
Abstract
Multidrug-resistant (MDR) Acinetobacter baumannii has increasingly emerged as an important nosocomial pathogen. The aim of this study was to determine the resistance profiles and genetic diversity in A. baumannii clinical isolates in a tertiary medical center in Malaysia. The minimum inhibitory concentrations of carbapenems (imipenem and meropenem), cephalosporins (ceftazidime and cefepime), and ciprofloxacin were determined by E-test. PCR and sequencing were carried out for the detection of antibiotic resistance genes and mutations. Clonal relatedness among A. baumannii isolates was determined by REP-PCR. Sequence-based typing of OXA-51 and multilocus sequence typing were performed. One hundred twenty-five of 162 (77.2%) A. baumannii isolates had MDR phenotype. From the 162 A. baumannii isolates, 20 strain types were identified and majority of A. baumannii isolates (66%, n = 107) were classified as strain type 1 and were positive for ISAba1-blaOXA-23 and ISAba1-blaADC and had mutations in both gyrA and parC genes at positions, 83 and 80, resulting in serine-to-leucine conversion. REP-PCR analysis showed 129 REP types that generated 31 clones with a 90% similarity cutoff value. OXA-66 variant of the blaOXA-51-like genes was predominantly detected among our A. baumannii clinical isolates belonging to ST195 (found in six clones: 1, 8, 9, 19, 27, and 30) and ST208 (found in clone 21). The study helps us in understanding the genetic diversity of A. baumannii isolates in our setting and confirms that international clone II is the most widely distributed clone in Universiti Kebangsaan Malaysia Medical Centre, Malaysia.
Introduction
A
An intrinsic class D oxacillinase, blaOXA-51-like, is present in A. baumannii that led to be an important genetic marker for identification of this organism. 8 However, the blaOXA-51-like gene was also detected in clinical isolates of Acinetobacter genomic species 13TU. 9 In addition, blaOXA-23, blaOXA-40, and blaOXA-58-like genes are the most common oxacillinases that may be plasmid or chromosomally encoded in carbapenem-resistant A. baumannii. 10 Ambler class C β-lactamase, ampC cephalosporinase, is chromosomally located in A. baumannii. 11 Furthermore, the presence of strong promoter sequences encoded by ISAba1 leads to overproduction of the ampC cephalosporinase and blaOXA-23 gene in cephalosporin- and carbapenem-resistant A. baumannii. 12
Resistance to quinolone is mainly due to chromosomal mutations in the gyrA and parC genes and decreased drug accumulation inside the cell, either due to a decreased permeability of the membrane or an overexpression of efflux pump systems. The mutations result in lower affinity for the binding of quinolone to the enzyme-DNA complex. 13 In A. baumannii, the most prevalent mutations are Ser-83 and Gly-81 in the GyrA protein and Ser-80 and Glu-84 mutations in the ParC protein. 14 Fluoroquinolone-resistant Acinetobacter spp. has emerged rapidly following an increase in the usage of fluoroquinolones (primarily ciprofloxacin). 15
Molecular epidemiological studies are crucial to control the spread of MDR A. baumannii infections. 16 REP-PCR has a high discriminatory power 17,18 and is a suitable option for molecular epidemiological study in most laboratories and hospitals to determine clonal relatedness among local isolates within the hospital. The blaOXA-51-like genes are intrinsic chromosomal β-lactamase genes naturally found in A. baumannii and up to 95 enzyme variants have been identified.19,20 Sequencing of the entire gene was proposed as a blaOXA-51 sequence-based typing (SBT) and it correlated well with the multilocus sequence typing (MLST) scheme proposed by Bartual et al. 21 MLST is a highly informative technique, which puts the isolate in a global context 16 and can directly assign it to a specific clonal complex. Thus, it is regarded as the method of choice for studies related to evolutionary history and long-term phylogenetic studies.
The aims of our study were to understand the mechanisms of antibiotic resistance in A. baumannii and to examine the genetic diversity to understand the local epidemiology of A. baumannii in our setting. Our study enables us to improve therapeutic strategies and infection control measures, which are crucial to reduce dissemination of MDR A. baumannii isolates in the hospital environment.
Materials and Methods
Bacterial isolates and antimicrobial susceptibility testing
One hundred sixty-seven nonrepetitive strains of Acinetobacter species were isolated from patients in various wards at Universiti Kebangsaan Malaysia Medical Centre (UKMMC), Kuala Lumpur, Malaysia, from October 2010 to April 2011. Patients' specimens were sent to the microbiology laboratory and isolates were identified as Acinetobacter spp. by standard microbiology protocols (growth culture characteristics, Gram staining, and biochemical tests). The types of specimens from which bacteria were cultured included soft tissue/wound (44.3%, n = 74), respiratory samples (32.3%, n = 54), urine (10.2%, n = 17), blood (4.2%, n = 7), sterile body fluid (2.4%, n = 4), swabs (4.2%, n = 7), catheter tips (1.8%, n = 3), and bone (0.6%, n = 1). The isolates were further identified as A. baumannii by the amplification of blaOXA-51-like, 16S rRNA, and rpoB gene sequencing, as previously described. 22 Minimum inhibitory concentrations (MICs) of carbapenems (imipenem and meropenem), cephalosporins (ceftazidime and cefepime), and ciprofloxacin for Acinetobacter isolates were determined by the E-test method (BioMérieux SA, France) according to the manufacturer's instructions. The results were interpreted according to the Clinical and Laboratory Standards Institute guidelines. 23 ATCC strains, including Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853, were used as controls. To classify an isolate as MDR, we used the criteria described by Hujer et al. 24
Amplification of antibiotic resistance genes
Resistance genes for carbapenems (blaOXA-23-like, blaOXA-24-like, blaIMP, and blaVIM), cephalosporins (blaADC), and the presence of insertion element (ISAba1) upstream of blaOXA-23-like and blaADC were determined as described previously. 22 The blaOXA-58-like primers used were as described by Hujer et al. 24
Amplification of quinolone resistance-determining regions (QRDRs) was performed with PCR reaction mixtures that consisted of 1× Pfu buffer, 0.8 mM dNTP mixture, 3 mM Mg2+, 10 pmol forward and reverse primers, 2 U Pfu DNA polymerase (Thermo Scientific, Rochester, NY), 100 ng template DNA, and sterile water. The sequences of the primers were described by Hujer et al. 24 The amplification of gyrA and parC genes was performed separately. The PCR amplification for gyrA was as follows: an initial denaturation at 95°C for 3 min; 33 cycles consisting of denaturation at 95°C for 30 sec, annealing at 50°C for 30 sec, and extension at 72°C for 1 min; and a final extension at 72°C for 10 min. The PCR amplification for parC consisted of an initial denaturation at 95°C for 3 min; 30 cycles consisting of denaturation at 95°C for 30 sec, annealing at 55°C for 30 sec, and extension at 72°C for 30 sec; and a final extension at 72°C for 10 min.
The genes were amplified using iCycler thermal cycler (Bio-Rad Laboratories). The PCR bands were detected by gel electrophoresis and purified using the GeneJET Gel Extraction kit according to the manufacturer's instructions (Thermo Scientific).
Detection of mutation in QRDRs
The purified PCR products for gyrA and parC genes were ligated into the pJET 1.2/blunt cloning vector using the Clone JET PCR cloning kit (Thermo Scientific) according to the manufacturer's protocol. The ligation mixture was transformed into E. coli JM109 competent cell that was prepared using the TransformAid Bacterial Transformation kit (Thermo Scientific). The transformed competent cells were plated immediately onto LB agar with 50 μg/ml ampicillin using sterile hockey stick and incubated overnight at 37°C. The plasmids containing genes of interest were extracted and sent for sequencing to FirstBase Laboratories Sdn. Bhd. (Selangor, Malaysia). Sequence comparisons were performed by comparing the sequences of clinical isolates with the wild-type A. baumannii gyrA (GenBank Accession No. X82165) and parC (GenBank Accession No. X95819) using BioEdit software, version 7.2.5.0.
REP-PCR amplification and analysis
The primers used for REP-PCR reaction were REP 1R-1 (5′IIIICGICGICATCIGGC3′) and REP 2-1 (5′ICGICTTATCIGGCCTAC3′). 25 The amplification conditions consisted of an initial denaturation cycle at 95°C for 3 min, followed by 30 cycles of denaturation at 90°C for 30 sec, annealing at 45°C for 1 min, extension at 65°C for 8 min, and final extension at 65°C for 16 min. The reaction mixtures consisted of 1 × reaction buffer, 0.8 mM dNTP mix, 3 mM Mg2+, 10 pmol forward and reverse primers, 1.5 U Taq polymerase (GeNet Bio, Daejeon, Korea), 100 ng template DNA, and sterile water. The PCR product was electrophoresed on 1.5% agarose gel for 1 hr at 80 V in 0.5 × TBE with GelRed dye (Biotium, Inc., San Francisco, CA) and visualized under UV light. The REP-PCR DNA profiles of the A. baumannii were analyzed using Fingerprinting™ II software, version 3.0 (Bio-Rad). Approximately 12 DNA bands with sizes ranging between 0.15 and 3.2 kb were detected, but the most prevalent band sizes were between 0.2 and 3.0 kb. In addition, the bands, which were less than 0.2 kb and more than 3.0 kb, were unclear and the numbers of isolates having these band sizes were small. Therefore, in this study, only DNA bands between 0.2 and 3.0 kb were considered for analysis. Cluster analysis of REP-PCR was based on unweighted pair-group method with arithmetic means (UPGMA). The similarity of REP types was calculated by the band-base dice coefficient (1.3%). A cutoff at 90% similarity was chosen as the threshold for the establishment of clonal relatedness of the isolates. One hundred percent similarity is used to determine REP-PCR types.
Determination of bla OXA-51-like variants and MLST
The blaOXA-51-like gene was amplified and sequenced using the 69A and 69B primers described earlier by Héritier et al. 26 from 31 clones of A. baumannii. MLST was carried out for seven major predominant clones, 1, 8, 9, 19, 21, 27, and 30, as per the Oxford scheme described by Bartual et al. 21
Results
Antimicrobial susceptibility testing
One hundred sixty-two isolates were identified as A. baumannii. The five isolates belonged to Acinetobacter spp. and were also negative for the blaOXA-51-like gene. Further analyses were carried out only for A. baumannii isolates.
The majority of A. baumannii isolates (79%, n = 128) were resistant to carbapenems (imipenem and meropenem). One isolate (0.6%) had intermediate level of resistance to the antibiotics. Both MIC50 and MIC90 values of imipenem and meropenem were >32 mg/L. One hundred twenty-seven (78.4%) isolates were resistant to ceftazidime. Resistance and intermediate to cefepime were observed in 75.3% (n = 122) and 3.7% (n = 6) of the isolates, respectively. Both MIC50 and MIC90 values of cephalosporins were >256 mg/L. One hundred twenty-nine isolates (79.6%) were resistant to ciprofloxacin and the MIC50 and MIC90 values were >32 mg/L.
The majority of A. baumannii isolates (77.2%, n = 125) were multidrug resistant, being resistant to at least three classes of antibiotics, that is, carbapenems (imipenem and meropenem), cephalosporins (cefepime and ceftazidime), and quinolone (ciprofloxacin).
Detection of resistance genes and mutations
Screening the isolates for carbapenem-resistant determinants showed that 82% (n = 133) of the isolates were positive for blaOXA-23-like, whereas 9.9% (n = 16) carried the blaIMP gene. Four strains were positive for both ISAba1-blaOXA-23 and blaIMP, 2 strains were positive for blaOXA-23 and blaIMP, and 10 strains only had the blaIMP gene. None of the isolates carried blaOXA-24-like, blaOXA-58-like, and blaVIM. The blaADC gene encoding for cephalosporin resistance was detected in 88.3% (n = 143) of the A. baumannii isolates. The insertion element, ISAba1, was detected upstream of blaOXA-23-like and blaADC genes in 94.7% (126/133) and 85.3% (122/143) of the isolates, respectively.
Nucleotide sequences of the gyrA and parC genes of our A. baumannii clinical isolates were identical to the sequences in the GenBank database (Accession No. AY642141.1 for gyrA, Accession No. JQ003194.1 for parC). Sequence analysis showed that all ciprofloxacin-susceptible isolates contained no mutation in the QRDRs and all ciprofloxacin-resistant A. baumannii isolates showed point mutations in both gyrA and parC genes. These resistant isolates had the same point mutations with serine-to-leucine conversion at the amino acid positions, 83 and 80, in gyrA and parC, respectively (Fig. 1).
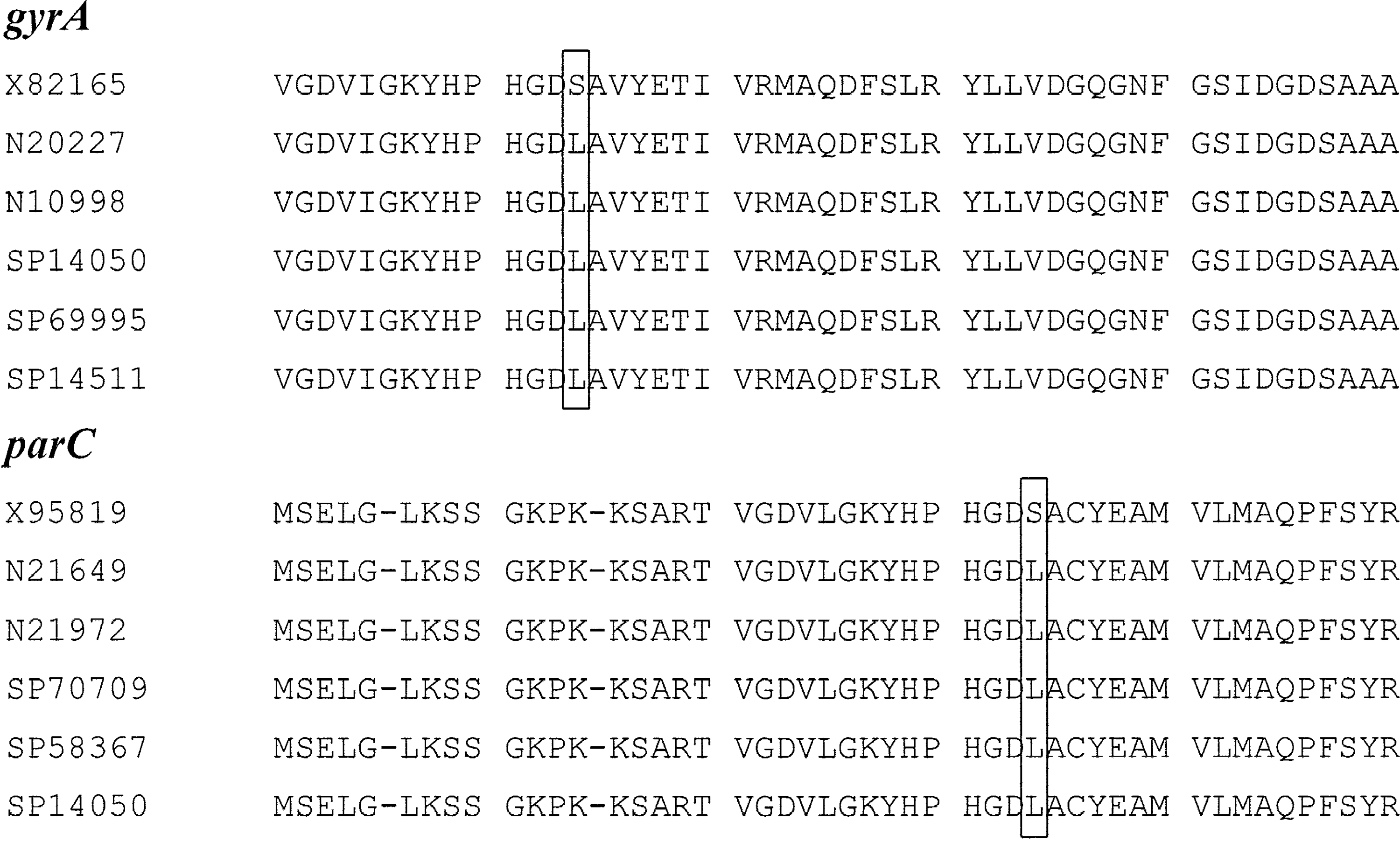
Multiple sequence alignment of QRDR in gyrA and parC for five resistant Acinetobacter baumannii isolates. There is one point mutation at position Ser-83 to Leu-83 and Ser-80 to Leu-80 for gyrA and parC genes, respectively, as shown in the boxes. X82165 and X95819 are wild-type sequences of gyrA and parC genes, respectively. QRDR, quinolone resistance-determining region.
Resistance phenotypes and genotypes
A. baumannii isolates were designated to a specific strain type based on the combination of resistance profile and genotype of the resistance gene. Overall, 20 strain types from a total of 162 isolates of A. baumannii were identified, as described in Table 1. The majority of A. baumannii isolates (66%, n = 107) were classified as strain type 1, followed by strain type 2 (6.2%, n = 10). Other strain types had less than 10 isolates in each group.
MIC value interpretation (CLSI 23 ) for susceptible, intermediate, and resistance. Carbapenem: ≤4, 8, ≥16 μg/ml, cephalosporins: ≤8, 16, ≥32 μg/ml, and ciprofloxacin: ≤1, 2, ≥4 μg/ml.
+ = present, − = absent, nd, not determined (ISAba1 was not determined in the A. baumannii isolates that did not harbor blaOXA-23 or blaADC genes).
CAZ, ceftazidime; CEF, cefepime; CIP, ciprofloxacin; IMI, imipenem; MER, meropenem; MIC, minimum inhibitory concentration.
One hundred twenty-four (76.5%) isolates (strain types 1, 2, 3, 5, and 19) showing MIC of carbapenems >32 mg/L harbored blaOXA-23 and ISAba1 upstream of the gene. Strain types, 10, 14, 16, and 18, which accounted for 7.4% (n = 12) of the isolates, also showed high MIC90 value of >32 mg/L to carbapenems, but we were unable to detect any carbapenem resistance genes. Two isolates (strain types 4 and 9) were susceptible to carbapenems despite having ISAba1 upstream of the blaOXA-23 gene.
A. baumannii having an MIC90 value of >256 mg/L to cephalosporins harbored the ISAba1-blaADC determinant and occurred in 67.9% (n = 110) of the isolates (strain types 1, 3, and 16). Isolates lacked the ISAba1-blaADC gene, but showed high MIC90 values to cephalosporins and were observed in 9.9% (n = 16) (strain types, 5, 10, 14, 18, and 19). In addition, 6.8% (n = 11) of the isolates harbored the ISAba1-blaADC gene, but were susceptible to cephalosporins (strain types 4, 6, and 13).
The presence of point mutations in QRDRs in both gyrA (Ser83Leu) and parC (Ser80Leu) genes was identified in isolates showing the ciprofloxacin MIC90 values of >32 mg/L.
REP-PCR fingerprinting analysis
REP-PCR fingerprints of the 162 A. baumannii and 5 non-A. baumannii isolates were established (Fig. 1). One hundred twenty-nine REP-PCR DNA profiles were defined for all the isolates, including Acinetobacter spp. A. baumannii ATCC 19606 was used as reference, which exhibited a unique REP-PCR pattern (REP96). At 90% similarity cutoff, 112 A. baumannii isolates were designated into specific clones (clones 1–31) and 50 A. baumannii isolates had unique REP-PCR profiles (singleton). Majority of the isolates with strain type 1 (84.1%; 90/107) were closely related isolates and were grouped into specific clones. The rest of the isolates with strain type 1 (15.9%; 17/107) had unique REP-PCR profiles. Six of 7 (85.7%) and 3 of 4 (75%) of clone 1 and clone 2 strains, respectively, were isolated from patients in the intensive care unit (ICU). Clone 8 represented the largest clone identified in this study, consisting of 15 A. baumannii isolates that were isolated from various wards; 33.3% (n = 5) from ICU, 26.4% (n = 4) from Medical, 13.3% (n = 2) from Surgery, and 26.7% (n = 4) from Orthopedic.
OXA-51 SBT
The blaOXA-51-like SBT was performed on 31 representative clones/isolate as defined by the REP-PCR pattern. Sequencing of alleles identified the presence of blaOXA-66 alleles in 90.3% (28/31) of these isolates belonging to specific clone groups. The variants, blaOXA-64 and blaOXA-67, were also identified in representative isolates belonging to clones 23 and 24 (Fig. 2), but belonged to carbapenem-susceptible strains with strain type 13 and type 12, respectively (Table 1).

Dendrogram generated from REP-PCR fingerprints representing the Acinetobacter spp. in UKM Medical Center which includes 162 A. baumannii and 5 non-A. baumannii as indicated with *. Black box indicates the isolates, which were positive for both ISAba1-blaOXA-23 and blaIMP.
Multilocus sequence typing
MLST using the Oxford scheme was performed on seven selected A. baumannii isolates representing the major REP-PCR clones (clones 1, 8, 9, 19, 21, 27, and 30) (Fig. 2) and two sequence types (STs) were identified. ST195 was the most predominant ST among the clonal population of A. baumannii that occurred in six different clones (1, 8, 9, 19, 27, 30), whereas ST208 belonged to isolate SP21856, which was unique to clone 21.
Discussion
The present study shows that majority of the A. baumannii isolates in our hospital were highly resistant to carbapenems (imipenem and meropenem), cephalosporins (ceftazidime and cefepime), and ciprofloxacin and more than 70% of the isolates were multidrug resistant (MDR). Our previous report showed that all A. baumannii isolates were susceptible to polymyxin B and 7.4% were resistant to tigecycline. 27 A study conducted from 2006 to 2009 showed that carbapenem resistance rates were as high as 96–98% in the University Malaya Medical Centre facility (UMMC) Kuala Lumpur, Malaysia. 28 However, in a different study 29 conducted in UMMC in 2008–2009, it was observed that the carbapenem resistance rates were as low as 55% (n = 55). Furthermore, it was found in the same study that 75% (n = 15) of the environmental isolates collected from the hospital environment were carbapenem resistant. 29 The resistance rates of MDR A. baumannii observed in the present study were 77.2% and, for carbapenems, it was 79% (n = 128). These are similar to the carbapenem resistance rates (77.8% for meropenem and 74.1% for imipenem) observed in Hospital Sultanah Nur Zahirah (HSNZ), a tertiary hospital in Terengganu, Malaysia, in 2011. 30 The same study also found that 76% (41/54) of the isolates also possessed the blaOXA-23 determinant, which is marginally less than what we observed in our study.
IMP-4 has been discovered on plasmids and integrons in Acinetobacter calcoaceticus strains isolated from UMMC from 2003 to 2004. 31 Subsequently, the first report of IMP-4 variant from a P. aeruginosa strain isolated from 2005 to 2006 in UMMC, Malaysia, was reported, which also mentioned other metallo-β-lactamases such as IMP-7, VIM-2, and VIM-11. 32 In a study from Singapore, 33 blaIMP-4 coexisted with blaOXA-58, but this was not observed in our study and all our isolates were blaOXA-58 negative. It is interesting to note that IMP metallo-β-lactamase was present in 9.9% (n = 16) and four strains, which were positive for ISAba1-blaOXA-23, belonged to clones, 8, 16, 25, and 31 (one strain to each clone), as shown in Fig. 2. The rest of the 12 blaIMP-positive A. baumannii isolates were singleton. Since interplay of plasmid-associated integrons does play a role in spread of carbapenem resistance, it can be concluded that clone possessing the IMP-4 variant could be responsible for the spread of this determinant from UMMC to UKMMC as both the medical centers are at a distance of just 11 km. MDR A. baumannii infections occurring in immunocompromised patients can result in increased mortality and hospitalization. Routine use of the same antimicrobial agents for treatment might have contributed to the selective pressure for development of resistance. The transmission of MDR A. baumannii through hands of healthcare workers as well as from hospital facilities might contribute to the wide dissemination of MDR A. baumannii in the hospital.34,35 The emergence of antibiotic-resistant Acinetobacter spp. could also be due to the introduction of resistant isolates from external sources, such as transfer of patients from other hospitals or wards within a hospital. 36
The molecular mechanisms responsible for resistance to carbapenems (imipenem and meropenem) and cephalosporins (ceftazidime and cefepime) in our clinical isolates were due to the presence of blaOXA-23 and blaADC genes under the influence of strong promoter provided by ISAba1 upstream of the genes. These resistance determinants have been reported in many studies.12,37–41 We found that up to 10% of the isolates did not harbor ISAba1-blaOXA-23 and ISAba1-blaADC, but were highly resistant to carbapenems and cephalosporins, suggesting that other resistance mechanisms might be involved such as the presence of other β-lactamases, changes in permeability, increase in efflux, and modification of affinity of penicillin-binding proteins.5,42–44 The presence of other insertion sequence (IS) elements such as ISAba125 has been reported to be involved in overexpression of the blaADC greater than the ISAba1 and leads to cephalosporin resistance, 45 but this was not observed in our study. Some of the strains did have ISAba1 upstream of the blaOXA-23 and/or blaADC genes, but exhibited low levels of resistance to carbapenems and cephalosporins and this warrants further investigation. This might be due to the translational frameshift of ISAba1, resulting in gene downregulation. 46
High levels of ciprofloxacin resistance in our isolates were due to mutations in both gyrA and parC genes at positions, 83 and 80, resulting in serine-to-leucine conversion. The high-level resistance to ciprofloxacin when two mutations exist in the gyrA and parC genes has also been described previously for ciprofloxacin-resistant P. aeruginosa, Salmonella spp., E. coli, and Klebsiella pneumoniae.47–50
Clonal relatedness and genetic profiles of A. baumannii isolates were determined using an in-house REP-PCR method, which is rapid, cost-effective, and reproducible. This has been shown to be very useful for the identification of clonal relationship among A. baumannii isolates. The combination of the REP-PCR method with other epidemiological typing tools such as blaOXA-51 sequence typing and MLST provides data for understanding the dynamics of the circulating strains. In the present study, the REP-PCR technique revealed considerable diversity between isolates, generating a dendogram with 31 clones. A considerably high number of unique pattern strains indicated that they were derived from distinct strains, which originated from different patients and different types of clinical samples. This also shows that A. baumannii genomes are heterogeneous regarding the gene contents and possession of a series of unique genes.1,51,52
Isolates with strain type 1 harboring OXA-66 variant belonging to international clone II were found to be predominant in almost all clones in our study and were distributed in various wards (ICU, Medical, Surgery, and Orthopedic). This suggests an extensive interhospital dissemination and thus these stains could be considered as an endemic strain. A. baumannii harboring OXA-66 variant has been reported from many studies from various regions.21,53,54 Sporadic variants of the OXA-51 gene, that is, OXA-64, OXA-67, and OXA-70, were also identified among our A. baumannii isolates and all of them did not harbor the acquired OXA-23 gene. These OXA-51 variants formed different clusters from OXA-66 lineage. 19 OXA-64 has been identified in the A. baumannii isolates from Greece (11.11%; 65/585). 55 Seven of 116 (6%) of the isolates from the Middle East (Syrian and Lebanese patients) also possessed the OXA-64 gene. 54 One isolate of Singaporean origin has been identified harboring the OXA-64 gene. 56 The blaOXA-64 belongs to the worldwide/international clone 7 lineage and this variant is closely related to OXA-71, which is now commonly found in the Middle East. Hence, strains possessing OXA-64 variant are often referred to as Middle Eastern clones. 57 The extensive movement of people from the Middle East to Asian countries for education, leisure, medical reasons, and tourism might serve as a way of transmission of these A. baumannii strains.
The UKMMC is 11 km away from UMMC, whereas HSNZ is at a distance of 450 km, and although no conclusions can be drawn with regard to spread of clones within the country, it can still be concluded that the prevalence of carbapenem-resistant A. baumannii in hospitals is as high as 77%. Hence, there should be more emphasis on implementing suitable and effective surveillance and control strategies to mitigate against any outbreaks occurring in the hospital environment. The major clones belonging to STs, 195 and 208 (CC92), harboring OXA-23-resistant determinant occur to be globally disseminated. 58 STs belonging to clonal complexes 92 (ST92, ST195, ST393, ST425, ST426); 108 (ST396, ST397); and 254 (ST254) have been reported from isolates in Malaysia. The whole-genome analysis of an extensively drug-resistant clinical isolate of A. baumannii AC12 from Malaysia also revealed that it belongs to ST195 and hence to the lineage of international clone II (IC-II) group. 59 Carbapenem-resistant A. baumannii belonging to IC-II, that is, CC92, is prevalent in many Asian countries such as India, Malaysia, Thailand, Singapore, Hong Kong, South Korea, Philippines, Taiwan, and China. It can be concluded that diversification of clones in this population has led to the clonal expansion of resistant lineage belonging to IC-II.
In conclusion, results of the present study shed light on the diversity of A. baumannii strains circulating in our setting and help us in better understanding the underlying molecular epidemiology of this bacterium in our hospital as well as in Malaysia. This study provides us and the Ministry of Health (MOH) with important data, which can be used in exploiting its potential in determination of outbreaks and for investigation of pathogen-associated antibiotic resistance trends in Malaysia.
Nucleotide accession numbers
The gyrA (strain N20227) and parC (strain N21649) nucleotide sequences have been deposited in GenBank under the accession numbers KX192333 and KX192334, respectively.
Footnotes
Acknowledgments
This work is funded by a grant from the Faculty of Medicine, Universiti Kebangsaan Malaysia (Grant No. FF-004-2012). The authors would like to thank the Universiti Kebangsaan Malaysia for providing studentship to S.B. and to the staff at the Department of Medical Microbiology & Immunology, Faculty of Medicine, Universiti Kebangsaan Malaysia for their assistance during the study.
Disclosure Statement
No competing financial interests exist.