
Abstract
ComPath is a pan-European antimicrobial surveillance program collecting bacterial pathogens from dogs and cats not recently exposed to antimicrobials. We present minimum inhibitory concentration data obtained using Clinical and Laboratory Standards Institute methodology for 616 urinary tract infection (UTI) isolates collected between 2008 and 2010. In both dogs and cats, the most common pathogen was Escherichia coli (59.8% and 46.7%, respectively). Antimicrobial activity against E. coli in dogs and cats was similar with fluoroquinolone and trimethoprim/sulfamethoxazole susceptibility >90%. Ampicillin susceptibility was ∼80%. Staphylococcus intermedius Group isolates from dogs (67/437, 15.3%) had high antimicrobial susceptibility (>90%) toward beta-lactams, fluoroquinolones, and trimethoprim/sulfamethoxazole. Four canine isolates (6%) were oxacillin resistant, and harbored mecA. Proteus mirabilis from dogs (48/437, 11.0%) had high antimicrobial susceptibility (∼90%) to amoxicillin/clavulanic acid, enrofloxacin, and marbofloxacin and slightly lower susceptibility (∼80–85%) to ampicillin and orbifloxacin. Streptococcus canis isolates (35/437, 8.0%) from dogs were all susceptible to ampicillin and amoxicillin/clavulanic acid and >90% susceptible to marbofloxacin. Although resistance was not observed, high intermediate susceptibility was seen for both enrofloxacin (28.6%) and orbifloxacin (85.7%). Overall, antimicrobial in vitro activity appears to be high in UTI pathogens from dogs and cats with low multidrug resistance, although a lack of specific dog and cat breakpoints for important antimicrobials such as cefovecin, cephalexin, and ibafloxacin prevents analysis of susceptibility for these agents.
Introduction
M
The Clinical and Laboratory Standards Institute (CLSI) is the only organization to provide internationally available breakpoints specifically for bacteria isolated from animals. 3 These breakpoints have evolved since first being introduced in 1997. 4 Initially, breakpoints used were those available for human infections, but these can be unsuitable due to differing dosing regimens, pharmacokinetics/pharmacodynamics (PK/PD), and other factors in farm and companion animals compared to humans results in inappropriate therapy in animals. 5 As data have become available, clinical breakpoints have been set for various animal-specific compounds and for several veterinary hosts, including dogs and cats. This process remains far from complete; so analysis for some antimicrobials is animal specific, whereas others still rely on human-derived breakpoints. 3 This is further complicated because human-derived breakpoints can be applied irrespective of the animal host or infection type, whereas host-specific breakpoints are specific not only for the animal host but, often, also for the infection type. In addition, different interpretation criteria are often applied in Europe, for example, the Résapath study 6 uses French national breakpoints, 7 SVARM in Sweden uses a combination of epidemiological cutoff values set by the European Committee on Antimicrobial Susceptibility Testing (EUCAST), and CLSI breakpoints found in the SVARM programs. 8
A further issue is the potential transmission of pathogens to and from humans, including resistant isolates.9–11 It is therefore important to know the extent of resistance in bacteria causing infections in companion animals through surveillance. Various international guidelines have been established to help assist on rational and appropriate antimicrobial use in animals12–14 and these also rely on data from resistance monitoring.
There are few centralized surveillance reports in the literature on the prevalence and antimicrobial susceptibility of pathogens from urinary tract infections (UTIs) in dogs and cats.15–17 This study is part of the CEESA ComPath monitoring program to create a pan-European collection of representative pathogens isolated from confirmed clinical cases of diseased dogs and cats not recently exposed to antimicrobials. Antimicrobial susceptibilities of pathogens recovered from UTI are presented in this study. Organisms were obtained from 10 European Union (EU) countries, which are a geographical selection, representing a major part of the companion animals in the EU. The sampling and isolation were conducted over an approximate 3-year period commencing January 2008 and ending November 2010.
Methodology
Bacterial isolates
Bacterial isolates were exclusively collected from veterinary practices or clinics, from dogs and cats with confirmed clinical UTI, subclinical isolates were not accepted. Isolates recovered from animals known to be treated with antibiotics within 4 weeks before the bacteriological sampling (or if antibiotic treatment history was unknown) were excluded, as were chronically diseased animals. In all cases, only one sample per animal was allowed to help prevent the collection of strains that are epidemiologically related. Whenever possible, pets from the same household or pound, cats from the same breeder, and dogs from the same kennel were not sampled twice. Veterinarians completed and supplied a sampling form for each specimen/isolate tested to confirm compliance with the study protocol. The following 10 countries were selected for sampling: Czech Republic, France, Germany, Hungary, Italy, The Netherlands, Poland, Spain, Sweden, and the United Kingdom.
National laboratories were responsible for recovery and identification of bacterial isolates. However, a complete identification was performed at the central microbiology laboratory, using matrix-assisted laser desorption ionization–time of flight mass spectrometry technology or biochemical confirmatory tests, if isolates were only identified to genus level by the collecting laboratory.
Antimicrobial susceptibility testing
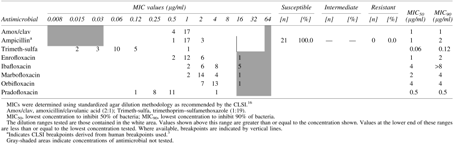
MICs were determined at the central laboratory (LGC, Fordham, United Kingdom; formerly Quotient Bioresearch) using standardized agar dilution methodology as recommended by CLSI. 18 Antimicrobials tested were amoxicillin/clavulanic acid (2:1), ampicillin, cefovecin, cephalexin, oxacillin, trimethoprim–sulfamethoxazole (1:19), enrofloxacin, ibafloxacin, marbofloxacin, orbifloxacin, and pradofloxacin. All experiments included CLSI QC reference strains 18 and MIC data were only accepted if data were within the required reference ranges. 3 The CLSI breakpoints applied are shown in Tables 3–8.
Results of these investigations were used to categorize isolates as susceptible, intermediate, or resistant to antimicrobials according to current MIC breakpoints published by the veterinary standard VET01-S. 3 There are fewer cat breakpoints than dog breakpoints; so where possible, dog breakpoints were used to analyze cat MIC data (ampicillin, enrofloxacin, marbofloxacin, orbifloxacin, and pradofloxacin vs. Escherichia coli). Similarly, cat breakpoints were used for amoxicillin/clavulanic acid with dog isolates of Streptococcus canis. For trimethoprim–sulfamethoxazole and, in part, ampicillin, categorization based on breakpoints derived from human data as recommended in VET01-S was used. 3
Susceptibility was analyzed for isolates where total number was ≥20 isolates to allow calculation of the concentration of each antimicrobial required to inhibit 50% and 90% of the bacterial population (MIC50 and MIC90, respectively). Enterobacteriaceae were categorized as multidrug resistant (MDR) if resistant to three or more from ampicillin, amoxicillin/clavulanic acid, fluoroquinolones (any one of enrofloxacin, marbofloxacin, orbifloxacin or pradofloxacin), or trimethoprim–sulfamethoxazole. For staphylococci, MDR was categorized as resistant to three or more from oxacillin, amoxicillin/clavulanic acid, fluoroquinolones (any one of enrofloxacin, marbofloxacin, orbifloxacin or pradofloxacin), or trimethoprim–sulfamethoxazole. Staphylococci resistant to oxacillin were taken as resistant to all of the beta-lactams tested irrespective of the actual MIC obtained or existence of a clinical breakpoint. 3 Streptococci and Enterococci were categorized as MDR if resistant to three or more from ampicillin, amoxicillin/clavulanic acid, fluoroquinolones (any one of enrofloxacin, marbofloxacin, orbifloxacin, or pradofloxacin), or trimethoprim–sulfamethoxazole. These definitions followed expert guidelines published in 2012. 19
Staphylococcus intermedius Group isolates (n = 6) with oxacillin MICs ≥0.5 μg/ml 3 were screened by PCR for the presence of mecA genes according to a method adapted from Bignardi et al. 20
Results
Bacterial species
UTI isolate numbers categorized by country for dogs and cats are shown in Tables 1 and 2, respectively. Although best efforts were made to collect similar numbers of bacterial isolates from each country, some veterinarians were better able to provide isolates than others with greater numbers obtained from Sweden and Germany than other countries (Tables 1 and 2).
Included S. dysgalactiae (n = 3), S. bovis (n = 2), S. agalactiae (n = 1), S. anginosus (n = 1), S. gallolyticus (n = 1), and S. lutetiensis (n = 1).
CZ, Czech Republic; F, France; D, Germany; H, Hungary; I, Italy; P, Poland; E, Spain; S, Sweden; NL, The Netherlands; UK, United Kingdom.
Included Staphylococcus felis (n = 11), S. intermedius Group (n = 11), S. simulans (n = 4), S. aureus (n = 2), S. schleiferi (n = 2), S. hominis (n = 1), S. lentus (n = 1), and S. warneri (n = 1).
Included Streptococcus canis (n = 5), S. dysgalactiae (n = 1), and S. lutetiensis (n = 1).
For dogs, E. coli was also the most common pathogen (n = 204/437, 46.7%), followed by the S. intermedius Group (n = 67/437, 15.3%), Proteus mirabilis (n = 48/437, 11.0%), and S. canis (n = 35/437, 8.0%). The remaining pathogens made up <4% each (Table 1). For cats, the most common organism was E. coli (n = 107/179) representing 59.8% of all isolates. The next most common pathogens were Staphylococcus spp. (n = 33/179) and Enterococcus faecalis (n = 21/179) at 18.4% and 11.7% of isolates, respectively. The remainder represented <4% each (Table 2).
Antimicrobial susceptibility in dogs
Susceptibility of E. coli to most agents was high at >93%, except for ampicillin, where susceptibility was lower at 79.4% compared to amoxicillin/clavulanic acid at 98.0% susceptibility (Table 3). Five isolates (2.5%) were MDR; two from Germany and one each from Hungary, Poland, and Spain.

The S. intermedius Group isolates were also highly susceptible to those antimicrobials with breakpoints, with all antimicrobials having susceptibility at 91% or above (Table 4). Four canine isolates (6.0%) were considered methicillin resistant (MRSIG), as determined by oxacillin MIC ≥0.5 μg/ml, two from Sweden and one each from Hungary and Spain. All four isolates harbored mecA genes and also were MDR.
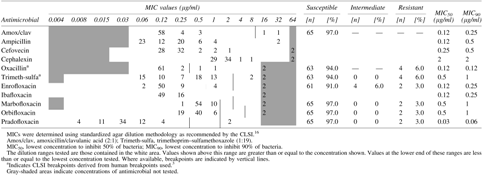
Data for antimicrobials against P. mirabilis from dog UTI are shown in Table 5. Susceptibility to beta-lactam antibiotics was 79.2% to 91.7% and to trimethoprim–sulfamethoxazole was 85.4%, and resistance to fluoroquinolones amounted to 81.3% to 91.7%. Three isolates were MDR (8.3%), one each from Germany, Italy, and Poland.

For S. canis, none of the isolates showed resistance to amoxicillin/clavulanic acid (using cat breakpoints) or ampicillin (using human breakpoints), and none to the fluoroquinolones tested (Table 6). The percentage susceptible and intermediate varied among the fluoroquinolones from 14.3% to 91.4% and from 8.6% to 85.7%, respectively. None was MDR.

Antimicrobial susceptibility in cats
Only amoxicillin/clavulanic acid has cat-specific breakpoints for E. coli and using these breakpoints, all isolates would be considered resistant (Table 7). Ampicillin, on the other hand, does not have cat-specific breakpoints and we have relied on the dog-derived breakpoints (which are higher). Thus susceptibility to ampicillin seems higher (81.3%) than amoxicillin/clavulanic acid.

Trimethoprim–sulfamethoxazole susceptibility in E. coli was the highest (based on human-derived breakpoints) at 95.3% (Table 7). Using dog breakpoints for the cat isolates, fluoroquinolone susceptibility was ∼92%.
Nine feline isolates were MDR (8.4%), four from Sweden, two from Poland, and one each from the Czech Republic, Germany, and Italy.
For E. faecalis, only ampicillin breakpoints are available and these are human derived. All 21 isolates were susceptible (Table 8).
Two feline isolates out of 11 in the S. intermedius Group (18.2%) were considered MRSIG, as determined by oxacillin MIC ≥0.5 μg/ml. Both isolates harbored mecA genes and were also MDR.
MDR isolates
As indicated above, MDR was low in isolates collected from dogs and cats. Data for those rare isolates found to be MDR are shown in Table 9.
AMP, ampicillin; AMC, amoxicillin/clavulanic acid; FOV, cefovecin; LEX, cephalexin; OXA, oxacillin; ENR, enrofloxacin; IBA, ibafloxacin; MAR, marbofloxaicn; ORB, orbafloxacin; PRA, pradofloxacin; T/S, trimethoprim–sulfamethoxazole; (R), MIC indicates resistance.
Discussion
The aim of this study was to increase knowledge on the antimicrobial susceptibility of pathogens associated with UTI in dogs and cats collected between 2008 and 2010. Only a small number of studies have investigated recent UTI pathogens in dogs and cats using centralized surveillance. A combined analysis of dog and cat isolates in Europe between 2002 and 2009 indicated some differences in susceptibility between E. coli and P. mirabilis isolated from UTI. 15 For example, trimethoprim–sulfamethoxazole susceptibility was 53.5% in P. mirabilis and 80.7% in E. coli. 15 We also found lower susceptibility to trimethoprim–sulfamethoxazole in P. mirabilis compared to E. coli in this study, but with less of a difference between the two species. In addition, MDR was higher in P. mirabilis than E. coli.
Our study does not include susceptibility patterns by country, but another study 16 showed that there was higher antimicrobial susceptibility in E. coli dog UTI strains in Sweden (>80% for all antimicrobials tested) than that shown for Europe, combined by Kroemer et al. 15 In our collection, the susceptibility of the Swedish canine (n = 51) and feline (n = 38) E. coli isolates exceeded 86%. The high proportion of isolates obtained from Sweden and Germany may have had an effect on the resistance rates reported in this study. E. coli from cat UTI in Norway 17 showed similar susceptibility as indicated by Kroemer et al. 15 for most antimicrobials, but lower susceptibility to amoxicillin/clavulanate (56% vs. 74.9%). Similarly, the Résapath surveillance network report in 2010 from France showed lower susceptibility to most antibiotics in E. coli from dog and cat UTI than the ComPath data presented in this study, especially to amoxicillin/clavulanic acid (53–58% susceptibility) and fluoroquinolones (75–78% susceptibility). 6 However, care should be taken with these comparisons because CLSI veterinary breakpoints set in 200818 were used by Kroemer et al., 14 whereas EUCAST human breakpoints 21 were used by Lund et al. 17 Furthermore, Résapath determines susceptibility using disk diffusion methodology following French national breakpoints. 7 These results highlight the importance of local antimicrobial resistance surveillance studies and the harmonization of breakpoints for MIC interpretations.
In dog UTI, E. coli was the dominant pathogen (∼50% of the total). Susceptibility to the veterinary fluoroquinolones enrofloxacin, marbofloxacin, orbifloxacin, and pradofloxacin, as well as trimethoprim–sulfamethoxazole, was high (>93%). Ibafloxacin, on the other hand, does not have breakpoints. In dogs, ampicillin and amoxicillin/clavulanate susceptibility was 79.4% and 98.0%, respectively, whereas in cats, ampicillin susceptibility was similar to that seen in dogs (81.3%), but all cat E. coli were deemed resistant to amoxicillin/clavulanic acid due to poorly aligned breakpoints (see below). The SVARM program also investigates E. coli from dog and cat UTI and, despite different breakpoints, the overall resistance observed for the same time period 8 compares well with the ComPath data presented in this study. For example, ampicillin resistance in E. coli was found to be 14–18% in SVARM and 19–20% in ComPath, trimethoprim–sulfamethoxazole resistance was 4–9% in SVARM and 5–7% in ComPath, and enrofloxacin resistance was 7–8% in SVARM and 4–8% in ComPath. BfT-GermVet monitored E. coli susceptibility (dogs and cats combined) in Germany from 2004 to 2006 and ampicillin resistance was found to be 24%, trimethoprim–sulfamethoxazole resistance was 11%, and enrofloxacin resistance was 7%. 22 In a separate study of our collection, 23 all Enterobacteriaceae resistant to cefotaxime/ceftazidime of the present collection were screened for phenotypical extended-spectrum beta-lactamases (ESBLs)/AmpCs, and subsequently genotypically characterized. The study resulted in eight ESBLs (CTX-M-1, CTX-M-14, CTX-M-15, CTX-M-32, TEM-52, SHV-11, and SHV-28) and five AmpCs (all CMY-2) comprising seven E. coli, three P.mirabilis, and three Klebsiella pneumoniae. 23
Within the S. intermedius Group in dogs, oxacillin resistance was low (4/67, 6.0%) in keeping with data from SVARM, which also shows low oxacillin resistance (1–4%) over the same time period, although samples were from skin sources. 8 Other investigators have also found low oxacillin (methicillin) resistance in S. intermedius isolates from dogs and cats, but have suggested an emergent trend of increasing resistance. 24 It will be interesting to observe future data from the ComPath monitoring study. For P. mirabilis from dog UTI, ampicillin susceptibility was similar to that observed with E. coli (79.2%), but susceptibility to amoxicillin/clavulanic acid (91.7%) and fluoroquinolones (81.3–91.7%) was lower than with E. coli. This lower susceptibility to ampicillin and enrofloxacin in Proteus spp. was also observed in combined dog/cat isolates in BfT-GermVet (2004–2006), with 22% resistance to both antimicrobial agents, but no resistance was found to amoxicillin/clavulanic acid. 25
As with dog UTI, E. coli was the most commonly tested pathogen in cat UTI, representing almost 60% of the total; but only amoxicillin/clavulanic acid has CLSI breakpoints specifically for cat UTI. 3 Therefore, for the purpose of this article, dog UTI breakpoints were used for other agents. However, this does create anomalies where applying the cat breakpoint, E. coli shows 0% susceptibility to amoxicillin/clavulanic acid although, based on dog breakpoints or human-derived breakpoints, E. coli shows 81.3% susceptibility to ampicillin. This is an anomaly because the ampicillin dog UTI breakpoint (susceptible only) is high (≤8 μg/ml) compared with the amoxicillin/clavulanic acid susceptible breakpoint for cats (≤0.25 μg/ml). Scientifically, this is illogical because ampicillin and amoxicillin have an essentially identical activity and the addition of clavulanic acid enhances the activity of amoxicillin as indicated by MIC90 of 8 μg/ml for amoxicillin/clavulanic acid and >32 μg/ml for ampicillin. Breakpoints set by the Veterinary Antimicrobial Susceptibility Testing (VAST) Working Group of CLSI rely on data in the public domain or that volunteered by original drug sponsors. Although there is no cat urinary PK/PD data available for amoxicillin/clavulanic acid in the public domain, VAST decided to set UTI breakpoints based on skin and soft tissue infection PK/PD assuming that it was safe to do so as a conservative approach. However, it could be reasonably expected that amoxicillin/clavulanic acid does concentrate in the bladder of cats, so a more appropriate approach could have been to not set any cat UTI breakpoint for amoxicillin/clavulanic acid because this situation is very misleading.
In a similar way, there are no ampicillin breakpoints for S. intermedius Group in dogs, but amoxicillin/clavulanic acid breakpoints are available. We suggest that this is worth further investigation and improvement in future CLSI documents.
Overall, the susceptibility rates for antimicrobials against dog and cat UTI pathogens were high in Europe with the exception of some antimicrobial agents against P. mirabilis dog UTI pathogens. Only a small number of recent publications and national surveillance programs with centralized laboratory testing of UTI pathogens in dogs and cats are available and it is difficult to make comparisons because differing breakpoints and sometimes methodologies were used. This article was designed to exclude animals with chronic disease. It is of interest to note that a recent publication on E. coli from dog UTI found much higher resistance than reported in this study, likely due to the fact that pathogens were from animals with chronic clinical disease submitted to a United States reference laboratory. 26 One other point this study has highlighted is the problem of breakpoint availability for antimicrobials used for canine and feline UTI. The data from this study will provide useful MIC distributions for important UTI pathogens in companion animals to help with the setting of new breakpoints. These MIC data will also provide a base line for tracking of UTI pathogen susceptibility in future ComPath studies and provide information to support the formal setting of epidemiological cutoff values where full clinical breakpoints may not be possible. 27
Footnotes
Acknowledgments
We would like to thank the national coordinators and the national microbiology laboratories involved in the sampling and bacterial isolation procedures. The authors gratefully thank Bayer Animal Health (Stefan Buschmann) for the completion of the mecA gene determinations.
Disclosure Statement
This study was sponsored by Bayer, MSD, Novartis, Vetoquinol, Virbac, and Zoetis. H.M. is a full-time employee of Zoetis. I.M. was an employee of Quotient Bioresearch Ltd. when the susceptibility testing was performed and is currently an employee of IHMA Europe Sàrl, which was paid for the writing of this article. A.d.J. was a full-time employee of Bayer Animal Health during the performance of the study. F.E.G. is a full-time employee of Vetoquinol. U.K. is a full-time employee of Elanco (formerly Novartis Animal Health). C.L. is a full-time employee of Bayer Animal Health. J.T. is a full-time employee of MSD Animal Health. M.Y. is a full-time employee of Virbac.