
Abstract
Timely detection of carbapenemases by both phenotypic and genotypic methods is essential for developing strategies to control the spread of infections by carbapenem-resistant isolates and related morbidity and mortality. The aim of this study was to compare the performance of a commercial kit, the RAPIDEC® CARBA NP, and an in-house technique, the carbapenem inactivation method (CIM), against a panel of 136 carbapenemase- and noncarbapenemase-producing Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa isolates. RAPIDEC CARBA NP displayed 99% sensitivity and 100% specificity, whereas the sensitivity and specificity were 78% and 100% for the CIM test, respectively. A slight modification of the CIM test, a prolonged incubation time of 4 hours instead of two, increased the sensitivity of the test to 90% by diminishing false negativity particularly for A. baumannii. In conclusion, both tests possess a high performance and are practical for the detection of carbapenemases. Although RAPIDEC CARBA NP is a more rapid and reliable method, the CIM test may represent a useful tool for microbiology laboratories due to its simplicity and availability at any laboratory with low cost.
Introduction
D
Molecular detection of a specific carbapenemase-encoding gene is the gold standard, but this method is of limited practical use for daily application in most of the clinical laboratories. Also, there are some drawbacks with the molecular techniques, such as high cost, requirement of significant expertise, and inability to identify the novel or unknown emerging resistance genes. Thus, a simple, reliable, and low-cost method for screening of carbapenemase producers is necessary for infection control measures.
In 2012, a novel phenotypic method named the Carba NP test was developed by Nordmann et al. for rapid detection of carbapenemase activity.4,5 It is based on the hydrolysis of imipenem molecule by the bacterial lysate, which is detected by changes in pH values using phenol red solution as indicator. This rapid method has very high sensitivity and specificity rates4–6 and is currently being issued in the CLSI and EUCAST guidelines.7,8 A commercially available colorimetric modification of Carba NP test, RAPIDEC® CARBA NP (bioMérieux, France), has now been introduced into many laboratories and provided a practical method for the early detection of carbapenemase production in Enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter baumannii isolates. Recently, van der Zwaluw et al. described the carbapenem inactivation method (CIM), which is a simple carbapenemase detection method that can be performed in any laboratory, since the only basic requirement needed was a 10 μg meropenem susceptibility testing disk. 9 This method has shown to be highly sensitive and specific for detection of any type of carbapenemase activity,9,10 but these results need to be confirmed with more extensive studies. The objective of this study was to evaluate the performance of the two carbapenemase detection assays, the RAPIDEC CARBA NP and CIM for screening carbapenemase-producing Enterobacteriaceae, P. aeruginosa, and A. baumannii isolates.
Materials and Methods
The present study was conducted at Şişli Hamidiye Etfal Training and Research Hospital, Istanbul, Turkey, between December 2015 and January 2016. A panel of 100 Enterobacteriaceae (n = 47), A. baumannii (n = 44), and P. aeruginosa (n = 9) strains with molecularly detected carbapenemases, most of which were published in previous studies,11–13 were assembled from four laboratories located in four different regions of Turkey (Istanbul, Malatya, Rize, and Zonguldak) included in the study. In parallel, a total of 36 isolates, including carbapenem-susceptible isolates of Enterobacteriaceae (n = 11), P. aeruginosa (n = 3), Acinetobacter spp. (n = 6), and A. baumannii (n = 6) plus carbapenem-resistant P. aeruginosa strains (n = 10) with no detected carbapenemase genes were tested as negative controls. The isolates included in this study are demonstrated in Table 1.
CIM test result by 2 hours of meropenem disk incubation with the bacterial suspension.
CIM test result by 4 hours of meropenem disk incubation with the bacterial suspension.
RAPIDEC CARBA NP yielded a negative test result at first, but converted to positive after repeat of the test.
N, not tested; R, strains isolated at the Microbiology Laboratory of Recep Tayyip Erdoğan University Medical Faculty Hospital, Rize, Turkey; M, strains isolated at the Microbiology Laboratory of İnönü University Medical Faculty Hospital, Malatya, Turkey; I, strains isolated at the Microbiology Laboratory of Şişli Hamidiye Etfal Training and Research Hospital, Istanbul, Turkey; Z, strains isolated at the Microbiology Laboratory of Bülent Ecevit University Medical Faculty Hospital, Zonguldak, Turkey; CIM, carbapenem inactivation method.
For routine identification procedures, BD Phoenix™ automated system (Becton Dickinson) was used in conjunction with conventional methods. Antimicrobial Susceptibility Testing was performed by BD Phoenix automated AST system or Kirby–Bauer disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) recommendations 7 and MICs of meropenem for all isolates were determined by E-test (Bioanalyse). All isolates were tested by the CIM and the RAPIDEC CARBA NP for the detection of carbapenemase production. The CIM was performed as previously described 9 on strains cultured on blood agar for 18–24 hours. Briefly, a 10 μg meropenem susceptibility disk (Oxoid Ltd.) was incubated for 2 hours in a suspension of the tested strain. In addition to this, a further 4-hour meropenem incubation with the bacterial suspension was also tested. A 0.5 McFarland suspension of Escherichia coli ATCC 25922 was used to prepare a lawn culture on a Mueller Hinton agar plate (Becton Dickinson). The incubated meropenem disk was removed from the suspension, placed on the Mueller Hinton agar plate and further incubated at 35°C in ambient air. Test results were evaluated at the 6th and 24th hours of incubation. The absence of an inhibition zone was interpreted as the presence of carbapenemase activity due to enzymatic hydrolysis of meropenem, whereas a clear inhibition zone indicated the absence of carbapenemase activity (Fig. 1A).
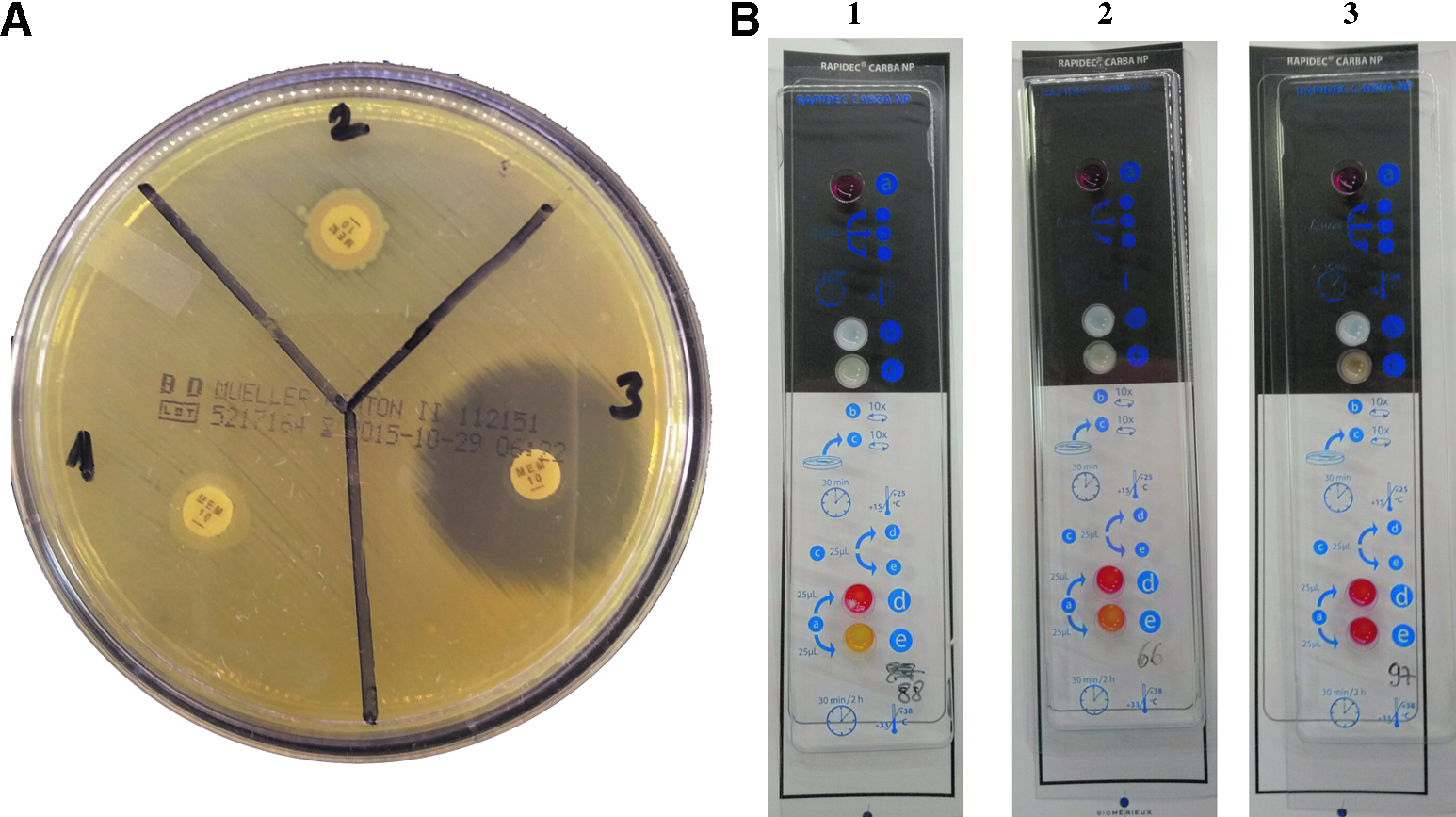
Representative results of the CIM
The RAPIDEC CARBA NP test was performed and interpreted according to the manufacturer's instructions. Any color change from red to yellow or red to orange between control well and test well visible with the naked eye was considered as a positive test result (Fig. 1B).
All the tests were performed by laboratory staff who were blinded to all isolates in the study.
Results and Discussion
The CIM and RAPIDEC CARBA NP results for all the strains are presented in Table 1. The results showed that both methods detected all carbapenemases with 100% sensitivity and 100% specificity for Enterobacteriaceae. After including all isolates (Enterobacteriaceae plus nonfermenting Gram-negative bacilli), the overall sensitivity and specificity were 95% and 100%, respectively, for the RAPIDEC CARBA NP test, 78% and 100% for the CIM with 2-hour initial incubation of meropenem disk, and increased to 90% and 100% for the CIM with 4-hour initial incubation of meropenem disk.
Four GES-22 plus OXA-23 producing A. baumannii isolates initially yielded a negative RAPIDEC CARBA NP test result, but these isolates yielded a positive reaction on repeat testing. These results increased the sensitivity of the test from 95% to 99%.
For the CIM test, all the results could be clearly evaluated after a 6-hour incubation period and there was no significant difference between 6- and 24-hour incubation periods.
For 12 A. baumannii isolates producing GES-22+OXA-23 (n = 2) and OXA-58 (n = 10)-type carbapenemases, false negative results were obtained by CIM tests with 2 hours of meropenem incubation. When the CIM was performed using a prolonged incubation time of 4 hours instead of two, CIM was positive for all these isolates, suggesting low-level carbapenemase activity. For Enterobacteriaceae, no difference was found between 2 and 4 hours of incubation. Thus, we recommend 4 hours initial incubation of the disk for A. baumannii isolates to obtain optimal performance with the CIM.
Two OXA-23-producing A. baumannii isolates exhibited decreased meropenem inhibition zones (18 and 21 mm) when compared with Enterobacteriaceae (E. coli) meropenem susceptibility zone diameter breakpoint of 23 mm. In this study, these isolates were considered as false negative by the CIM test, but it should be kept in mind that a decrease in zone diameter might be a sign of carbapenemase activity and have to be further tested by molecular confirmatory tests.
All negative control strains of A. baumannii yielded negative results for both tests. The naturally produced OXA-51 enzyme of A. baumannii seems not to cause false positive test results and has no effect on CIM test results with prolonged incubation time. A total of 10 carbapenem-resistant noncarbapenemase-producing P. aeruginosa isolates with previously determined 47 kDa membrane protein loss were included in the study and were found negative by both CIM and RAPIDEC CARBA NP tests. Likewise, in a recent study by the authors, in which a total of 84 carbapenem-resistant P. aeruginosa isolates were investigated for the presence of carbapenemases by both CIM and PCR tests, full concordance of CIM and PCR results was reported, including 81 carbapenemase-negative isolates. 14
A subset of carbapenemase-producing isolates (9 Klebsiella pneumoniae, 1 E. coli, and 8 A. baumannii) showed a positive test result with 2-hour meropenem incubation and a negative result with 4-hour meropenem incubation by the CIM test. After analyzing each step of our test procedure, we noticed that discrepancies were due to the fact that we had used decreased amount of bacteria to prepare bacterial suspensions for the second test, that is, with 4 hours incubation, as most of the colonies on the agar plates were used for the first test. When the same amount of bacterial suspension was used for both tests, the results were concordant suggesting the importance of the use of an adequate bacterial inoculum.
OXA-48-type enzymes, which are widespread in Turkey and have also emerged globally, are represented largely (43%) in this study since their detection is often problematic by many phenotypic tests, including Carba NP due to weak carbapenemase activity.14,15 The present study suggests that both tests successfully detected all OXA-48 enzymes with excellent accuracy (100%). On the other hand, the difficulties detecting low-level carbapenemase activity among OXA-58 and OXA-23 producing A. baumannii isolates can be regarded as a limitation of the CIM.
In summary, the RAPIDEC CARBA NP has demonstrated a high performance for rapid, easy, and reliable detection of carbapenemase-producing Gram-negative bacteria. CIM was also very efficient for the detection of carbapenemase-producing Enterobacteriaceae species, but has sensitivity inferior to that of the RAPIDEC CARBA NP for the detection of carbapenemase production in P. aeruginosa and Acinetobacter species. Better results can be obtained with the CIM test when the recommended initial meropenem incubation was doubled (2 hours vs. 4 hours) particularly for A. baumannii isolates. Although the CIM test requires a longer period of time (a minimum of 8 hours for Enterobacteriaceae and 10 hours for A. baumannii vs. 0.5–2 hours for the RAPIDEC CARBA NP) to obtain results, it may be a useful tool for microbiology laboratories as it presents additional advantages, as follows: (i) remarkably reduced cost per isolate (less than €0.5 vs. €8.7 in our institution), taking into account the possibility of the use of the same Petri dish for four to six isolates; (ii) the use of simple equipment such as meropenem disk, Mueller Hinton agar plate, and cotton swabs which are globally available at most laboratories; and (iii) interpretation of results for the CIM is easier compared with the RAPIDEC CARBA NP since the color change might be slight for some isolates with the latter test.
In conclusion, although the RAPIDEC CARBA NP test is a more rapid and sensitive method for detection of carbapenemases, the CIM may be a simple and cost-effective alternative test in the clinical laboratory setting.
Footnotes
Acknowledgment
This work was supported by internal funding of Şişli Hamidiye Etfal Training and Research Hospital (decision date: July 12, 2015).
Disclosure Statement
No competing financial interests exist.