
Abstract
Worldwide increase in carbapenem resistance and transferable carbapenemases are significant challenges in treatment of Pseudomonas aeruginosa infections. In this study, investigation of carbapenemase production in carbapenem-resistant P. aeruginosa isolates recovered from clinical specimens in a tertiary hospital was aimed. A total of 84 carbapenem-resistant P. aeruginosa isolates were examined. “Carbapenem inactivation method” (CIM) was used for phenotypic detection of carbapenemase production. The existence of blaKPC, blaNDM, blaIMP, blaVIM, blaOXA-48, and blaGES genes was investigated by polymerase chain reaction (PCR). Subtypes of the detected genes were identified by sequence analysis. Arbitrarily primed PCR (AP-PCR) was performed to evaluate the clonal relationship among the isolates. The presence of high-risk clones in carbapenemase producers was investigated by Matrix-assisted laser desorption/ionization—time of flight mass spectrometry (MALDI-TOF MS). Three isolates (3.5%) were identified as carbapenemase producers by CIM tests, while PCR tests demonstrated three isolates carrying carbapenemase genes as well. blaVIM gene was found in two isolates and blaGES gene was found in one isolate. Sequence analysis demonstrated that the carbapenemases were VIM-1, VIM-2, and GES-5. AP-PCR yielded high clonal diversity among the isolates. According to MALDI-TOF MS analysis, none of the carbapenemase-producing strains belonged to the high-risk clones. In conclusion, the presence of VIM-1, VIM-2, and GES-5 type carbapenemases in P. aeruginosa isolates was demonstrated for the first time in our hospital, GES-5 being reported for the second time in Turkey. Our results will lead strategies for controlling the spread of carbapenemases and contribute to epidemiological data from Turkey.
Introduction
P
Antimicrobial resistance has become a global problem today. The most recent data from the European antimicrobial resistance surveillance report by European Centre for Disease Prevention and Control (ECDC) have demonstrated an alarming increase in carbapenem resistance especially among gram-negative bacteria within the last decade. 5 Developing strategies to prevent the spread of resistant bacteria can be achieved only by determining antimicrobial resistance profiles of the countries.
Carbapenemase production is one of the most important resistance mechanisms of carbapenem resistance of P. aeruginosa and other gram-negative bacteria. Genes encoding carbapenemases are often located on mobile genetic elements such as plasmids and transpozons that offer them the potential for dissemination, making the spread of carbapenemases among gram-negative bacteria a major challenge for all countries in the world.6,7 Moreover, the carbapenemase-producing isolates are commonly associated with certain multidrug-resistant “high-risk clones,” of which ST235, ST111, and ST175 are the most common, causing outbreaks in hospitals worldwide. 8
Identification of carbapenemases with molecular techniques and regional detection of circulating resistance genes is important for epidemiological surveillance and infection control. In Turkey, the VIM-type metallo-beta lactamases (MBLs) are the most commonly reported carbapenemases in P. aeruginosa in a limited number of studies.9–11 However, more extensive studies are needed to put forward the real rates of resistance genes.
The aim of this study is to determine the occurrence of carbapenemase-encoding genes among carbapenem-resistant P. aeruginosa isolates by both phenotypic and genotypic methods.
Materials and Methods
Bacterial isolates
A collection of 84 P. aeruginosa isolates, resistant to at least one of imipenem or meropenem, obtained from clinical samples sent to Şişli Hamidiye Etfal Training and Research Hospital Clinical Microbiology Laboratory between June 2011 and August 2015 were included in the study. Ninety-three recurring isolates obtained from the same patients were excluded from the study. Bacterial identification, antimicrobial susceptibility testing (AST), phenotypic carbapenemase detection, and polymerase chain reaction (PCR) tests were carried out at the Clinical Microbiology Laboratory of Şişli Hamidiye Etfal Training and Research Hospital, while sequence analysis of the detected carbapenemase-producing strains was performed at İnönü University Faculty of Medicine.
Bacterial identification and AST
For routine identification procedures, automatized systems BD Phoenix™ (Becton Dickinson) or Matrix-assisted laser desorption/ionization—time of flight mass spectrometry (MALDI-TOF MS) (Bruker Daltonics) was used in conjunction with conventional methods. AST was performed by BD Phoenix automatized AST system or Kirby Bauer disk diffusion method, and interpretation was done according to 2011–2015 Clinical and Laboratory Standards Institute (CLSI) guidelines. 12 For isolates found as imipenem and/or meropenem resistant, carbapenem resistance was confirmed by E-test (Oxoid M.I.C. Evaluator; Thermo Fisher Scientific). The isolates were stored at −80°C in trypticase soy broth until molecular tests were performed.
Phenotypic detection of carbapenemase production
To investigate the carbapenemase production of the isolates, “carbapenem inactivation method” (CIM) was used as the phenotypic screening test. To evaluate the efficacy of this newly developed method, negative and positive control strains, which were previously known VIM, IMP, KPC, NDM, OXA-48, and GES producer strains, were tested. After obtaining valid results for all the control strains, the method was applied to the isolates included in the study. CIM was performed as previously described by van der Zwaluw et al. 13 Briefly, a full 10 μl inoculation loop of the tested isolate recovered from blood agar plate was suspended in 400 μl distilled water. Afterward, 10 μg meropenem (Oxoid Ltd.) disk was put into the suspension and incubated at 35°C for 2 hr. A suspension of a carbapenem-susceptible Escherichia coli strain (ATCC 25922) was prepared in saline equal to a McFarland 0.5 turbidity standard and inoculated onto Mueller-Hinton agar (MHA) by covering the entire surface of the plate. The meropenem disk was taken up from the incubated suspension, placed on an MHA plate, and further incubated at 35–37°C. Test results were evaluated at the 6th and 24th hours of incubation. The absence of an inhibition zone was interpreted as the presence of carbapenemase activity due to enzymatic hydrolysis of meropenem during the first incubation step, whereas a clear inhibition zone indicated the absence of carbapenemase activity.
Molecular detection of carbapenemase genes
blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA-48 genes responsible for carbapenemase production were investigated by multiplex PCR as previously described, 14 whereas the blaGES gene was detected by a single primer set. 15 DreamTaq Green PCR Master Mix (Thermo Scientific) was used for PCR tests. Amplification of bacterial DNA was performed by using Gene Amp PCR System 9700 (Applied Biosystems) thermal cycler.
To confirm the enzyme gene types and determine subtypes, nucleotide sequencing was performed by using the Bigdye Terminator V3.1 cycle sequencing kit with an automated DNA sequencing on ABI Prism 310 Genetic Analyzer (Applied Biosystems). The genetic sequence was compared with the database located at NCBI blast server (http://blast.ncbi.nlm.nih.gov).
Phenotypic detection of chromosomal resistance mediated by AmpC hyperproduction plus porin loss
A commercially available combined-disk test (CDT) using imipenem and cloxacillin (AmpC inhibitor) was used to detect the presence of chromosomal resistance (OprD+AmpC), which was likely the most common mechanism in isolates that tested negative for the presence of acquired carbapenemase genes. A 0.5 McFarland inoculum was prepared and inoculated on MHA plates (Becton-Dickinson). Meropenem (10 μg) disk and meropenem disk supplemented with cloxacillin (Bioanalyse) were placed on each plate. After 16 to 18 h of incubation at 35°C to 37°C, the difference between the zone diameters around the meropenem disks with and without cloxacillin was noted. When susceptibility to meropenem was restored in disks containing cloxacillin, it was interpreted that resistance was caused by AmpC hyperproduction coupled with OprD deficiency.16,17
Evaluation of clonal relatedness by AP-PCR analysis
To evaluate the clonal relationship of the isolates, arbitrarily primed PCR (AP-PCR) was performed as described previously. 18 PCR amplification was carried out with the M13 primer. Analysis of AP-PCR band profiles was done using the GelCompar version 6.0 software package (Applied Maths). A dendrogram was constructed by using “Unweighted Pairwise Grouping Mathematical Averaging” (UPGMA) clustering algorithm. Dice coefficient was used to calculate similarities between the pairs of isolates. If the Dice similarity coefficient value was below 90%, isolates were accepted as different genotypes. If the value was between 90% and 100%, isolates were identified as related.
Detection of high-risk clones
The presence of high-risk clones of P. aeruginosa ST111, ST175, ST235, ST253, and ST395 was investigated for the carbapenemase-producing strains using MALDI-TOF MS (Bruker Daltonics) as described by Cabrolier et al. 19 Analysis of the mass spectra was performed using the spectrum view of flexAnalysis 3.4 software (Bruker Daltonics). The presence or absence of the peak biomarkers specific to the high-risk clones was analyzed by visual comparison of the specific spectra.
Results
Bacterial isolates
During the study period, a total of 1,122 P. aeruginosa isolates had been reported and 185 (16.4%) of them were found as carbapenem resistant. Among them, 84 nonduplicate isolates available in stocks were included in the study. Of these isolates, 46 (54.7%) were from female patients, while 38 (45.2%) were from males. Of the patients, 20, 9, 9, 18, and 28 patients were aged between 0–5, 6–15, 16–29, 30–59, and >60, respectively. Most of the isolates were obtained from respiratory specimens (44.0%), followed by urine (20.2%), wound and soft tissue specimens (17.8%), blood (8.3%), sterile body fluid (4.7%), catheters (2.3%), and cerebrospinal fluid (2.3%). Most of the specimens were sent from intensive care units (45%), followed by surgical clinics (23%), internal medicine clinics (18%), and outpatient clinics (14%) of the hospital.
Antimicrobial susceptibility profile
For imipenem-resistant isolates, the range of minimum inhibitory concentration (MIC) value was 8 to ≥32 μg/ml with MIC50 and MIC90 being 16 and ≥32 μg/ml, respectively. Among the carbapenem-resistant P. aeruginosa isolates, susceptibility to amikacin was the highest, while susceptibility to aztreonam was the lowest. Antimicrobial susceptibility profiles of the isolates were shown in Table 1.
S, susceptible; I, intermediate; R, resistant.
CIM tests
CIM tests were primarily applied to VIM, IMP, KPC, NDM, OXA-48, and GES producer positive control strains and a positive reaction was observed with all of them (Fig. 1). Of the 84 isolates tested, three isolates (3.5%) were found to be positive for carbapenemase production by CIM (Fig. 2). The remaining 81 isolates showed clear inhibition zones and were interpreted as CIM negative. All the results could be clearly evaluated after a 6-hr incubation period and there was no significant difference between 6- and 24-hr incubation periods.
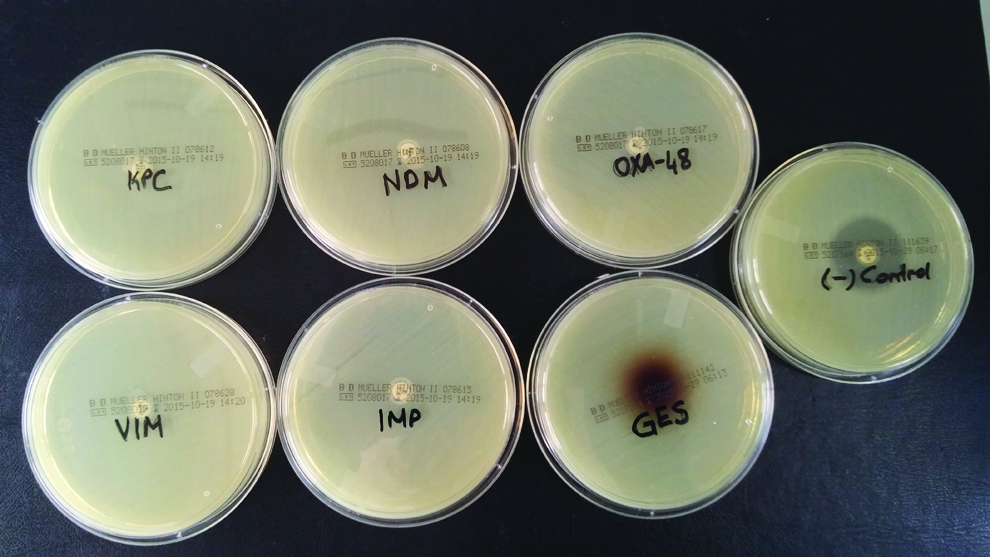
CIM with control strains. Meropenem disks incubated with the suspension containing KPC, NDM, OXA-48, VIM, IMP, and GES producer positive control strains showed no inhibition zone. For the GES-positive strain, a brown discoloration was observed in and around the meropenem disk. A clear inhibition zone was observed for noncarbapenemase producer negative control strain. CIM, carbapenem inactivation method. Color images available online at www.liebertpub.com/mdr

CIM with carbapenemase producing isolates of the study (left) and a negative control strain (right). CIM, Carbapenem inactivation method; Color images available online at www.liebertpub.com/mdr
Molecular detection of carbapenemase genes
PCR detection of carbapenemase genes was positive in three strains (3.5%), two of which were positive for blaVIM and one of which was positive for blaGES. These three isolates were those that were found to be positive by CIM. The other genes (blaIMP, blaKPC, blaNDM, blaOXA-48) were not detected by PCR.
The sequence analysis of the three PCR positive isolates revealed that the carbapenemases were VIM-1, VIM-2, and GES-5. blaVIM-1 carrying P.aeruginosa was obtained from a wound swab of a 9-year-old girl hospitalized in the burn unit of the hospital and showed resistance to all antimicrobials tested except colistin. blaVIM-2 was isolated from a 63-year-old male patient in the intensive care unit of neurosurgery clinic and the isolate was susceptible only to amikacin and colistin. blaGES-5 carrying an isolate was recovered from respiratory tract specimen of an 82-year-old female patient hospitalized in intensive care unit. The isolate was resistant to all antimicrobials except amikacin, cefepime, and colistin.
CDT results
According to the CDT, carbapenem resistance was caused by chromosomal mechanisms (AmpC+OprD) in 43 of the 84 isolates (51.1%). The three isolates identified as carbapenemase producers by the CIM and molecular tests were negative by the CDT.
AP-PCR results
Molecular epidemiological evaluation by AP-PCR yielded no dominant clones among P. aeruginosa isolates. Eighty four P. aeruginosa isolates yielded 73 profiles. The total clustering rate was 23%. Nineteen isolates formed eight clusters (tolerance: 1.0; cut-off: 90%). The largest cluster was genotype I, which included a total of five isolates. The carbapenemase-producing isolates were not in any clusters. The dendrogram of the isolates is shown in Fig. 3.

The dendrogram of AP-PCR profiles generated by UPGMA method based on Dice coefficient. Indistinguishable isolates were shown by a common “numeral.” AP-PCR, arbitrarily primed polymerase chain reaction. UPGMA, Unweighted Pairwise Grouping Mathematical Averaging.
MALDI-TOF MS analysis for the high-risk clones
According to MALDI-TOF MS analysis, there were no high-risk clones, ST111, ST175, ST235, ST253, and ST395, among carbapenemase-producing strains. The GES-producing strain belonged to an international cluster where the high-risk ST235 clone belonged, but yielded peaks characteristic for non-ST235 clones in the cluster. The peak biomarkers for ST111, ST175, ST235, ST253, and ST395 are shown in Fig. 4.
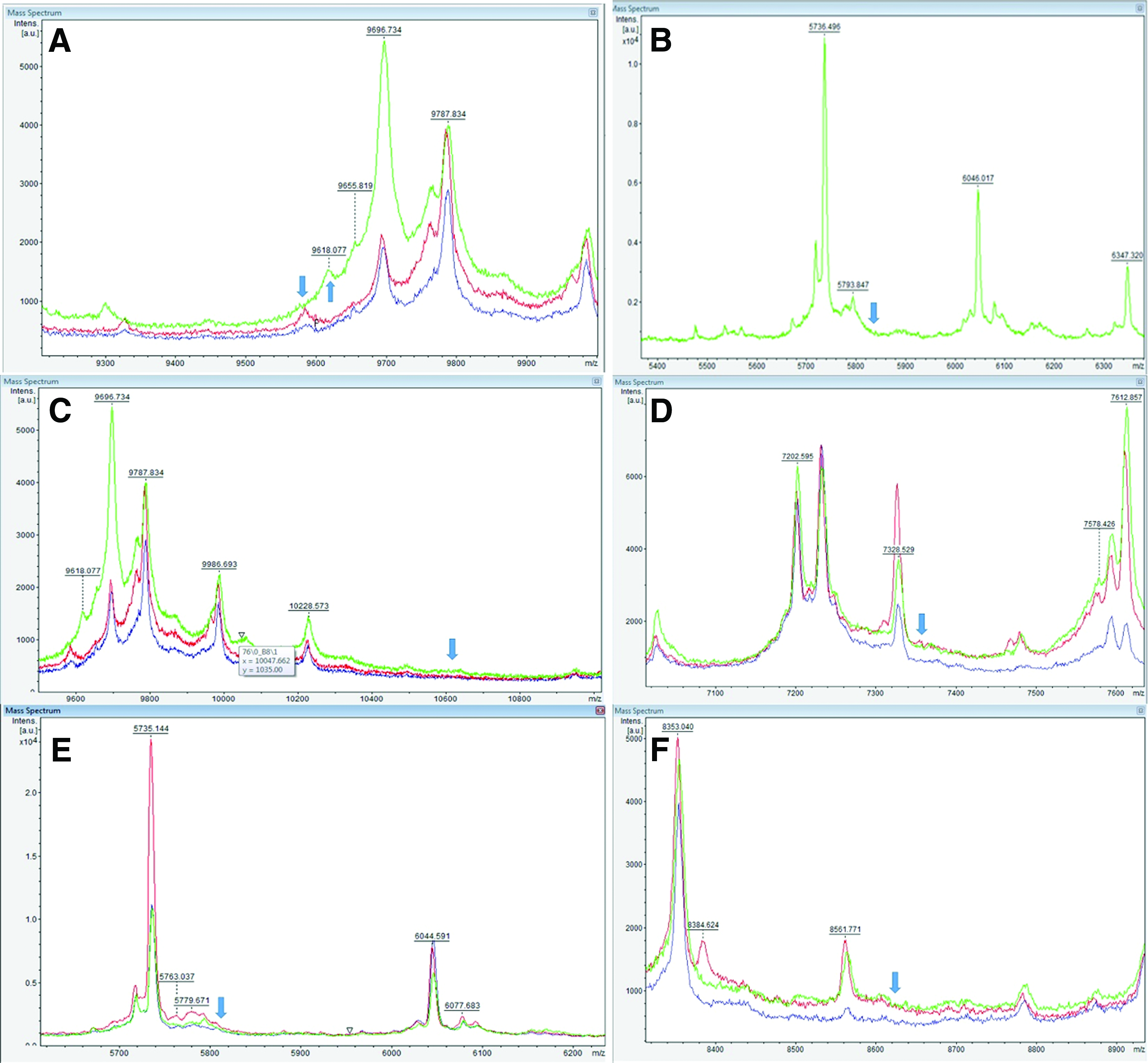
MALDI-TOF MS peak profiles of VIM-1 (red), VIM-2 (blue), and GES-5 (green)-producing P. aeruginosa isolates. The relative intensities of the ions (in a.u., arbitrary units) are shown on the y-axis, and the masses of the ions (in Da) are shown on the x-axis. The m/z value represents mass to charge ratio.
Discussion
Carbapenem resistance in P. aeruginosa is a current and significant concern, particularly because of the limited therapeutic options for this pathogen. Resistance to carbapenems is mostly due to loss of OprD porins, however, carbapenemases encoded by mobile genetic elements, such as serine carbapenemases of molecular classes A, D, and MBLs of molecular class B are important emerging resistance mechanisms in P. aeruginosa.20,21 In this study, of the 84 carbapenem-resistant isolates, 3 isolates (3.5%) were positive for carbapenemase production by phenotypic and genotypic methods. Carbapenem resistance in the remaining 81 isolates may be attributed to other resistance mechanisms, such as porin loss, increased efflux, and AmpC overexpression, however, these mechanisms were not extensively evaluated as this was not the scope of this study. The CDT showed that the most common resistance mechanism was AmpC hyperproduction coupled with OprD deficiency among noncarbapenemase-producing isolates. Although the rate of carbapenemase production in our strain collection is relatively low compared to other mechanisms, detection of these carbapenemases in our area is still important as this brings with it the high potential of horizontal spread.
Over the last decade, different types of carbapenemases among P. aeruginosa strains have been reported with an increasing frequency worldwide. Carbapenemases now account for up to 39% of worldwide and 30.6% of European carbapenem-resistant P. aeruginosa cases.21,22 Although the types of carbapenemase vary among countries, VIM-type and IMP-type MBLs are the most common enzymes with a worldwide distribution. 23 There are limited number of genotype-based studies evaluating carbapenem-resistant P. aeruginosa from Turkey, most of which targeted MBL carbapenemases. The prevalence of carbapenemase producers among carbapenem-resistant P. aeruginosa has ranged from 0% to 48% in different geographic regions in Turkey. In 2010, Küçükbasmacı et al. 24 and in 2013, Mansur et al. 25 and Aksoy 26 reported the lowest prevalence where no MBL genes were identified among all isolates tested. VIM-type carbapenemases were predominantly reported from Turkey with a prevalence varying between 10% and 48% (8–10). Contrary to this, in 2007, Özgümüş et al. 27 reported a 10% MBL prevalence among P. aeruginosa isolates, of which 9% were IMP-1 and 1% was VIM-type MBL. In 2013, Iraz et al. 28 have identified a novel carbapenemase, VIM-38, and published the first report of GES-5-type carbapenemase in P. aeruginosa from Turkey. Recently, Esenkaya Taşbent et al. 29 demonstrated the presence of OXA-type carbapenemases in Pseudomonas strains as being the first report from Turkey.
Although the majority of the detected carbapenemases in P. aeruginosa isolates were Ambler class B MBLs, KPC, GES, and OXA-type serin-beta lactamases are also increasingly reported worldwide. 23 For GES-type beta lactamases, the carbapenemase activity has been demonstrated in certain variants, including GES-2, GES-4, GES-5, GES-6, GES-14, and GES-18.23,30 GES-2, the first described GES-type carbapenemase was identified from a P. aeruginosa isolate during a hospital outbreak in South Africa. 31 Subsequently, GES-5 has been reported from China, South Africa, Brazil, and Turkey.28,32–34 Recently, GES-18, which differs from GES-5 by one amino acid substitution, was identified from a P. aeruginosa isolate from Belgium. 30 To our knowledge, this is the second report of a clinical isolate of P. aeruginosa carrying the blaGES-5 gene in Turkey. In this study, the patient infected with the GES-positive P. aeruginosa died due to hospital-acquired pneumonia caused by this agent. Therefore, its identification is crucial for appropriate and early initiation of treatment and also for implementation of infection prevention measures directed to control their dissemination. Although AP-PCR yielded no dominant clones and the clustering rate was low among the studied population, it should be kept in mind that hospital outbreaks by carbapenem-resistant P. aeruginosa isolates, particularly those producing carbapenemases, are not unlikely.
Detection of high-risk clones of P. aeruginosa in the clinical microbiology laboratory has a major relevance from the aspects of infection control and public health. Although multilocus sequence typing is the gold standard for the analysis of these clones, other cheaper and faster typing techniques are also available. 8 A recent study was able to accurately and quickly detect several P. aeruginosa high-risk clones using the MALDI-TOF MS. 19 In this study, we investigated the presence of the high-risk clones among carbapenemase-producing strains with MALDI-TOF MS, however, none of the isolates yielded peaks specific to the high-risk clones. On the other hand, the absence of the control strains can be regarded as a limitation of investigation of high-risk clones in this study. Another limitation is that the procedure with MALDI-TOF MS has only been validated for French isolates and peak variations may exist.
To improve the detection of carbapenemase producers, various phenotypic tests have been proposed as a first screening step before the use of confirmatory molecular techniques. In 2012, the Carba-NP test provided a great superiority to previous phenotypic methods such as the modified Hodge test and MBL E-test. 35 This method has very high accuracy rates, detects the carbapenemase activity within 2 hr, and is currently being issued in the CLSI and EUCAST guidelines.12,16 However, there are some limiting factors for its use such as its relatively high cost and difficulties for detecting carbapenemase activity in mucoid isolates and isolates with weak carbapenemases such as OXA-48. Recently, a novel test, the CIM, has shown to be very effective for accurate, low cost, and practical detection of carbapenemase activity in gram-negative bacilli. This method can be easily implemented in all laboratories at various levels and does not require special equipment or experienced staff. Although the detection time is longer when compared to Carba-NP test (8 hr vs. 2 hr), the results can be obtained on the same day. In this study, the CIM test and PCR were applied to all isolates included in the study, and a full concordance was found. This study is the first to test GES-producing isolates by CIM. We concluded that the CIM test was a simple and convenient method for screening carbapenem-resistant P. aeruginosa isolates for the presence of carbapenemase enzymes.
Carbapenemase enzymes among P. aeruginosa isolates in Turkey remain poorly investigated. This study reveals new information about carbapenemase enzymes among P. aeruginosa isolates in Turkey by demonstrating the presence of VIM-1, VIM-2, and GES-5 carbapenemases among P. aeruginosa isolates at a tertiary hospital in Istanbul, Turkey. GES-type carbapenemases in P. aeruginosa have been reported rarely in our country and in Europe, and the demonstration of these carbapenemases in this study will contribute to epidemiological data and infection control measures. Considering the emergent characteristic of carbapenemases, continuous surveillance studies are necessary to control the transmission of resistant isolates.
Footnotes
Disclosure Statement
No competing financial interests exist.