
Abstract
A rapid increase was observed in the incidence of extensively drug-resistant Acinetobacter baumannii (XDR Aba) isolates in a Greek hospital during 2014. To investigate the causes of this rise, the antimicrobial resistance profiles of all carbapenem-resistant (CARB-R) Aba isolates recovered during 2014–2015 were determined. Selected XDR Aba isolates (n = 13) were characterized by molecular methods. XDR Aba (48 isolates) represented 21.4% of the 224 CARB-R Aba recovered during the study period. The 13 selected XDR Aba isolates were positive for the blaOXA-23, the intrinsic blaOXA-51, and the adeB gene of the AdeABC efflux pump, and all belonged to the 3LST ST101, corresponding to the international clone II. Three bloodstream isolates possessed two amino acid substitutions (A138T+A226V) in the deduced amino acid sequences of the pmrB gene, which may be implicated in colistin resistance. This study demonstrates that this clone still evolves by obtaining an ever-increasing arsenal of antibiotic resistance mechanisms. The clinical characteristics of the intensive care unit (ICU) patients with XDR Aba were reviewed retrospectively. Infected ICU patients with XDR Aba displayed higher death rates compared with infected ICU patients susceptible to colistin and tigecycline CARB-R Aba, although there were no statistically significant differences. Conclusively, continuous surveillance and molecular characterization of XDR Aba, combined with strict infection control measures are mandatory for combating nosocomial infections caused by this organism.
Introduction
A
A. baumannii isolates coresistant to carbapenems, colistin, and tigecycline (CARB-R+COL-R+TIG-R) were recovered sporadically during 2011–2013 at the General Hospital of Nea Ionia, “Konstantopouleio-Patission” (Athens, Greece). 8 In the second semester of 2014, a rapid increase was observed in the incidence of CARB-R+COL-R+TIG-R Aba isolates. To investigate the causes of this rise, the antimicrobial resistance profiles of all carbapenem-resistant (CARB-R) Aba isolates recovered during 2014–2015 were determined. Selected isolates were characterized by molecular typing using the 3LST scheme and determination of the carbapenemase gene content. The mechanisms of resistance to tigecycline and colistin were also assessed. The clinical characteristics of the intensive care unit (ICU) patients with CARB-R+COL-R+TIG-R Aba isolates were reviewed retrospectively. We report, in this study, the investigation and management of an outbreak of XDR Aba isolates during 2014–2015.
Materials and Methods
Setting and infection control measures
“Konstantopouleio-Patission,” is a general hospital in Athens, with a potential of 280 beds in total, including a 9-bed medical ICU, internal medicine, surgical, urology, and other wards. Colonization was defined as the isolation of microorganisms from specimens in the absence of infection. To assess colonization on admission, surveillance rectal swab cultures were routinely collected within 24 hrs from all newly admitted patients. Furthermore, urine and bronchial secretion specimens were collected twice per week so as to access acquired colonization, that is colonization that occurred more than 24 hrs after admission to the ICU, without colonization on admission. In some instances, infected patients with XDR Aba were isolated, while a cohorting policy of infected/colonized patients was implemented. From August 2014, an intensive educational program was applied to improve compliance to the infection control measures (hand hygiene, use of personal protective equipment, environmental cleaning, and safe waste management). During the outbreak period, meetings of the Nosocomial Infections Committee with ICU staff of the hospital were held to validate the compliance to infection control measures. The ICU was closed for disinfection on August 2014 and 2015.
Identification and antibiotic susceptibility testing of bacterial isolates
Identification of the isolates to the species level and antibiotic susceptibility testing were performed by the MicroScan® system (Siemens Healthcare, Malvern PA), according to the interpretive criteria of the Clinical and Laboratory Standards Institute (CLSI) 9 and the European Committee on Antimicrobial Susceptibility Testing (EUCAST; www.eucast.org). The minimum inhibitory concentrations (MICs) for imipenem, meropenem, colistin, and tigecycline were additionally determined using the MIC Test Strips (Liofilchem® s.r.l.). There are no CLSI or EUCAST breakpoints for tigecycline to Acinetobacter spp. A common practice is to use the Food and Drug Administration (FDA) breakpoints to Enterobacteriaceae, that is strains with an MIC of ≥4 mg/L were considered to be nonsusceptible. 10
XDR Aba isolates were defined as the nonsusceptible isolates to one or more agent in all, but two or fewer antimicrobial categories. 3 A total of 226 CARB-R Aba isolates were included in the study; the first two CARB-R+COL-R+TIG-R Aba isolates recovered during 2013 and all CARB-R Aba isolates (MICs of imipenem and meropenem ≥8 mg/L) recovered from January 2014 to December 2015. The two XDR Aba isolates (being coresistant to carbapenems, colistin, and tigecycline—CARB-R+COL-R+TIG-R) recovered at the hospital in 20138 were included in the study for comparison with XDR Aba isolates recovered during 2014–2015. Furthermore, molecular identification of XDR Aba isolates was performed by polymerase chain reaction (PCR) detection and sequencing of the blaOXA-51-like gene, as described previously. 2
Molecular identification of XDR Aba isolates
DNA extraction was performed using the QIAcube system (Qiagen, Düsseldof, Germany), according to the instructions of the manufacturer. OXA carbapenemase-encoding genes (blaOXA-23, blaOXA-24, blaOXA-51, and blaOXA-58) and genes associated with tigecycline (adeB, tetX1/tetX2) and colistin (pmrB) resistance were detected by PCR, and the sequences of the PCR products of pmrB from three bloodstream isolates were determined on both DNA strands, as described previously. 8 The 3LST scheme using PCR amplification and sequencing of the ompA-, csuE-, and blaOXA-51-like gene fragments was applied for genotyping of the isolates. 2 Alleles and sequence types were compared on the 3LST scheme website (www.hpa-bioinformatics.org.uk/AB).
Clinical data collection and statistical analysis
The medical records of the ICU patients with XDR Aba were reviewed retrospectively and clinical data were collected. Hospital-acquired infections were defined using established criteria. 11 The gender, age, initial diagnosis, surgical procedures, Acute Physiology and Chronic Health Evaluation (APACHE) II score, infection/colonization status, antibiotic treatment before XDR Aba isolation, and clinical outcome of the ICU patients were assessed. The death rates of ICU patients diagnosed with an infection were compared between two groups of patients admitted to the ICU during the study period: group A consisted of 12 infected patients with XDR Aba (CARB-R+COL-R+TIG-R), whereas group B consisted of 12 infected patients susceptible to colistin and tigecycline CARB-R Aba isolates. Mortality rates of the two groups of patients were compared using the Fisher's exact test, and a p-value of <0.05 was considered to indicate statistical significance. The length of stay (LOS) in the ICU, the APACHE II score, and the age between the two groups of patients were compared using the two-tailed Mann–Whitney test with a critical value of U = 37 at p ≤ 0.05.
Results and Discussion
During 2014–2015, out of 224 CARB-R Aba recovered at the Department of Microbiology, 48 isolates (21.4%) were characterized as XDR, being resistant to penicillins and b-lactamase inhibitors (ampicillin/sulbactam), extended-spectrum cephalosporins (cefotaxime, cefepime, ceftazidime), monobactams (aztreonam), carbapenems (imipenem, meropenem), aminoglycosides (amikacin, gentamicin, tobramycin), fluoroquinolones (ciprofloxacin, levofloxacin), colistin, and tigecycline, and resistant with intermediate susceptibility to tetracyclines (minocycline). Of the 48 XDR Aba isolates, 43 isolates (90%) were also resistant to folate pathway inhibitors (trimethoprim/sulfamethoxazole).
The incidence of XDR Aba isolates has increased rapidly from the first semester (2 out of 35 CARB-R Aba isolates; 5.7%) to the second semester (24 out of 56 CARB-R Aba isolates; 42.8%) of 2014, and thereafter it has decreased gradually to 6.75% (5 out of 74 CARB-R Aba isolates) in the second semester of 2015 (Fig. 1). The rates of coresistant to carbapenems and colistin (CARB-R+COL-R) Aba isolates was 10.3% (23 out of 224 CARB-R Aba isolates) during 2014–2015, whereas an increase was observed from 8.6% (3 out of 35 CARB-R Aba isolates) in the first semester of 2014 to 16.6% (13 out 74 CARB-R Aba isolates) in the second semester of 2015 (Fig. 1). During the study period, coresistant to carbapenems and tigecycline (CARB-R+TIG-R) Aba isolates were also recovered at high frequencies (82 out of 224 CARB-R Aba isolates; 36.6%) in the hospital (Fig. 1). Colistin is widely used due to the high rates of CARB-R Klebsiella pneumoniae, Pseudomonas aeruginosa, and A. baumannii in Greek hospitals. 12 The use of colistin for therapy may have further contributed to the selection of CARB-R Aba isolates that were resistant to both colistin and tigecycline and the rise in the incidence of CARB-R+COL-R Aba isolates.
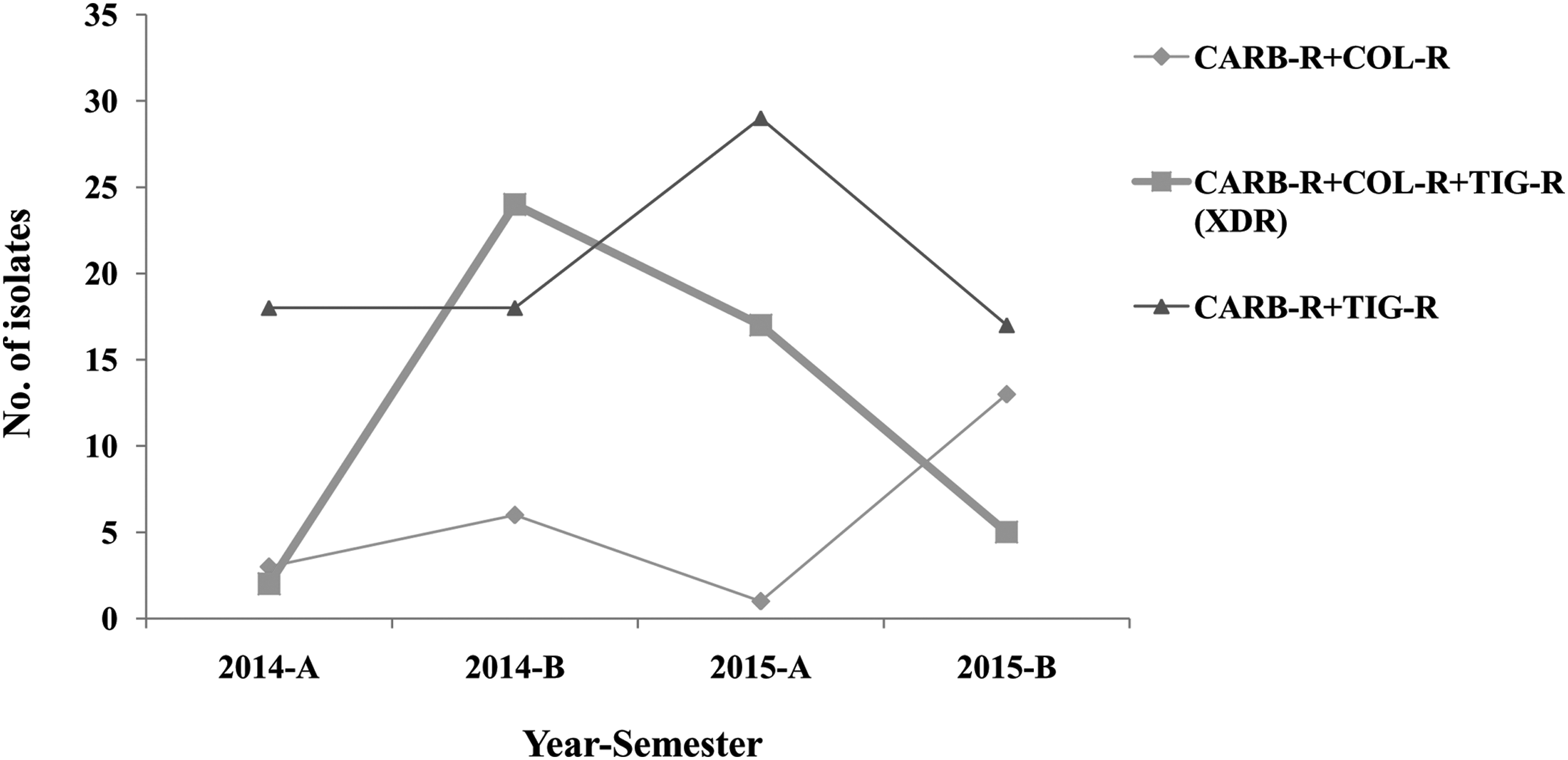
Isolation of XDR Aba per semester (A and B) during 2014–2015. XDR Aba, extensively drug-resistant Acinetobacter baumannii.
The most effective measures reported thus far to reduce the burden of MDR A. baumannii infections in hospitals are cost-effective in the long run, posing a vast burden on hospital resources and personnel. 13 In this study, minor hygiene deviations were recorded during central venous catheter care or suctioning of bronchial secretions. The low hand-hygiene compliance (29%) of healthcare workers improved (46%) after the application of an intensive educational program that may have contributed to the decline in the incidence of XDR Aba isolates from the second semester of 2014 to the second semester of 2015. Upon admission to the ICU, only one ICU patient was found positive for the presence of CARB-R Aba obtained from surveillance rectal swab cultures. A limitation of this study is that surveillance cultures were obtained only from rectal swab cultures of ICU patients and not from other body sites (e.g., the nose, the pharynx, and the skin) and the hands of nursing staff and doctors, so as to identify silent carriers of XDR Aba, or from environmental samples. Moreover, the ICU of the hospital is a small unit with only two isolation rooms and contact precautions were applied in some instances. Decolonization of the patients was not performed.
To investigate whether the rise of the incidence of XDR Aba isolates during the first semester of 2014 was due to the expansion of a single clone or introduction of different clones, XDR Aba (13 isolates) recovered on the onset of the outbreak were further characterized by molecular methods, including the first 2 XDR Aba isolates recovered during 20138 and 11 consecutive XDR Aba isolates from January to September 2014, when the rapid increase in the incidence of XDR Aba was observed. The clinical, microbiological, and molecular characteristics of the 13 XDR Aba isolates are presented in Table 1. Genotyping of the isolates by the 3LST scheme revealed that all belonged to the 3LST ST101 (ompA-csuE-blaOXA-51 like allelic profile: 1-1-1; sequence type Group 1), corresponding to the international clone II. All isolates were positive for the blaOXA-23, the intrinsic blaOXA-51, and the adeB gene of the AdeABC efflux pump. In A. baumannii, resistance to tigecycline is relatively rare, but may develop through overexpression of efflux pumps (such as the AdeABC), especially upon exposure to this agent. 7 Nucleotide sequencing of pmrB from three bloodstream isolates revealed two substitutions (A138T+A226V) in the deduced amino acid sequences, which may be associated with colistin resistance. 8
3LST, trilocus sequence typing; AK, amikacin; AMP/SUL, ampicillin/sulbactam; ATM, aztreonam; bs, bronchial secretions; CAZ, ceftazidime; CIP, ciprofloxacin; COL, colistin; FEP, cefepime; GM, gentamicin; ICU, intensive care unit; IMP, imipenem; IMW, internal medicine ward; MER, meropenem; MICs, minimum inhibitory concentrations; MIN, minocycline; ND, not done; ST, sequence type; SXT, trimethoprim/sulfamethoxazole; TIG, tigecycline; TOB, tobramycin; XDR Aba, extensively drug-resistant Acinetobacter baumannii.
The majority of the 48 XDR Aba isolates were recovered from bronchial secretions (30 isolates; 62.5%) and blood (13 isolates; 27%), and also from other clinical specimens. Overall, the 48 XDR Aba isolates were recovered from 43 patients; 36 (83.7%) patients admitted to the ICU and 7 patients (16.3%) admitted to other wards of the hospital. The clinical characteristics of the 36 XDR Aba ICU cases are presented in Table 2. The mean age of the 36 ICU patients with XDR Aba was 66.8 years (range 20–95 years) and 25 of them (69.5%) were male. The APACHE II scores of the ICU patients with XDR Aba were found in the low to medium category (range 5–39, mean 20.5). ICU patients with XDR Aba have reported prior use of antibiotics, including meropenem (15 patients; 41.6%), colistin (11 patients, 30.5%), and tigecycline (4 patients; 11.1%). The majority of the 36 XDR Aba ICU cases (28 patients; 77.8%) was medical patients (i.e., not subjected to surgical procedures), and 12 of them (33.3%) were diagnosed with an infection.
APACHE, Acute Physiology and Chronic Health Evaluation; VAP, ventilator-associated pneumonia.
During the study period, 37 ICU patients were affected by susceptible to colistin and tigecycline CARB-R Aba isolates and 12 of them (32.43%) were diagnosed with an infection. Infected ICU patients with XDR Aba displayed higher death rates (out of 12 patients, 8 patients expired; 66.67%) than infected ICU patients with susceptible to colistin and tigecycline CARB-R isolates (out of 12 patients, 6 patients expired; 50%), although there were no statistically significant differences (p value of 0.4469). No statistically significant differences were found for the LOS, APACHE II score, and the age between the two groups of patients (U values of 63.5, 67.5, and 51.5, respectively).
The clinically relevant antibiotic resistances in A. baumannii include resistance to broad-spectrum cephalosporins, carbapenems, aminoglycosides, tigecycline, and colistin, which are the last source antibiotics for therapy. In this study, we have described a rapid increase in the incidence of XDR Aba during 2014 due to the dissemination of blaOXA-23-producing Aba of 3LST ST101 in a Greek hospital. The incidence of the XDR Aba isolates has substantially decreased from the second semester of 2014 to the second semester of 2015 (from 42.8% to 6.75%, respectively), and during the first 2 months of 2016 (3 out of 39 CARB-R isolates; 7.7%, data not shown), presumably due to the improved compliance to the implementation of infection control measures. Nonetheless, eradication of the XDR Aba isolates was not feasible.
The dissemination of 3LST ST101 blaOXA-23-producing Aba resistant either to colistin or tigecycline has been reported recently in Greece.8,14 The spread of XDR Aba limits the therapeutic options for nosocomial infections caused by this pathogen. Conclusively, this study demonstrates that the blaOXA-23-producing 3LST ST101 clone still evolves by obtaining an ever-increasing arsenal of antibiotic resistance mechanisms. Thus, continuous surveillance and molecular characterization of XDR A. baumannii combined with strict infection control measures are mandatory for combating nosocomial infections caused by this organism.
Footnotes
Acknowledgments
We thank Ms Rania Kordanouli for excellent technical assistance. Part of the study was presented in the European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), April 9–12, 2016, Amsterdam, the Netherlands.
Disclosure Statement
No competing financial interests exist.