
Abstract
The aim of the study was to investigate the molecular epidemiology of Staphylococcus epidermidis in Iranian hospitals and to compare the genotypes with a previously characterized collection of >1,300 S. epidermidis isolates of nosocomial and community origin from Northern Europe, Australia, and USA. In total, 82 clinical S. epidermidis isolates from three Iranian hospitals were examined by multilocus sequence typing, pulsed-field gel electrophoresis (PFGE) and staphylococcal cassette chromosome mec (SCCmec) typing. In addition, antimicrobial susceptibility, the presence of the ica operon, and the predilection to biofilm formation were assessed. Three predominant PFGE clones were found. The PFGE patterns of the most common sequence type (PFGE type 040-ST2) showed 80% similarity to multidrug-resistant S. epidermidis (MDRSE) clinical isolates from eight hospitals in Northern Europe. The second most common (PFGE 024-ST22) showed an unique PFGE pattern, whereas the third most predominant genotype (PFGE 011-ST5) proved indistinguishable to the PFGE Co-ST5 identified in five hospitals in Northern Europe. In conclusion, the study documented the dissemination of three MDRSE clones within and between hospitals in Iran and revealed an intercontinental spread of two clonal multidrug-resistant lineages (ST2 and ST5) in the hospital environment. Isolates of the predominant clones were significantly more frequently associated with multidrug-resistance and biofilm formation compared to nonclonal isolates. Further studies are needed to explore and characterize the genetic traits that enable these successful MDRSE clones to persist and disseminate worldwide in the healthcare settings.
Introduction
I
Notably, at present more than 70% of healthcare-associated S. epidermidis are methicillin-resistant, which is of concern and limits the options for effective antimicrobial treatment.7–9 Resistance to methicillin is mediated by the mecA gene carried on the staphylococcal cassette chromosome mec (SCCmec). It has been suggested that the frequent loss and acquisition of SCCmec elements in S. epidermidis accounts for the prevalence of different SCCmec types in closely related strains.6,7
Several studies have reported the intrahospital and occasional interhospital endemic occurrence of a few well-adapted, highly resistant S. epidermidis lineages.4,10–12 Moreover, there is limited evidence of wide geographic dissemination of epidemic clonal lineages of S. epidermidis between countries.13–16 To obtain a more complete picture of the worldwide occurrence and spread of healthcare-associated S. epidermidis lineages, more molecular epidemiology data is needed from the Middle East, for example from the most populous country in this region, Iran. In this respect, molecular typing can help to identify clonal or sporadic dissemination and subsequently can be helpful to address more effectively the related infections. Pulsed-field gel electrophoresis (PFGE) has been utilized as the most discriminatory method for genotyping of staphylococcal strains and widely been used for hospital outbreak investigations. 17 To predict long-term evolutionary relationships, multilocus sequence typing (MLST) is the recommended method. 6
This study was aimed to characterize clinical S. epidermidis isolates from Iranian hospitals, using both genotypic and phenotypic methods and to track the epidemic spread of these isolates. The Iranian isolates were compared with a previously characterized collection of S. epidermidis strains from nosocomial and community origin in northern Europe, Australia, and USA.
Materials and Methods
Bacterial isolates
From a total of 177 clinical coagulase-negative staphylococci (CoNS) collected from February 2012 to December 2013, 82 nonrepetitive S. epidermidis isolates were included in this study. This collection contained 42 isolates from a pediatric teaching hospital in Tabriz (Tabriz, north-western Iran, coded “T”) and 40 isolates from two hospitals in Tehran: 21 isolates from a referral pediatric university-affiliated hospital (Tehran, central Iran, coded “MT”), and 19 isolates from a tertiary care hospital (coded “M”). The majority of the isolates, 77% (63/82), were collected from neonates and children (≤10 years of age) (Table 1).
T, a pediatric teaching hospital; MT, a referral pediatric university-affiliated hospital; M, a tertiary care hospital.
F, female; M: male; d, days; y, years; B, blood; C, catheter; CSF, cerebrospinal fluid; E, eye; P, peritoneal fluid; S, shunt; T, tracheal tube; U, urine; W, wound.
Most isolates, 67% (55/82), were obtained from blood cultures and <10% each originated from other sources (Table 1). Clinically significant isolates were determined in accordance with criteria defined by Center for Disease Control and Prevention for determination of nosocomial infection 18 and those proposed by Stoll et al. for diagnosis of invasive blood culture isolates in neonates. 19 S. epidermidis isolates from a monobacterial positive blood culture were defined as infecting isolates in neonates when combined with C-reactive protein >10 mg/L. For non-neonates two positive cultures out of a set of two separately collected bottles were defined as infecting isolates. Also, S. epidermidis from normally sterile internal fluids or from foreign bodies in pure primary cultures were considered as infecting isolates.
Species identification and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry
Identification of CoNS was performed primarily using standard laboratory methods with further identification to species level by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). In summary, isolates were cultured overnight at 35°C in air on blood agar as previously described.20,21 Colonies of bacteria were identified using the MALDI-TOF MS according to the manufacturer's protocol (Bruker Daltonics).
Antimicrobial susceptibility testing
Antimicrobial susceptibility testing was performed by disk diffusion using the following antibiotics: gentamicin (10 μg), erythromycin (15 μg), clindamycin (2 μg), ciprofloxacin (5 μg), cefoxitin (30 μg), trimethoprim/sulfamethoxazole (1.25/23.75 μg), fusidic acid (10 μg), and linezolid (30 μg) (MAST). For vancomycin, minimum inhibitory concentration (MIC) value was determined using the Liofilchem® MIC test strip (Liofilchem). The results were interpreted according to criteria defined by the Clinical and Laboratory Standard Institute (CLSI) guidelines. 22 For fusidic acid, susceptibility breakpoint proposed by Deveci et al. was used. 23 Multidrug-resistance (MDR) was defined as resistance to at least four different classes of antibiotics. 10
Semiquantitative biofilm assay
Biofilm formation was quantified using a microtiter plate assay as described previously. 24 Overnight grown cultures were diluted 1:100 in trypticase soy broth (Merck) supplemented with 0.25% glucose, of which 200 μl was inoculated into 96-well microtiter plates (Greiner CELLSTAR Bio-One B.V). After incubation at 37°C for 24 hours, the bacterial suspensions were gently removed and the wells were washed three times with 200 μl saline to remove bacteria that had not adhered to the biofilm before staining with 0.1% safranin (Merck) solution. After 30 seconds, the excessive dye was removed by rinsing the wells three times with 200 μl sterile distilled water. The plate was allowed to dry and the biofilm-bound-safranin was extracted by addition 200 μl of 95% ethanol and the absorbance was measured at 490 nm using a microplate reader (BioTek, ELX 800; Winooski). An optical density ≥ 0.17 was considered as biofilm formation. S. epidermidis ATCC 12228 and S. epidermidis RP62A were used as negative and positive controls, respectively.
Detection of the ica operon
DNA extraction was performed by the Cetyitrimethylammonium Bromide (CTAB) method 25 and all isolates were examined for the presence of ica operon by PCR amplification. 26
SCCmec typing
All mecA-positive isolates detected by PCR 27 were characterized as SCCmec types I-V using multiplex PCR as previously described. 28 Isolates, which showed unrelated patterns, were classified as nontypeable.
PFGE and MLST
DNA was prepared from 3 mL S. epidermidis overnight cultures in Todd Hewitt broth (Difco Laboratories) as previously described. 15 The DNA was digested using SmaI (Thermo Scientific) and the DNA fragments were separated by PFGE in a GenePath apparatus (Bio-Rad Laboratories) using Program 14, for 19.7 hours according to the manufacturer's instructions (Bio-Rad). Gels were stained in 1 mg/L ethidium bromide, destained, and photographed under UV illumination. Genetic similarity between isolates was calculated using GelCompar II 4.0 (Applied Maths) using the Dice coefficient, and the unweighted pair group method with arithmetic mean (UPGMA) with 1.3% tolerance and 0.8% optimization settings. S. aureus NCTC 8325 was included as a reference in every sixth to seventh lane to allow normalization of the electrophoretic pattern. Band sizes below 36 kb were not analysed. 29 PFGE types were visually identified according to established criteria, isolates with more than three-band variation in the PFGE pattern were defined as genetically unrelated. 30 This corresponded to a similarity coefficient of 90% using the cluster analysis. PFGE types were assigned arbitrary numbers (001, 002, 003…) and isolates with 1–3 band differences were assigned to PFGE subtypes (numbers with letter codes, 001a, 001b, 001c…).
MLST was performed as previously described. 15 Selected isolates from each PFGE type that included ≥3 isolates were analyzed by MLST. Sequence types (STs) were assigned using the S. epidermidis MLST database (www.mlst.net).
The PFGE patterns of the 82 studied isolates were compared with a previously in part described compilation of 1,315 S. epidermidis isolates,11–13,15,31 of which >90% were methicillin-resistant S. epidermidis (MRSE). The collection contained healthcare-associated S. epidermidis collected from 1994 to 2012 at the Umeå University Hospital (498 isolates), the Östersund Hospital in northern Sweden (479 isolates), as well as isolates from nine other northern European hospitals (149 isolates) and Royal Perth Hospital, Australia (27 isolates). In addition, a collection of nonhealthcare-associated nasal or hand colonization S. epidermidis isolates were included from Umeå (124 isolates) and VA Medical Center, Medical University of South Carolina, Charleston, SC (38 isolates kindly provided by Dr. Joseph F John). All PFGE analysis in the present study as in the PFGE collection was carried out at the Department of Clinical Microbiology, Umeå University Hospital, Umeå, Sweden.11–13,15,31
Ethical approval
The study was approved by the regional ethics board at Tabriz University of Medical Sciences.
Statistical methods
Statistical analysis was performed using the software IBM SPSS Statistics version 21. The chi-square test was used to compare the characteristics of isolates in predominant clonal genotypes with nonclonal ones. A p-value of <0.05 was considered statistically significant.
Results
Eighty-two isolates of S. epidermidis were included. The distribution of isolates in infecting (I) and noninfecting (N) groups was 73% (60/82) and 27% (22/82), respectively (Table 2). Overall, 74% (61/82) of the S. epidermidis isolates were methicillin-resistant. The antimicrobial resistance rates were as follows: erythromycin (78%), trimethoprim/sulfamethoxazole (78%), clindamycin (76%), ciprofloxacin (57%), gentamicin (49%), and fusidic acid (27%). No resistance to vancomycin and/or linezolid was found. MDR phenotype was found in 67% (55/82) of the isolates (Table 2).
Biofilm formation determined by MTP assay.
Predominant genotypes include: PFGE 011-ST5, PFGE 024-ST22 and PFGE 040-ST2.
T, a pediatric teaching hospital, Tabriz, MT, a referral pediatric university-affiliated hospital, Tehran.
M, a tertiary care hospital, Tehran.
GM, gentamicin; E, erythromycin; CD, clindamycin; FA, fusidic acid; CIP, ciprofloxacin; TS, trimethoprim/sulfamethoxazole; MDR, multidrug resistance.
Molecular analysis
DNA macrorestriction analysis of the 82 isolates revealed 42 different PFGE types, of which 34 types were singletons (Fig. 1). Three dominant PFGE types were detected (presented with corresponding ST-type); PFGE type 040-ST2, PFGE 024-ST22, and PFGE 011-ST5, which comprised 21% (17 isolates), 13% (11 isolates), and 11% (9 isolates) (Table 3). These PFGE types included five, five and four subtypes, respectively. In addition, PFGE 031-ST32 included three isolates and each of four other PFGE types included two isolates (PFGE 007, 022, 028, 041). PFGE 040-ST2 and PFGE 011-ST5 were detected in all three hospitals, whereas PFGE 024-ST22 was identified in two hospitals (T and M). Furthermore, two novel single-locus variants, belonging to sequence types of ST5 and ST2, were identified and assigned ST592 and ST593, respectively in the MLST database (www.mlst.net). The eBURST algorithm was used to assess the relationship between predominant sequence types identified in this study with the available database in MLST website (Fig. 2).
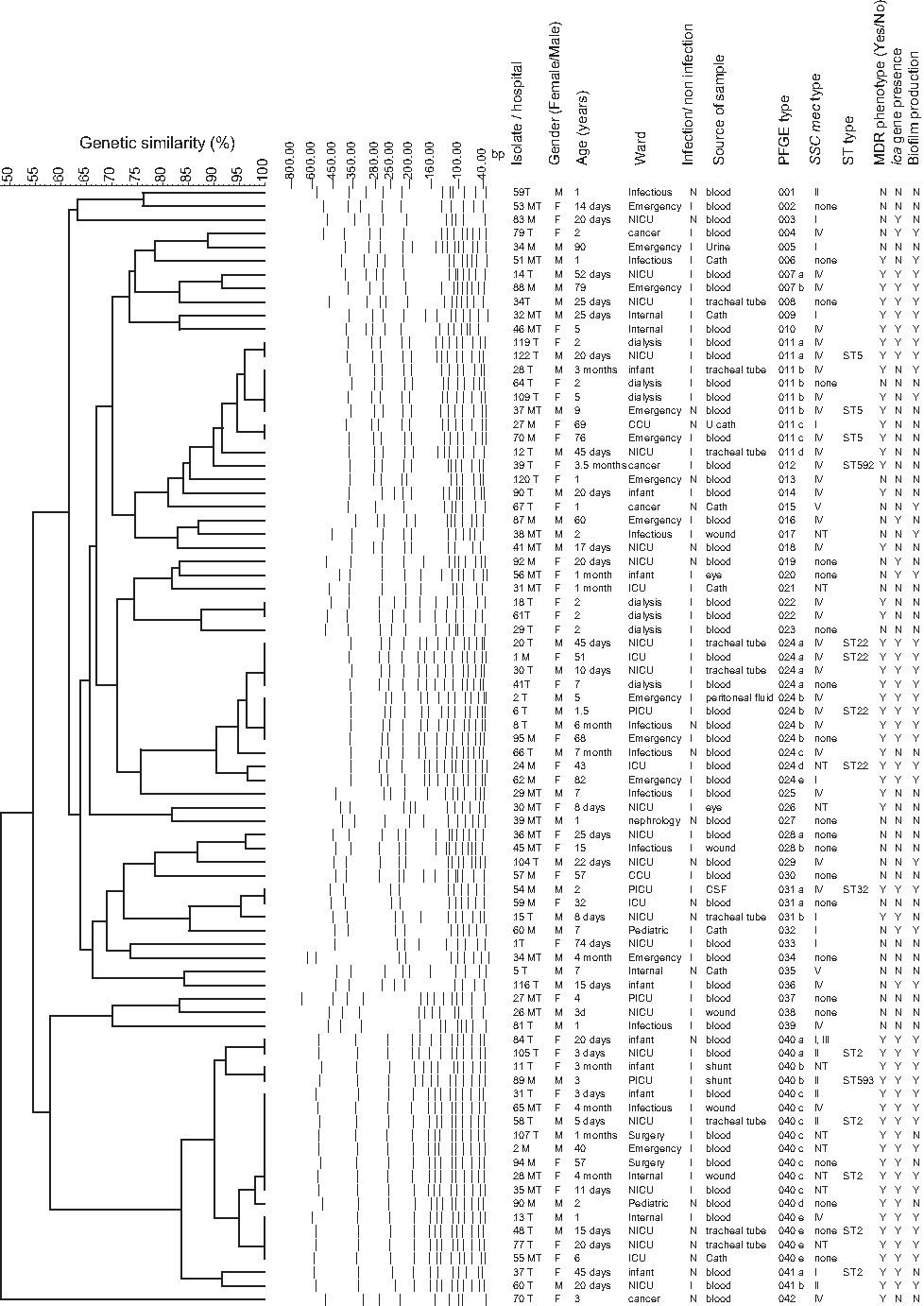
Analysis of the genetic similarity of 82 Staphylococcus epidermidis isolates using PFGE. The horizontal upper bar represents genetic similarity (percent). The dotted lines in the center represent digitalized transformation of the PFGE-DNA pattern. Isolate code/hospital, gender, age, wards, infection/noninfection, source of sample, PFGE type, SCCmec type, ST, MDR phenotype, ica gene presence, and biofilm production are described in the columns to the right. PFGE, pulsed-field gel electrophoresis; ST, sequence type; MDR, multidrug-resistant; SCCmec, staphylococcal cassette chromosome mec.
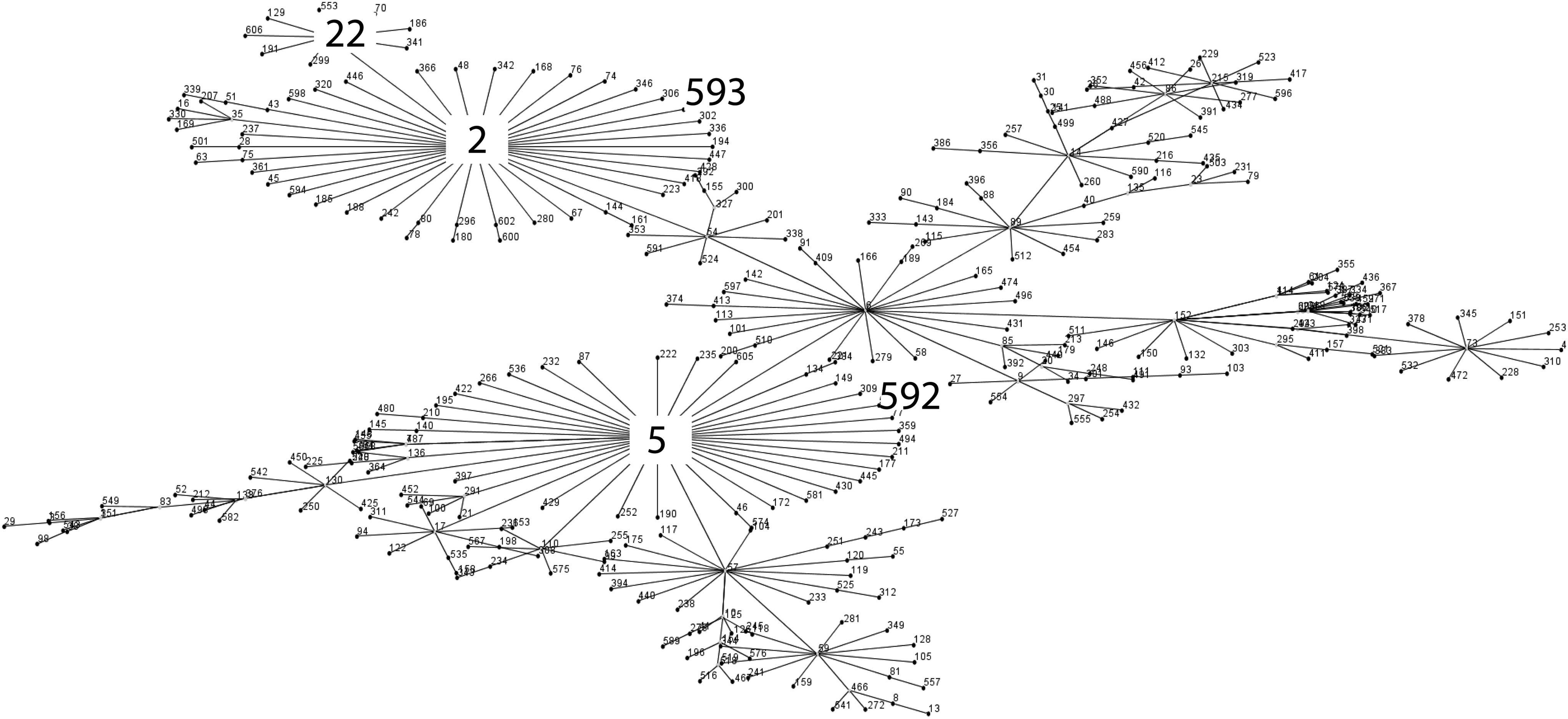
eBURST analysis of S. epidermidis STs observed in this study compared with STs in the multilocus sequence typing database. The numbers in the figure represent the sequence types and ST592 and ST593 represent the novel sequence types found in the present study.
Biofilm formation determined by the microtiter plate assay.
p-value: comparison of predominant and nonclonal PFGE types. Using chi-square test. A p-value of <0.05 is considered statistically significant.
Approximately 54% (44/82) of the isolates harbored the ica operon of which 64% (28/44) were distributed among ST2 and ST22 (Table 3). No significant difference in the carriage of the ica genes were found between infecting and noninfecting groups (p > 0.05).
The SCCmec analysis of 61 mecA-positive isolates revealed that SCCmec type IV was the most prevalent (54%), followed by type I (15%), type II (10%), type V (3%), and type I + III (2%). Ten isolates (16%) were not typable according to SCCmec analysis. PFGE type 044-ST2 isolates were not associated with a specific SCCmec type. Conversely, the majority of isolates in ST22 and ST5 (14/20) carried SCCmec IV (Fig. 1).
The three dominant PFGE types revealed no significant difference in methicillin resistance or MDR phenotype (p > 0.05). However, ST2 isolates were significantly more frequently resistant to fusidic acid (p < 0.001) and gentamicin (p = 0.01) in comparison with those belonging to PFGE 024-ST22 and 011-ST5 (Table 3).
PFGE 011-ST5 proved indistinguishable to the PFGE Co-ST5 previously described in clinical samples from five hospitals in Northern Europe (Umeå, Östersund, Trondheim, Copenhagen, and Växjö) in 2001–2011.12,15 The remaining 41 PFGE types, including the second most common PFGE 024-ST22, showed unique patterns compared to the 1,315 S. epidermidis isolates in the database. However, PFGE 040-ST2 demonstrated 80% similarity to PFGE B-ST2 previously described in MDRSE clinical isolates obtained from eight hospitals in Northern Europe during 2003–2008. 15
Phenotypic characterization of predominant and sporadic PFGE types
The isolates in the three predominant PFGE types showed a significantly increased predisposition to biofilm formation (p = 0.001) and were significantly more commonly associated with ica carriage (p < 0.001) and the MDR phenotype (p < 0.001) compared to nonclustered types. However, no significant association was found in methicillin resistance or clinical significance between these two groups (p = 0.3; p = 1.0) (Table 3).
Discussion
PFGE analysis of 82 clinical S. epidermidis isolates from Iranian hospitals identified three predominant MDRSE clones among isolates with high genetic diversity. The presence of indistinguishable PFGE types in the three hospitals 600 km apart may be explained by the fact that the two examined hospitals in Tehran are large hospitals with patient admissions from all over the country.
The three predominating sequence types belonged to previously well-known healthcare-associated MRSE genotypes. In accordance with other reports,2,4,8,10,13,32,33 all ST2 were MDR and ica positive. Our results are in agreement with a Swedish report that reported 86% MDR among ST2 isolates 4 and two studies from China that reported that all ST2 isolates were ica positive.8,33 Hence, these traits appear to be important factors in ST2 ability to disseminate worldwide. Also ST2 isolates were associated with intensive care units (esp. neonatal ICU), highlighting its adaptability to ward units associated with long period of stay, use of invasive procedures, and high antibiotic pressure, which promote selection of strains and persistence.
The documented interhospital spread of ST22, a single locus variant of ST2, is particularly concerning since linezolid-resistant S. epidermidis (LRSE) isolates belonging to ST22 have been reported in six Greek hospitals. 34 However, LRSE was not detected in this study and whether or not LRSE is present in Iranian hospitals requires further study.
All except one isolate in the three predominant genotypes in the present study were MDR. Hence, acquisition of antibiotic resistance might be an important factor for these genotypes to establish and persist in the hospital environments. This reduces the number of available antimicrobial agents for treatment, increases cost, and the risk of therapy failure. Antimicrobial stewardship intervention and implementation of strict infection control procedures may prevent the establishment and further spread of these MDRSE isolates in healthcare settings.
The existence of PFGE types among distant geographic locations indicate long-distance dissemination of these genotypes. 16 However, the presence of indistinguishable or closely related PFGE types in Iran and in Northern Europe may also reflect an independent evolution at different locations of these genotypes since direct transmission might be less likely to occur. The transmission in and between hospitals worldwide warrants additional studies, including whole-genome sequencing to elucidate the relationship between these strains. 35
SCCmec type IV was the prevailing among ST5 and ST22 isolates. However, the ST2 isolates revealed several different SCCmec types, which is in agreement with Kozitskaya et al. 27 and Ahlstrand et al. 4 This is in contrast to Li et al. 8 who reported SCCmec type III as being the most frequent in ST2 isolates. Recently, SCCmec type IV was identified as the most frequent, and probably the most advantageous in relation to fitness cost, SCCmec type among S. epidermidis isolates of both community and hospital origin. 6
There are some limitations to our study. We classified the isolates according to clinical significance, which is seldom reported in other studies. 4 There are several possible explanations for why no difference in the distribution of genotypes among infecting and noninfecting isolates was detected. First, it can be due to misclassification since there are no generally accepted criteria in this field. Second, the noninfecting isolates may represent the hospital environment flora colonizing the patients before infection. Hence, depending on the timeframe of culture in an individual patient, identical S. epidermidis genotypes may be classified as infecting or noninfecting isolates. Third, the present cohort is small and further studies are warranted to confirm the dynamics and relatedness between infecting and noninfecting isolates.
Lastly, most specimens were obtained from children, in contrast to our compilation of S. epidermidis isolates, which mainly originates from adults. This skewness may hamper the PFGE evaluation since children and especially neonates have a different composition of the skin flora compared to adults. 36 However, this limitation likely had a minor effect on the outcome of the results.
A strength of the present study is that all PFGE analysis, including the compilation of >1,300 S. epidermidis strains, was performed at only one laboratory, which excludes interlaboratory variation that has been reported to affect the evaluation of PFGE gels. 29
In summary, this study provides an overview of the molecular characterization and distribution of clinical isolates of S. epidermidis in Iranian hospitals. We documented the dissemination of MDRSE clones between three Iranian hospitals and a global dissemination of two clonal lineages (ST2 and ST5). Further studies are warranted to explore if interventions such as implementation of antimicrobial stewardship and strict infection control procedures may prevent further spread of these MDRSE isolates in healthcare settings.
Footnotes
Acknowledgments
The authors would like to thank the staff of Medical Microbiology and Clinical Microbiology Departments of Umeå University, Umeå, Sweden.
This study was supported by a grant from the Research and Development Unit, Jämtland County Council, Sweden, and through a regional agreement between Umeå University and the Västerbotten County Council (ALF).
Disclosure Statement
No competing financial or commercial interests exist.