efficient local interventions. To the best of our knowledge, this represents the only study investigating these factors in Egyptian hospitals.
Three University teaching hospitals were included in the present study, with a wide variability of specialties, age sectors, and experience profiles (Table 1). Practicing staff members were included in this study, because they participate in the patient care and decision making in Alexandria University hospitals as either specialists or consultants. They are considered experts in their specialties in different private and governmental hospitals in Alexandria where they provide guidance to students and junior physicians. Clinical pharmacists working at AMUH were also included for comparative purposes regarding knowledge and awareness. An unpredicted high response rate of 91.14% was achieved, although the survey was performed during the working hours. A high percentage of the participants prescribed AMs more than once per day (58.1% of residents and 54.7% of staff members).
Knowledge and awareness regarding AMs and local AMR patterns
Fair theoretical knowledge was noted among physicians (4.71 ± 1.29 out of 7) in spite of the insufficient educational activities about AMs and AMR. Although this knowledge score (67%) is higher than the one achieved in a similar study in DR Congo (61.25%), 5 it is much lower in comparison with another similar study performed in Lima, Peru (6 ± 1.3 out of 7). 6 Furthermore, theoretical knowledge among clinical pharmacists proved to be significantly better than among physicians. This can be probably explained by their better understanding of the underlying pharmaco-kinetics and modes of action. There was no significant difference between knowledge among residents and staff members, which highlights the lack of a continuous medical education system and therefore the lack of a significant improvement. Surprisingly, such continuous medical education is not legally mandatory either for the physicians or for the nurses in Egypt.9,14 No significant difference was noted between the three hospitals involved despite the variable specialties included, a finding that further emphasizes the reliance on the common undergraduate education. Analysis showed that the question regarding dosage adjustment in renal patients had the highest frequency of wrong answers. This should stimulate better consideration of this topic in curricula due to its high significance and clinical implications.
The lack of awareness among most of the physicians regarding the local AMR patterns in their hospitals was evident. This can be explained by the lack of communication between the well-equipped central microbiological laboratories and hospital physicians. Updates regarding local AMR patterns should be made available for physicians, as they can significantly alter their decisions. Additionally, awareness among residents proved to be significantly better than among staff members. The stronger engagement in daily patient care and local culture and sensitivity testing results can explain this finding. Again, knowledge of these details was better in the Peruvian study. 6 It is worth mentioning that the high level of resistance of K. pneumoniae to third-generation Cephalosporins reported by the local microbiological laboratories coincides with proportions reported worldwide, exceeding 50% in all WHO regions. 1
Beliefs and perception of the problem of AMR
It was evident that the problem of AMR was perceived by participants as both a global and a local issue. This finding represents a good starting point for launching targeted interventions. Participants believed that the most important factors contributing to the worsening of AMR are: inappropriate indications for therapy (62.5%) and self-medication (17%). Surprisingly, almost 25% of participants believed that no harm will result if AMs are prescribed without a real need. This finding reflects the lack of awareness of this fraction regarding the etiology of AMR and its vital role in delaying its progression.
Confidence and seeking inputs
Despite the choice of AM being evidently perceived as a difficult decision, overall confidence levels among participants were found to be high. Higher confidence levels among staff members can be attributed to their greater experience rather than to a significant improvement in knowledge regarding AMs. This is supported by similarly high confidence levels reported in other similar studies despite variations in knowledge.5,6
Continuous education and sources of information
Analysis showed poor engagement of participants in educational activities related to AMR (70% did not participate in any related activity during the year preceding the survey). In view of the evident high acceptance of receiving AMR-related education and the high perception among participants of AMR as a global and a local issue, this poor engagement can possibly be explained by absence of relevant educational programs rather than by poor participation. In fact, only one lecture about AMR targeting the included hospitals' physicians was conducted during the year of the present study.
Most participants believe that they have sufficient sources of information regarding AMs, with variable preferences. Mobile applications and international pocket guides were significantly more popular among residents compared with staff members. Consideration of these preferences is required to design practical interventions. Results also highlight the reliance on external sources for information rather than local microbiological studies, as most of the participants were not familiar with any national guidelines. In fact, no local guidelines for AMs prescription are currently adopted in the studied hospitals, although a preliminary draft was prepared by Intensive Care consultants in 2011.
Practice and prescription habits
Analysis showed that performance of culture and sensitivity testing was not common during the primary assessment. This practice can be explained by the nature of the studied hospitals as tertiary centers where physicians are commonly confronted by advanced medical conditions necessitating immediate empirical AM therapy. The extended period between ordering and receiving the results of culture and sensitivity testing could also be a contributing factor. However, it was chosen as the most common response when no improvement was achieved with the prescribed AMs, with shifting to a different AM chosen second in the same context.
Most of the participants (around 90%) stated that they did not prescribe AMs over the phone, which is considered a good practice in view of the common habit of phone consultation by the discharged patients (due to their frequent non-compliance with follow-up visits). On the other hand, the majority of participants did not consistently explain the side-effects of the medications to the patients, a factor that can contribute to both risky patient behavior and self-medication. This finding was significantly worse among residents. This may be explained by the high patient inflow, limited time spent with individual patients, and long working hours.
The majority of participants admitted that the patient request for AMs and the socioeconomic status of the patient do influence their decision. This should drive the conduct of public campaigns promoting awareness of the side-effects of AMs and the grave consequences of AMR, which are parallel to targeting the medical community. The development of a more efficient health insurance system and the encouragement of production of high-quality yet affordable generics could also help alleviate the concern regarding the socioeconomic statuses of the patients, thus allowing for optimal choice of AM therapy. On the other hand, the influence of availability, expiry dates, the need to seek approval, and hospital restrictions were less evident.
Around 42% of the participants believed that decreased efficiency of antibiotics was the result of the poor quality of medications in their hospital. Generics can sometimes be perceived by physicians as inferior to the original medications, 15 and around 70% of the AMs available for in-patient prescription were generics during the period of the survey. In Egypt, a functioning quality control system is available for licensed medications. 9 However, analysis of the efficiency of the current quality control protocol and its perception is beyond the scope of this study. In view of the evident unawareness of local AMR levels and the reported prescription habits, the poor efficiency of prescribed AMs can be attributed to other etiologies rather than to the quality of AMs. Nevertheless, this finding definitely sheds light on the lack of trust in locally provided medications, which should stimulate the efforts of the ministry of health, hospital administration, and pharmaceutical companies to strengthen the trust of physicians in the AMs available.
Acceptability of potential interventions
A strong desire to receive educational programs about AMs and AMR was evident among participants. The majority also agreed that local guidelines based on the local microbial patterns would be more useful than international ones.
Guidelines for developing an institutional program to enhance AM stewardship published in 2006 stated that, although education is an essential part of any AM stewardship promoting programs aiming at improving prescription practices, “education alone, without incorporation of active intervention, is only marginally effective in changing AM prescribing practices and has not demonstrated a sustained impact.” 16 Other reports have shown considerable improvements during intervention studies that were mainly based on education of the physicians. 10
The ability of local practice guidelines to improve the usage of AMs has also been highlighted. This should be based on local microbiological studies and microbial resistance patterns. Continuous healthcare provider education and feedback of AMs usage and their outcomes can facilitate the development of valid local guidelines. 16
Despite the presence of an active infection control committee in the hospitals studied, the promotion of AM stewardship and auditing of the prescription practices is not included in its duties. Currently, there are no AM committees in any of the hospitals studied despite the presence of national regulations that require the organization and development of drug committees.9,14 Similar circumstances were also noted in several other Egyptian hospitals during a recent study. 10
Conclusions
Identification of the key local factors leading to AMs misuse is necessary to outline effective interventions against AMR. Poor knowledge regarding AMs dosage adjustment in renal patients, limited awareness of local AMR patterns, poor engagement in related educational activities, neglect in explaining the side-effects to patients, and the influence of patients' demands and socioeconomic statuses on the AM prescription were the most evident problems identified by the present study.
Future interventions
The Center for Disease Control and Prevention (CDC) has outlined four main interventions to hinder the progress of AMR to critical levels: prevention of infections and the spread of AMR, improving the use of antibiotics, tracking and surveillance of resistant bacteria, and the development of new antibiotics and investigations for resistant organisms. 7 Among these, the consistent commitment of physicians to prescribe AMs only when indicated for disease treatment or prevention, or “AM stewardship,” is clearly the easiest and the most feasible approach.
A full understanding of the magnitude of AM misuse and the factors underlying inappropriate prescriptions is necessary to allow the design of effective national policies, and this will require multi-centric collaboration and research. Based on the results of the present survey, targets of potential interventions include: provision of educational and training programs targeting AM prescribers with the aim of improving their theoretical knowledge about AMs. Special emphasis on detected deficiencies (e.g., dosage adjustments in renal patients) and correction of their faulty prescription practices should be included. It also highlighted the need to periodically inform physicians of the local AMR patterns and to develop local AM guidelines. The physicians' lack of confidence in local AMs can be improved by an effective quality control system. Conducting public awareness campaigns about the side-effects of AMs and the problem of AMR is necessary to decrease patient demand for AMs. Strengthening the role of health insurance can allow physicians to choose the optimal AM regardless of the socioeconomic status of the patients. Finally, clinical pharmacists should be encouraged to share in the process of local promotion of AMs stewardship.
Footnotes
Acknowledgments
This study was a part of “Innovation project” in collaboration with Bibliotheca Alexandrina and AlRazi project for research development.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.