
Abstract
The aim of this study was to detect the decreased susceptibility to azithromycin (DSA) and associated mechanisms in Shigella from China. Three hundred and ninety-two Shigella isolates, including 134 Shigella flexneri and 258 Shigella sonnei isolates, were examined for minimum inhibitory concentrations (MICs) and zone sizes to azithromycin by broth microdilution and disk diffusion methods, respectively. The MICs were compared with corresponding zone diameters to find whether there was uniformity between both tests. Twelve macrolide-resistant genes located on mobile elements were determined for the DSA isolates by PCR, and chromosomal efflux pump activity was analyzed using Phe-Arg-β-naphthylamide inhibition test and quantitative real-time PCR. Shigella isolates displayed MICs of 0.125–512 μg/ml and zone sizes of 6–26 mm against azithromycin. There were 80 (20.4%) isolates to be DSA. No significant difference was found between the DSA rates of S. flexneri and S. sonnei isolates (p = 0.052). There was an intimate relativity between MICs and zone diameters (p < 0.001). Only the plasmid-borne mphA conferring high-level DSA was detected in 55.0% (44/80) DSA-Shigella isolates. This study highlighted the prevalence of DSA-Shigella and mphA in the region studied. Clinical laboratories and clinicians should pay attention to the elevated azithromycin MICs in Shigella spp.
Introduction
S
The treatment of shigellosis can reduce the duration and severity of the infection. However, with the long-term excessive use of antibiotics, the resistant Shigella, such as extended-spectrum β-lactamase (ESBL)-producing isolate, has been prevalent worldwide.4,5 In China, ESBL-producing Shigella has been reported in recent years. 6 Also, the occurrence of ESBL-producing isolates with multidrug resistance (MDR) makes it more difficult to treat Shigella infection due to less choice of effective antibiotics.
Azithromycin belongs to the macrolide antibiotics, which have primarily been used to treat infections of Gram-positive microorganisms; however, this drug has also displayed good effect against diverse Gram-negative organisms. 7 The American Academy of Pediatrics and the Infectious Diseases Society of America have recommended to use azithromycin for the treatment of MDR Shigella infection.8,9 However, until now, there are no interpretive criteria for azithromycin susceptibility testing of Shigella. A report by Howie et al. 10 displayed the sensitive wild-type distribution of minimum inhibitory concentrations (MICs) of azithromycin to range from 4 to 16 μg/ml, and an isolate with MIC >16 μg/ml is defined as decreased susceptibility to azithromycin (DSA).
In most studies, DSA-Shigella isolates were validated to carry plasmid-borne mphA gene, which encodes a macrolide-2′-phosphotransferase mediating macrolide resistance.10–15 Except for the mphA, other molecular mechanisms have also been described in the development of DSA, such as the determinants located on mobile genetic elements (mphB, ermA, ermB, ermC, ereA, ereB, mefA, msrA, ermF, ermT, and ermX),16–18 punctual mutations in genes rplD (encoding the L4 ribosomal protein), rplV (encoding the L22 ribosomal protein) and rrlH (23S rRNA), and chromosomal efflux pumps (such as OmpA and OmpW).7,19 Due to the horizontal transmission ability among bacteria, the prevalence of mobile element-located resistance genes is a bigger challenge for controlling the spread of reduced azithromycin susceptibility compared with the other two.
To the best of our knowledge, the susceptibility of Shigella spp. to azithromycin has not yet been recorded in mainland China. Therefore, the aims of this study were to detect the azithromycin MICs of Shigella and determine the mobile element-mediated genes and efflux pumps related to raised MIC values. In addition, the MIC values were also compared with corresponding disk diffusion zone diameters to find whether there was correlation between both test methods.
Materials and Methods
Bacteria isolates
Three hundred and ninety-two nonduplicate Shigella isolates were gathered from the feces of different diarrhea patients in Hangzhou City of Zhejiang Province [n = 356, including 112 Shigella flexneri (S. flexneri) and 244 Shigella sonnei (S. sonnei), isolated from January 2008 to December 2012] and Shanghai City (n = 36, including 22 S. flexneri and 14 S. sonnei, isolated during 2007 and all were ESBL producers), China. Of the 356 Hangzhou strains, 184 were ESBL positive, including 58 S. flexneri and 126 S. sonnei, and 172 were ESBL negative, including 54 S. flexneri and 118 S. sonnei. The molecular characteristic and antibiotic susceptibility of all these isolates had been previously described.6,20
Susceptibility testing of azithromycin
Susceptibility of azithromycin (reference powder, Sensititre; Trek Diagnostics, Westlake, OH; 15 μg disc, Oxoid, Basingstoke, United Kingdom) for all Shigella isolates were determined by broth microdilution and disk diffusion methods, respectively, according to the Clinical and Laboratory Standards Institute guidelines (CLSI). 21 DSA is defined as MIC of azithromycin >16 μg/ml.8,11 The susceptibility detection was carried out thrice. Staphylococcus aureus ATCC 29213 and ATCC 25923 were used as quality control strains for the MIC and disk diffusion testing, respectively.
MICs of azithromycin in the existence of efflux pump inhibitor
The azithromycin MICs of DSA isolates were examined by adding efflux pump inhibitor Phe-Arg β-naphthylamide (PAβN) (20 μg/ml) (Sigma, St Louis, MO)] to ascertain whether the PAβN-inhibitable efflux pumps were active. 19 A decrease of ≥4-fold in azithromycin MIC denoted the existence of an efflux pump. 22 The effect of this concentration of PAβN on the viability of Shigella was also evaluated. The testing was performed in triplicate for each isolate.
Determination of macrolide-resistant mechanisms
Genomic DNA of DSA-Shigella was prepared by boiling method and obtaining the supernatant after centrifugation at 12,000 g for 5 min. Macrolide resistance determinants encoded in mobile genetic elements (mphA, mphB, ermA, ermB, ermC, ereA, ereB, mefA, msrA, ermF ermT, and ermX) were detected using the primers as described previously.16–19 A representative PCR product for each determinant was sequenced to verify that primers amplified the target genes.
Quantitative real-time PCR for efflux pump gene
The expression levels of outer membrane proteins A and W genes (ompA and ompW) were examined by quantitative real-time-PCR (qRT-PCR), according to document described by Gomes et al. 19 qRT-PCR was run in triplicate. Negative and genomic DNA contamination controls for each gene were included, and the housekeeping gene rpoB was used as an internal control. The 2−Δ (Δ Ct) method was used to determine relative expression of the determinants detected, and an increase of ≥2-fold 23 compared to that for S. flexneri ATCC 12022 was considered indicative of overexpression.
Statistical analysis
The χ2-test was used to analyze the differences of DSA and associated resistance gene distribution; correlation between the MIC values and the inhibitory zone diameters was carried out by Spearman Rank Correlation test (SPSS 22). A p < 0.05 was considered to be statistically significant.
Results
Susceptibility of azithromycin
Among 392 Shigella isolates, 267 (68.1%) isolates showed the azithromycin MICs between 4 and 16 μg/ml; 45 (11.5%) displayed MICs ≤2 μg/ml; and 80 (20.4%) revealed MICs ≥32 μg/ml (DSA-Shigella). The azithromycin MICs among 134 S. flexneri isolates ranged from 0.125 to >512 μg/ml with an MIC50 of 8 μg/ml and MIC90 of 32 μg/ml, whereas the MICs among 258 S. sonnei isolates ranged from 0.25 to >512 μg/ml with an MIC50 of 16 μg/ml and MIC90 of 128 μg/ml. The azithromycin MICs ranged from 0.125 to >512 μg/ml with an MIC50 of 16 μg/ml and MIC90 of 32 μg/ml for 172 ESBL-negative isolates and from 0.125 to >512 μg/ml with an MIC50 of 16 μg/ml and MIC90 of 256 μg/ml for 220 ESBL-producing isolates (data not shown).
Of 80 DSA-Shigella isolates, 20 (8 ESBL-negative and 12 ESBL-positive isolates) were S. flexneri and 60 (22 ESBL-negative and 38 ESBL-positive isolates) were S. sonnei. No significant difference was found between the DSA rates of S. flexneri and S. sonnei isolates [14.9% (20/134) vs. 23.3% (60/258), p = 0.052] (Table 1) or those of ESBL-negative and ESBL-positive Shigella isolates [17.4% (30/172) vs. 22.7% (50/220), p = 0.198] (Table 2).
p < 0.05 was considered statistically significant.
DSA, decreased susceptibility to azithromycin; S, susceptibility.
p < 0.05 was considered statistically significant.
ESBL, extended-spectrum β-lactamase.
For disk diffusion test, our isolates exhibited azythromicin inhibition zone between 6 and 26 mm, and there were 83 (21.2%, 83/392) isolates with inhibitory zone <15 mm. Two zones of inhibition were found in 57 Shigella isolates (51 S. sonnei and 6 S. flexneri isolates) with MIC values from 1 to 128 μg/ml. For these isolates, the diameters of the outer zones and inner zones ranged from 22–30 mm to 13–21 mm, respectively. Compared with S. flexneri isolates, S. sonnei isolates were more prone to occur in dual zones [19.8% (51/258) vs. 4.5% (6/134), p < 0.001]. Compared with ESBL-producing isolates, ESBL-negative isolates were more likely to produce two zones [11.4% (25/220) vs. 18.6% (32/172), p = 0.044] (Table 3). At present, the clinical significance of two zones is not clear. Therefore, we used the diameter of inner zone to interpret the susceptibility for our Shigella isolates.
The median for each group is listed.
Numbers in parentheses, range.
p = 0.044.
p < 0.001.
Correlation of MICs of azithromycin with zone sizes
In another study, Lluque et al. 24 used inhibitory zone size <15 mm (15 μg/disk) as the break point for the screening of DSA-Shigella. Therefore, in this study, we evaluated the correlation between the results of microdilution and disk diffusion methods for the sensitivity detection. Significant correlation was observed between MICs and inhibition zone sizes (Spearman rank correlation coefficient = −0.542, p < 0.001). In Figure 1 the MIC values were plotted against the inhibition zone sizes for the 15 μg disk. According to the interpretive zone size above, setting the break point of DSA at ≥32 μg/ml and susceptibility at ≤16 μg/ml, a good separation was gained for the disk. For the disk interpretative zone sizes of DSA, <15 mm led to 5.36% (21/392) strains with major errors (the zone diameters of 3.06% isolates with ≤16 μg/ml were less than 15 mm, and those of 2.30% isolates with ≥32 μg/ml were ≥15 mm) (data not shown).
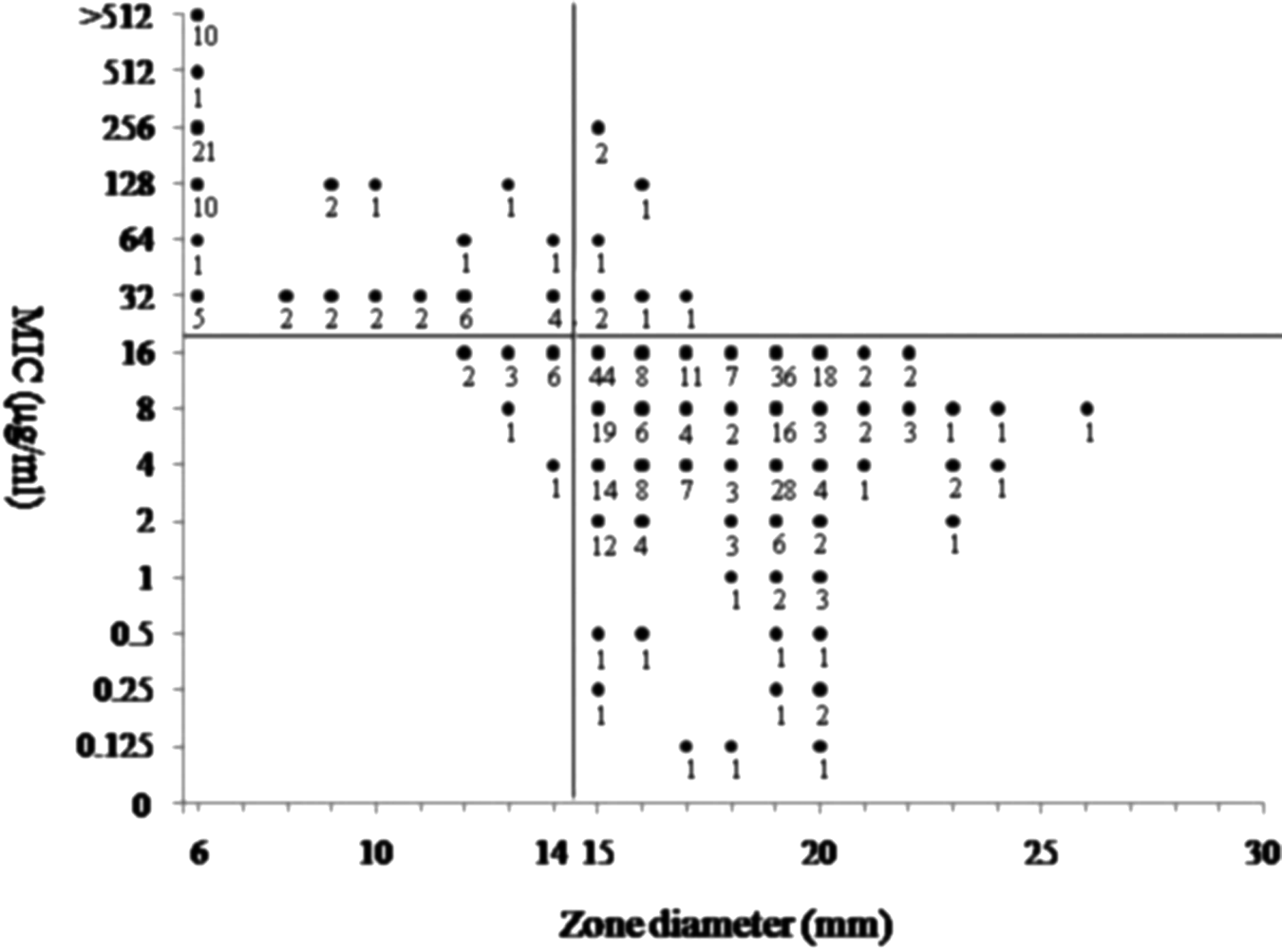
Scatterplot of azithromycin MIC versus zone diameter (15 μg disk) with proposed tentative interpretive breakpoints (n = 392). The digit under each dot is the number of isolates. MIC, minimum inhibitory concentration.
Macrolide resistance genes
Among the 80 DSA-Shigella isolates, 44 (55.0%) were plasmid-mediated mphA gene positive. All isolates were negative for genes mphB, ermA, ermB, ermC, ereA, ereB, mefA, msrA ermF, ermT, and ermX (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/mdr). Of 44 isolates with mphA, 41 (93.2%) exhibited high-level DSA (MICs ≥64 μg/ml). A significant difference was found in the distribution of the mphA gene between ESBL-positive and ESBL-negative isolates (64% vs. 40%, p = 0.0367). However, there was no significant difference between S. flexneri and S. sonnei isolates (p = 0.119) (Supplementary Table S1).
Activity of efflux pump
The survivability of bacteria was not affected by the existence of PAβN (20 μg/ml) only. No significant differences in the azithromycin MIC levels of all the DSA-Shigella were found when compared with those in the absence of an inhibitor. The qRT-PCR results also showed that no overexpression was found in the mRNA levels of efflux genes ompA and ompW related to decreased azithromycin susceptibility in all the DSA-Shigella isolates (Supplementary Table S1).
Discussion
At present, the occurrence and prevalence of MDR-Shigella lead to reduction in the choice of available drugs. Therefore, there is an increasing requirement for therapeutic measures. Azithromycin used to treat shigellosis is one of the measures. Also, the insusceptibility of Shigella to azithromycin in China causes our concern.
Although presently no CLSI or EUCAST (European Committee on Antimicrobial Susceptibility Testing) breakpoints exist for azithromycin and Shigella, the prevalence of DSA among Shigella was reported by some studies according to the interpretation criteria indicated by Howie et al. 10 In the Bay of Bengal in India, the DSA rate is 48% in Shigella isolates from 2006 to 2011. 25 In America, in 2011 and 2012, the DSA rate of isolates (MIC >32 μg/ml) was 3.1% and 4.2%, respectively. 26 Plasmid-conferred (mphA gene) DSA-S. sonnei isolates had been described in France (MIC = 64 μg/ml), Canada (MICs >64 μg/ml), and the USA (MICs >16 μg/ml).11,12,14 In this study, the prevalent rate of DSA-Shigella was 20.4% (80/392) and 66.3% (53/80), which were of MICs ≥64 μg/ml (Supplementary Table S1). In 53 isolates with MICs ≥64 μg/ml, 71.7% (38/53) were ESBL positive (Supplementary Table S1). Among the 44 DSA-isolates with the mphA, 93.2% had the MICs from 64 to >512 μg/ml, which is in line with the report by Baker et al., 27 that mphA mediates a high level of DSA (MIC ≥64 μg/ml).
Acquired macrolide resistance may arise from various mechanisms. In Enterobacteriaceae, macrolide resistance mechanisms include target site modification by methylases encoded by erm genes, drugs inactivation by enzymes, such as esterases encoded by ere determinants or phosphotransferases encoded by mph genes, and acquisition of efflux pumps, such as mefA and msrA. 16 All of these mechanisms can mediate resistance to erythromycin and azithromycin. 16 Fortunately, except for the mphA, no other genes were detected in this study. In addition, macrolide resistance may be correlated with the mutations of rllH (23S rRNA), rplD, and rplV genes, as well as with the presence of outer membrane proteins.7,19 The results of PAβN inhibition test and qRT-PCR for ompA and ompB showed that the outer membrane proteins did not play a role in the decreased susceptibility of Shigella to azithromycin. Therefore, for the DSA-Shigella isolates without transferable resistance determinants (36 isolates) in this study, the chromosomal mutations of the 23S rRNA, rplD, and rplV genes could be the resistance mechanisms.
Several studies have reported that some mutations (including point mutation, insertion, and deletion) in the extended loop of ribosomal proteins L4 (encoded by rplD) and L22 (encoded by rplV) and the domain V of 23S rRNA conferred macrolide resistance.7,28,29 Unfortunately, we did not detect the nucleotide sequence changes of the specific regions of the three genes. Of course, the presence of point mutations of the aforementioned genes amplified in the primer binding sites causing a negative PCR might be one of the explanations for the DSA. It was another limitation of this study that we could not verify this speculation by Southern blot with macrolide-resistant gene, such as mphA, as a probe.
In this study, we analyzed the correlation of MICs with the zone diameters to evaluate the value of disc diffusion method in the detection of DSA-Shigella isolates. A close retrocorrelation was found between the two variables. Although there were 3.06% of false DSA rate and 2.30% of false sensitivity rate using azithromycin disk compared to the MIC values, we think that the interpretation of zone size <15 mm can be used for the screening of DSA-Shigella.
Two-zone phenomenon of azithromycin susceptibility testing was reported in Shigella previously.30,31 This could lead to the same isolate being interpreted as sensitive by the outer zone, but DSA by the inner zone. Therefore, it should be indicated that the dual inhibitory zones yielded by azithromycin by the disk diffusion method generated complexity in the explanation of findings. In addition, our results showed that S. sonnei isolates and ESBL-negative isolates were more likely to yield two inhibitory zones than S. flexneri isolates and ESBL-positive isolates. The causes resulting in the phenomenon of two zones and the occurrence tendentiousness of dual zones among isolates are unknown.
Recently, some investigators found that shigellosis can be transmitted among MSM (men who had sex with men) patients, in whom oroanal sex and concurrent infection with HIV significantly increase infection rate. 27 A USA retrospective study showed that among 55 DSA-Shigella isolates from 2002 to 2013, 81% were isolated from HIV patients and 79% were identified as gay, bisexual, or other MSM. 13 Baker et al. 27 described the intercontinental spread of DSA shigellosis in MSM by sexual dissemination. Therefore, in future monitoring and research work, we should pay more attention to this population.
The clinical implication of in vitro decreased susceptibility of Shigella to azithromycin is not still clear because this drug can reach high intracellular concentration in leukocytes, colonic cells, and stool, 32 but azithromycin treatment failure has been described in sufferers with shigellosis.14,33 In addition, the emergence and prevalence of DAS-Shigella in the face of high resistance rate of ampicillin and trimethoprim–sulfamethoxazole, and third-generation cephalosporin resistance, are worrying for children infections in China because the remaining choice for therapy is fluoroquinolones such as ciprofloxacin and levofloxacin, which may cause cartilage toxicity and are not recommended for use in children. We expect that clinical laboratories and clinicians pay attention to the variation in the distribution of azithromycin MICs and the prevalence of the highly mobile DSA-conferring plasmid. In addition, the official breakpoints of Shigella spp. to azithromycin should be developed to allow the laboratories to report the susceptibility results to clinicians with confidence.
Footnotes
Acknowledgments
This work was supported by grants from Zhejiang Province Medical Science and Technology Projects (2015KYA194), Xiaoshan District, Major Scientific and Technological Research Projects (2013314), Natural Science Foundation, Science and Technology Commission of Shanghai (12ZR1425000), and the National Natural Science Foundation of China (81371872).
Disclosure Statement
All authors report no conflicts of interest relevant to this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.