
Abstract
The aim of this study was to investigate the molecular features among Klebsiella pneumoniae and Escherichia coli strains showing a resistant/intermediate-resistant phenotype to ertapenem (R/IR-ERT), implicated in colonization/infection in patients of the Hematology and Graft Units of the National Bone Marrow Transplant Center of Tunisia (3-year period, 2011–2014). The major carbapenemase, extended-spectrum beta-lactamase, and plasmidic AmpC beta-lactamase genes were analyzed and characterized by PCR and sequencing. Genetic relatedness was determined by pulsed-field gel electrophoresis (PFGE) using XbaI and multilocus sequencing typing. The blaOXA-48 and blaKPC carbapenemase genes were detected among R/IR-ERT isolates. All R/IR-ERT K. pneumoniae strains (n = 19) had blaOXA-48 gene, and 14/19 strains also harbored the blaCTX-M-15 gene. Eight different PFGE patterns were detected among these K. pneumoniae isolates, and they showed eight different sequences types, ST11 and ST15 being the most prevalent ones. Two out of three R/IR-ERT E. coli isolates carried blaOXA-48 and one coproduced the blaCTX-M-15 gene. One E. coli strain, ascribed to the new sequence type ST5700, harbored the blaKPC-2 gene. E. coli isolates were not clonally related and belonged to different sequence types (ST5700, ST227, and ST58). To our knowledge, this is the first report in Tunisia of either KPC-2 carbapenemase in E. coli or OXA-48 carbapenemase in K. pneumoniae of lineage ST15.
Introduction
C
In Tunisia, in 2011, 41.3% of K. pneumoniae and 10.5% of E. coli isolates were resistant to third-generation cephalosporins, essentially by extended-spectrum beta-lactamase (ESBL) production. These rates were of 31.8% and 17.2% in the National Bone Marrow Transplant Center (NBMTC). 2
In previous studies conducted in Tunisia, the most frequent carbapenemase was OXA-48.3,4 OXA-48 or OXA-204, a new OXA-48 derivative, has been reported in ST11, ST383, ST101, and ST147 K. pneumoniae strains.5,6 Other carbapenemases, such as VIM-4 7 and NDM-1, 8 were rarely identified in K. pneumoniae. IMP-1 and VIM-2 were described in both K. pneumoniae and E. coli isolates.5,9
The aim of this study was to investigate the prevalence and genetic relationship of the ertapenem-resistant/intermediate-resistant (R/IR-ERT) K. pneumoniae and E. coli isolates collected in the National Bone Marrow Transplant Center (NBMTC) of Tunisia during a 3-year period, and to determine the beta-lactamase genes encoding this resistance.
Materials and Methods
Bacterial strains and identification
The NBMTC in Tunis receives patients with immunodeficiency or blood malignancies. In addition to samples analyzed for diagnosis of bacterial infection, systematic surveillance sampling was carried out for all patients upon admission and weekly during hospitalization (throat samples, sputum, urine, and stool), to identify possible colonizing pathogens. Bacterial pathogens and commensal strains were isolated, identified, and antibiotyped. This information is important to guide on an effective first-line antibiotic therapy in neutropenic patients (white blood cells <500), when there is fever or a risk of bacteremia.
All our patients were admitted in single-patient rooms. Contact precautions were systematically implemented, in addition to standard precautions, at admission in the hematology or graft units. When a patient was detected as colonized or infected with multidrug-resistant organism (as ESBL or carbapenemase-producing enterobacteria, among others), contact precautions were continued during all the period of hospitalization.
A retrospective study of carbapenem-resistant K. pneumoniae and E. coli clinical isolates was carried out in the NBMTC from October 2011 to September 2014. During this period, 1,008 patients were hospitalized in our center and the total days of hospitalization were 22,196. When multiple isolates were obtained from a single patient, duplicates were eliminated based on identical patterns of antimicrobial susceptibility, except when duplicates were from different samples and units. Nineteen K. pneumoniae strains isolated from 18 patients were R/IR-ERT (detected by disk diffusion method). These strains were isolated in 2% of all hospital admissions and every 0.86‰ days of hospitalization. Also, three E. coli strains isolated from three patients were R/IR-ERT. These strains were isolated in 0.3% of all hospital admissions and every 0.14‰ days of hospitalization.
Bacterial identification was performed according to the conventional tests and using the API 20E system (bioMérieux, Marcy l'Etoile, France).
Susceptibility testing
Antimicrobial susceptibility was determined by the disk diffusion method according to the French CA-SFM guidelines. 10 K. pneumoniae and E. coli strains, which were R/IR-ERT by disk diffusion test, were included in this study. The minimal inhibitory concentrations (MICs) of ertapenem, imipenem, meropenem, ceftazidime, cefotaxime, amikacin, colistin, and ofloxacin were assessed using the E-test strips (bioMérieux), and breakpoints indicated in CA-SFM guidelines 10 were used (R/IR phenotype: ertapenem: >0.5 μg/ml; imipenem and meropenem: >2 μg/ml). For the quality control in susceptibility testing, E. coli CIP 7624 (ATCC 25922) was used as reference strain for internal quality control, 10 and external quality controls were conducted regularly by the Tunisian Health Ministry.
Detection of resistance genes and integrons
Bacterial DNA extraction was performed using the KIT Instagene Matrix (BIORAD).
All isolates were screened by PCR for the following beta-lactamase genes: blaKPC, blaGES, blaIMI, blaIMP, blaVIM, blaNDM, blaOXA-48, blaSHV, blaTEM, blaCTX-M, and blaOXA-1. Moreover, pAmpC genes (blaMOX, blaCMY, blaLAT, blaBIL, blaDHA, blaACC, blaMIR, blaACT, blaFOX) were also examined by PCR assay using previously described primers. Colistin-resistant strains were screened by PCR for mcr-1 gene (Table 1). PCR products were sequenced for CTX-M-, SHV-, OXA-48-, pAmpC-, and KPC-producing strains.
To completely determine the KPC variant and its environment, KPC-F, KPC-R, and 4,714 primers were used for PCR and sequencing.
Y = C + T; S = G.
For both K. pneumoniae and E. coli isolates, the presence of the intI1, intI2, and intI3 genes, encoding class 1, 2, and 3 integrons, respectively, was determined by PCR as previously described (Table 1).
Molecular typing
Phylogenetic group
The assignment of K. pneumoniae phylogenetic groups was carried out by amplification of the gyrA gene and consequently digestion with TaqI restriction enzyme (Table 2).
The identification of E. coli phylogenetic groups A, B1, B2, and D was performed by PCR as previously described (Table 2).
Pulsed-field gel electrophoresis
For all K. pneumoniae and E. coli strains, pulsed-field gel electrophoresis (PFGE) was performed with a contour-clamped homogeneous electric field CHEF-DR II apparatus from Bio-Rad Laboratories (Richmond, CA), as previously described. 25
Multilocus sequence typing
Multilocus sequence typing (MLST) was carried out for the three E. coli strains and for one representative K. pneumoniae strain of each PFGE pattern, by sequencing the seven housekeeping genes according to previously published strategies (Table 3).
MLST, multilocus sequence typing.
Allele sequences and STs were verified in MLST databases from Pasteur Institute (Paris, France) for K. pneumoniae (http://bigsdb.web.pasteur.fr/klebsiella/klebsiella.html) and E. coli on MLST Warwick website (http://mlst.warwick.ac.uk/mlst).
Results
Bacterial strains
From 2011 to 2014, 315 K. pneumoniae and 411 E. coli isolates were collected in the NBMTC. From this collection, 19 K. pneumoniae and 3 E. coli isolates presented an R/IR-ERT phenotype by disk diffusion, representing 6.03% and 0.73% of isolated K. pneumoniae and E. coli strains, respectively. A total of 14/19 K. pneumoniae and 3/3 E. coli R/IR-ERT strains were isolated from rectal swabs, suggesting an intestinal colonization. Only five R/IR-ERT K. pneumoniae strains, recovered from five different patients, were involved in infections: bacteremia (three strains), urinary tract infection (one strain), and low respiratory infection (one strain). Seventeen K. pneumoniae and two E. coli strains were ESBL producers and represented 17/98 (17.35%) and 2/57 (3.51%) of total ESBL-producing K. pneumoniae and E. coli strains, respectively.
Susceptibility testing
All 19 K. pneumoniae strains with an R/IR-ERT phenotype detected by disk diffusion presented a MIC >0.5 μg/ml for ertapenem, except one strain that showed a MIC of 0.5 μg/ml (in the susceptible category). These strains showed resistance to cephalosporins [cefotaxime (15/19), ceftazidime (15/19), and cefoxitin (10/19)], tobramycin (17/19), gentamicin (15/19), ofloxacin (17/19), tigecycline (12/19), tetracycline (12/19), and trimethoprim–sulfamethoxazole (18/19). Three out of the 19 K. pneumoniae strains were resistant to colistin and had been involved in colonization (4978-b, MIC = 24 μg/ml) or infection (4540 and 3982, MIC = 24 μg/ml) (Table 4). High MIC50 of cefotaxime, ceftazidime, and ofloxacin was observed for the K. pneumoniae strains (>32, 48 and 32 μg/ml, respectively). The 19 K. pneumoniae strains exhibited heterogeneous susceptibilities to carbapenems: ertapenem (MIC50 = 2 μg/ml, MIC90 ≥ 32 μg/ml), imipenem (MIC50 = 0.75 μg/ml, MIC90 = 4 μg/ml), and meropenem (MIC50 = 0.5 μg/ml, MIC90 = 1.5 μg/ml). Four K. pneumoniae strains were resistant to ertapenem (MIC: 1.5–6 μg/ml), but susceptible to third-generation cephalosporins (MIC of CTX: 0.75–1.5 μg/ml).
Same patient.
These strains presented a phenotype R/IR for ertapenem by disk diffusion method, although by MIC determination appeared as susceptible for this antibiotic.
tonB allele was not clear, and two ST could be possible.
H, hematology; G, graft; sl, stool; ur, urine; bl, blood; rp, respiratory; ERT, ertapenem; IMP, imipenem; MEM, meropenem; CTX, cefotaxime; CAZ, ceftazidime; GEN, gentamicin; TOB, tobramycin; AMK, amikacin; TET, tetracycline; OFX, Ofloxacin; SXT, trimethoprim–sulfamethoxazole; COL, colistin; TGC, tigecycline; FOX, cefoxitin; PG, phylogenetic group.
Of the three R/IR-ERT E. coli strains detected by disk diffusion, two strains showed an MIC for ertapenem >0.5 μg/ml (R/IR category), but one showed an MIC of 0.38 μg/ml (susceptible category). Two out of these three strains were resistant to tobramycin, gentamicin, tetracycline, and trimethoprim–sulfamethoxazole. All isolates were susceptible to imipenem, meropenem, amikacin, ofloxacin, colistin, cefoxitin, and tigecycline (Table 4). One E. coli isolate (4133-b) was susceptible to cefotaxime (MIC = 0.19 μg/ml), but resistant to ertapenem (MIC = 32 μg/ml).
Resistance genes
The blaOXA-48, alone or in combination with other genes, was the most prevalent carbapenemase encoding gene detected among K. pneumoniae (19/19) and E. coli strains (2/3) isolated during the studied period (Table 4). The blaKPC-2 gene was detected in only one E. coli strain (ertapenem MIC = 0.38 μg/ml) and sequencing revealed the region immediately downstream surrounding the blaKPC-2 as a transposase, the same one described by Naas et al. 11
All the isolates were negative for genes encoding IMP, GES, IMI, VIM, and NDM carbapenemases. The three colistin-resistant K. pneumoniae strains were negative for mcr-1 gene.
The blaCTX-M-15 gene was found in 14/19 K. pneumoniae and in 1/3 E. coli isolates. Among all the carbapenem-resistant isolates, only one K. pneumoniae strain (2994-a) harbored a pAmpC gene, blaDHA-1, in combination with blaOXA-1 and blaOXA-48 genes.
The four-gene combination, encoding CTX-M-15 + SHV-type + OXA-1 + OXA-48 beta-lactamases, was the most prevalent in K. pneumoniae strains (12/19). Integron analysis showed that all isolates carried class 1 integrons, while class 2 and class 3 integrons were not detected.
Molecular typing
K. pneumoniae strains belonged to phylogenetic group KpI (17/19) or KpII (2/19) (Table 4). The phylogroups identified in E. coli strains were A (1/3 strain) and B1 (2/3 strains) (Table 4).
PFGE identified eight different pulsotypes among K. pneumoniae isolates with a genetic relatedness of 75–100% (Fig. 1). Two major clusters were designated as follows: cluster A (n = 8) and B (n = 4). Six minor clusters were also identified: C (n = 1), D (n = 1), E (n = 1), F (n = 2), G (n = 1), and H (n = 1).
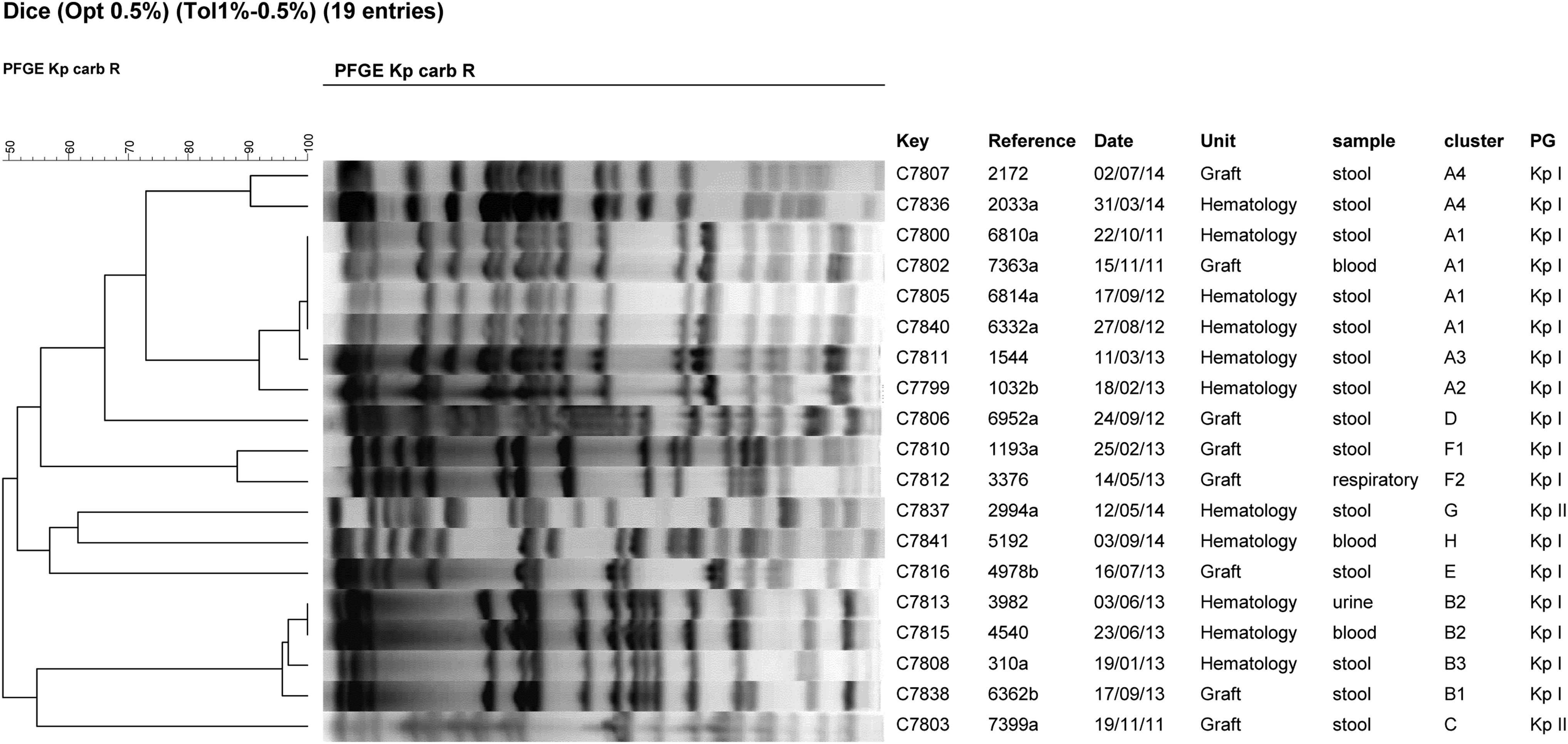
Dendrogram of pulsed-field gel electrophoresis (PFGE) fingerprinting of R/IR-ERT K. pneumoniae isolates (n = 19) after digestion with enzyme XbaI. PFGE, pulsed-field gel electrophoresis; PG, phylogenetic group.
Cluster A was found since October 2011 and persisted until July 2014, in the hematology unit. It was isolated twice in the graft unit, in November 2011 and July 2014. Clone B appeared in January 2013 and persisted until June 2013 in the hematology unit. It was isolated once in the graft unit, in September 2013.
Two out of three colistin-resistant K. pneumoniae strains belonged to cluster B and were isolated from the same unit (hematology) in June 2013 (3,982, 4540an). The remaining strain was of cluster E and was isolated from the graft unit in July 2013 (4978-b).
MLST was performed for one isolate of each of the eight different PFGE patterns and eight different sequence types were detected: ST15 and ST11 were identified in the two major clusters (A and B, respectively). The other STs detected were the following ones: ST196, ST1978, ST14, ST101, ST144, and ST882 (Table 4).
For E. coli isolates, PFGE patterns were different (data not shown). MLST identified three different STs among E. coli isolates: ST227, ST5700, and ST58 (ST155 complex). The ST5700 was identified in the KPC-2-producing strain. It was a new ST with a first described adk allele (503). The ST227 was identified in the CTX-M-15, TEM type, and OXA-48-producing strain (7522-a). The ST58 (ST155 complex) was assigned to the OXA-48, TEM type, and OXA-1-producing E. coli strain (4133-b).
Discussion
In our study, 19 K. pneumoniae and 3 E. coli isolates showed an R/IR-ERT phenotype and carried a carbapenemase-encoding gene. The percentage of R/IR-ERT in K. pneumoniae isolates increased from 3.75% in 2011–2012 to 8.38% in 2013–2014. The increase in combined resistance to more antimicrobial groups and the high frequency of ESBL-producing isolates have led to an increased use of carbapenems, thus favoring the dissemination of carbapenem-resistant bacteria. 28
The majority of the R/IR-ERT isolates were responsible for intestinal colonization (14/19 K. pneumoniae and 3/3 E. coli). Indeed, systematic rectal sampling was carried out in patients upon admission and weekly during the period of hospitalization in the NBMTC. The five remaining K. pneumoniae isolates were involved in different types of infections.
The gene encoding OXA-48 was the most prevalent among the carbapenem-resistant K. pneumoniae (19/19) and E. coli (2/3) isolates. Recently, it has been demonstrated that OXA-48 is the most widespread carbapenemase in North African countries and, in some areas, are facing endemic situations, since carbapenems are the last resort for treating infections due to ESBL-producing Enterobacteriacae. 29
During the period of study, a high prevalence of blaCTX-M-15 was observed among our strains. This is in accordance with another Tunisian study, which reported that all ertapenem-resistant K. pneumoniae harbored the blaOXA-48 gene alone or in combination with CTX-M-15. 30
Regarding the prevalence of plasmid-mediated AmpC-type beta-lactamase genes among our carbapenem-resistant strains, only the blaDHA-1 gene was detected in one cefoxitin-resistant K. pneumoniae isolate, which harbored the blaOXA-48 and blaOXA-1 genes. This blaDHA-1 gene has also been detected in OXA-48-producing K. pneumoniae strains in Morocco. 31
In our study, three K. pneumoniae strains involved in colonization (n = 1) and infections (n = 2) were resistant to colistin. They were recovered between June and July 2013 and the infection cases had well evolved in the hematology unit. The mcr-1 gene was not detected in these colistin-resistant strains. Resistance to colistin has been previously reported among OXA-48-producing isolates, 32 and might be due to the selective pressure exerted by the excessive use of colistin. 33 In our center, colistin was used systematically for total digestive decontamination in transplant patients.
No K. pneumoniae isolates harbored blaKPC gene, but one E. coli isolate was a KPC-2 producer. Sequencing revealed a transposase at the downstream surrounding of the blaKPC-2 gene, suggesting that this gene is located on a transposon. In fact, blaKPC genes have been associated with transposon-related structures. 11 Our strain was susceptible to expanded spectrum cephalosporins, fluoroquinolones, and aminoglycosides (except kanamycin), and showed reduced susceptibility to ertapenem by disk diffusion, but low carbapenem MIC values in the susceptible category (0.38, 0.5, and 0.05 μg/ml for ertapenem, imipenem, and meropenem, respectively). KPC alone not always confer resistance, but reduced susceptibility to carbapenems. The level of resistance to carbapenems is usually higher when ESBL and permeability defects are associated. 1 However, the clinical significance of the presence of a carbapenemase gene in an isolate with a carbapenem MIC in the susceptible range is currently unknown and can lead to therapeutic failure. 34
The phylogroup KpI was the most prevalent among K. pneumoniae isolates followed by KpII. It has been suggested that the higher prevalence of KpI isolates was the consequence of its higher resistance rates. 24 Regarding E. coli isolates, all belonged to A or B1 phylogenetic groups. These phylogroups have traditionally been considered “commensal,” although they have been increasingly recovered in human infections. 35
The MLST analysis showed diversity among the representative R/IR-ERT K. pneumoniae isolates of the eight different PFGE patterns, as the eight tested isolates showed eight different STs: ST11, ST14, ST15, ST101, which are well described clones of OXA-48-producing K. pneumoniae strains, and ST144, ST196, ST882, and ST1978.
ST11, ST14, and ST15 have been associated with multidrug resistance. 36 Moreover, in a recent Spanish study, ST11 and ST15 were described as the most prevalent sequence types among K. pneumoniae carrying the OXA-48 carbapenemase. 37
The ST11, associated in our study to the representative K. pneumoniae isolate of cluster B, carried blaOXA-48, blaSHV-11, blaOXA-1, and blaCTX-M-15 genes. This lineage has been recently reported in Tunisia expressing OXA-48-, CTX-M-15-, and CMY-4-encoding genes. 5 The ST11 is the second most frequent ST in the MLST database (4.28%) (103 of 2,405). 37 Dissemination in both Europe and Asia may indicate that ST11 is a pandemic clone.38,39 It is a single locus variant of ST258, which is a well-known lineage of K. pneumoniae that plays an important role in the global spread of carbapenemases. 40
Our study represents the first report of blaOXA-48-producing K. pneumoniae belonging to ST15 in Tunisia. The occurrence of OXA-48 carbapenemase in a ST15 K. pneumoniae strain was reported in 2012 in Finland. 31 The ST15 is a single-allele variant of ST14. 14 It corresponds to an internationally occurring clone and has been associated with different ESBL and metallo-beta-lactamase genes (blaNDM and blaVIM).41,42 The ST15, associated in our study to the representative K. pneumoniae isolate of cluster A, carried blaSHV-28, blaOXA-48, blaOXA-1, and blaCTX-M15 genes. OXA-48-producing K. pneumoniae isolates belonging to ST15 and coexpressing CTX-M-15, SHV-28, OXA-1, and TEM-1 were also reported from dogs in Germany. 43
ST101 was associated to the representative K. pneumoniae isolate of cluster F, harboring blaOXA-48, blaSHV-28, blaOXA-1, blaCTX-M-15, and blaTEM genes. ST101 was recently reported in Tunisia expressing blaOXA-48, blaSHV-1, blaOXA-1, blaCTX-M-15, and blaTEM-1 genes. 5 This lineage was reported as a predominant OXA-48-producing K. pneumoniae clone in several Mediterranean and European countries. 31
In our study, ST14 belonged to cluster E harboring blaOXA-48, blaSHV-28, blaOXA-1, blaTEM, and blaCTX-M-15 genes. To our knowledge, this is the first report of ST14 K. pneumoniae in Tunisia. This lineage was previously found in OXA-48-producing K. pneumoniae isolates in Turkey, Egypt, and in the USA.31,44
Focusing on carbapenem-resistant E. coli isolates, PFGE showed that they were not related, suggesting that these bacteria could acquire the carbapenemase gene from other bacteria by horizontal transfer of mobile genetic elements. By MLST, three different sequence types were identified among E. coli isolates: ST227, ST5700, and ST58. The ST5700 has been first described in our study and was associated with the production of KPC-2 in an E. coli strain belonging to B1 phylogroup. So, in this study, we report for the first time in Tunisia the emergence of KPC-2 in an E. coli strain. The KPC-2-producing E. coli isolate has been reported previously in other countries (United States, Ireland, etc.) and was associated to the widespread and typically multidrug-resistant ST131 clone. 45
The E. coli strain coproducing OXA-48, CTX-M-15, TEM, and OXA-1 in our study, belonged to phylogroup A and was associated to the uncommon sequence type ST227. In Lebanon, a similar E. coli isolate ascribed to ST227 (phylogroup A) and harboring both blaOXA-48 and blaTEM genes was recently reported. 46
The OXA-48, OXA-1, and TEM-1-producing E. coli strain were of phylogroup B1 and corresponded to the lineage ST58 (ST155 complex). In Europe, OXA-48-producing E. coli isolates were associated to ST38 in France, and to ST131, ST58, and ST83 in Spain.47,48
Conclusion
In conclusion, the R/IR-ERT phenotype was increasing among K. pneumoniae isolates and was emerging among E. coli strains in the NBMTC, with a limited clonal diffusion. This resistance was encoded essentially by blaOXA-48 gene and once by blaKPC-2 in an E. coli strain. This is the first study reporting the emergence of a KPC-producing E. coli isolate in Tunisia, also in a new sequence type ST5700. In addition, OXA-48-producing ST15 K. pneumoniae is described for the first time in Tunisia. For the infection caused by ESBL-producing Enterobacteriaceae that are resistant to cephalosporins and frequently to other classes of antimicrobials, carbapenems remain active and are routinely used for therapy. Emergence of ertapenem-resistant Enterobacteriaceae therefore threatens the viability of this therapeutic approach in our center where ESBL production is frequent among K. pneumoniae strains.
Footnotes
Acknowledgments
F.B.T. has a fellowship from the Research Unit (UR 12ES02), Faculty of Medecine, Ministère de l'Enseignement Supérieur et de la Recherche Scientifique, in Tunisia. C.A.A. has a predoctoral fellowship of the Ministerio de Economía y Competitividad of Spain.
Disclosure Statement
No competing financial interests exist.