
Abstract
Aim:
To perform a retrospective analysis of the high occurrence of Clostridium difficile infection in the surgical department of a Czech tertiary care hospital and to identify weaknesses in C. difficile infection (CDI) prevention and control policies.
Methods:
Clinical and epidemiological data on eleven CDI cases were collected. C. difficile isolates were characterized by capillary electrophoresis ribotyping, multilocus variable tandem repeat analysis (MLVA), gyrA gene fragment sequencing, and erm(B) fragment PCR amplification. Antibiotic susceptibility to metronidazole, vancomycin, ciprofloxacin, moxifloxacin, and clindamycin was tested.
Findings:
Eleven CDI cases were caused by C. difficile PCR ribotype 001 strains. These strains revealed two different MLVA profiles with 11 tandem repeat differences. All isolates were susceptible to metronidazole and vancomycin and resistant to ciprofloxacin (MIC ≥32 mg/L), moxifloxacin (MIC ≥32 mg/L), and clindamycin (MIC ≥256 mg/L). All isolates revealed amino acid substitution Thr82Ile, in the GyrA and were erm(B) negative.
Conclusion:
Two fluoroquinolone and clindamycin-resistant C. difficile PCR ribotype 001 strain clusters occurred at one of the surgical departments of a tertiary care hospital. Ineffective decontamination with suboptimal concentration and time of exposure of sporicidal disinfectants may have resulted in C. difficile transmission.
Introduction
C
C. difficile infection (CDI) incidence and CDI testing frequency vary widely in European countries (0.7–28.7 cases per 10,000 patient bed days; 4.6–223.3 tests per 10,000 bed days). 5 Underdiagnosed CDI cases due to suboptimal CDI laboratory algorithms and/or a low CDI testing frequency have undoubtedly contributed to the increasing CDI incidence trend.
Molecular typing allows differentiation of individual C. difficile isolates from each other. PCR ribotyping is the recommended typing method for CDI surveillance. 6 Application of capillary electrophoresis for detection of amplified 16S and 23S intergenic region fragments provides better discrimination power than gel-based ribotyping and, moreover, allows laboratory data exchange.7,8
Some C. difficile genotypes, such as PCR ribotype 027, appear to be more epidemically successful, with a large number of reported national outbreaks 9 and tracking of worldwide clonal spread by whole-genome sequencing. 10 Whereas PCR ribotype 027 has spread worldwide, other PCR ribotypes have been restricted to specific geographic areas; for example, PCR ribotype 244 in Australia 11 and PCR ribotype 176 in Poland 12 and the neighboring Czech Republic. 13 An outbreak association of other C. difficile types not from the PCR ribotype 027 family was reported, e.g., toxin A-negative PCR ribotype 01714,15 and PCR ribotype 106. 16
To detect the clonal spread of C. difficile belonging to the same ribotype requires the use of another subtyping technique, such as multilocus variable tandem repeat analysis (MLVA)17,18 or whole-genome sequencing.19,20 A concordance of 95% in potential outbreak investigation was found between MLVA and whole-genome sequencing. 21
In 2014, a fivefold higher CDI incidence at the surgical department was observed in comparison with the overall CDI incidence in the hospital. In response, we performed retrospective analysis to identify potential CDI outbreak risks and weaknesses in departmental CDI prevention and control policies.
Methods
Infection prevention control measures before and during increased CDI incidence
Appropriate hand hygiene and use of protective clothing
When contact with a CDI case occurred, healthcare workers, patients, and visitors washed their hands using soap and water, and after drying their hands, they used alcohol-based hand cleanser to avoid transmission of other nosocomial pathogens. The department staff used disposable gloves for every contact with patients and they also had to wear the disposable coat provided at every entrance to the department.
Environmental cleaning
Over the duration of the multiple CDI occurrences, admission of new patients was suspended and daily deep cleaning with sporicidal disinfectants (Persteril and Oxiper) was ordered. After the last patient was discharged, the surgical ward was closed and a complete environmental decontamination was performed.
When CDI occurred, cleaning was performed three times daily for frequently touched surfaces and twice daily for other surfaces (floor), and two sporicidal disinfectants (Persteril and Oxiper) were used alternately. Persteril, based on hydrogen peroxide in combination with peracetic acid, was used at the manufacturer's recommended concentration of 5,000 ppm and 30-minute exposure. Oxiper, based on hydrogen peroxide in combination with quarternary ammonium, was used at the manufacturer's recommended concentration of 2,500 ppm and 30-minute exposure.
Microbiological methods
Hospital CDI testing algorithm
Diarrheal stools are tested only at the physician's request. As a first diagnostic step, a dual lateral flow immunoenzymatic assay (Quik Chek complete, Alere) was used, which detects the presence of glutamate dehydrogenase and toxin A/B simultaneously in the stool sample. Stool samples that tested positive for GDH and toxin A/B or GDH only were cultured for the presence of C. difficile on a selective agar medium (Oxoid; C. difficile Selective Brazier's Medium, PB5191A) after an alcohol shock treatment. Selected C. difficile isolates were sent to the Department of Medical Microbiology of Motol University Hospital for molecular typing.
Ribotyping, toxin gene multiplex PCR, MLVA
Capillary electrophoresis ribotyping was performed according to the standard operation protocol (www.ecdisnet.eu) using primers published by Stubbs et al. 22 The Leeds-Leiden C. difficile reference strain collection was used to determine the ribotype.
The presence of genes for toxin (A, B, binary) production was investigated by multiplex PCR. 23
MLVA was performed by amplification and sequencing of seven previously published loci (A6Cd, B7Cd, C6Cd, E7Cd, F3Cd, G8Cd, and H9Cd) 17 with change of reverse primer for locus G8Cd. 24 The sum of tandem repeat difference (STRD) was counted manually after sequence software processing (Sequencing Analysis Software, Applied Biosystems).
Antibiotic susceptibility testing and molecular resistance mechanism investigation
Susceptibility to metronidazole, vancomycin, ciprofloxacin, moxifloxacin, and clindamycin was determined by E-test (Liofilchem) on Wilkins-Chalgren agar. Clinical breakpoints of 8 mg/L for clindamycin, 4 mg/L for ciprofloxacin, 25 4 mg/L for moxifloxacin, and 2 mg/L for metronidazole and vancomycin 26 were assessed. The molecular mechanism of resistance to fluoroquinolones was investigated by amplification and sequencing of the gyrA gene 27 and to clindamycin by amplification of the erm(B) gene fragment. 28
Results
CDI case history
Four CDI cases occurred from January 2014 to the end of February 2014 (patients 1–4) and six CDI cases occurred from November 2014 to the end of December 2014 (patients 6–11) in the surgical department (17 beds) of the tertiary care hospital (900 beds). Between these two multiple CDI case occurrences, one CDI case, ostensibly unrelated, was observed (patient 5, March 2014). All eleven CDI cases were considered as healthcare-associated infections. Ten patients (Fig. 1, patients 2–11) developed symptoms of CDI more than 48 hours after admission and one patient (Fig. 1, patient 1) showed the onset of CDI at the time of admission, but she had been transferred from another healthcare facility. Detailed CDI timelines are depicted in Fig. 1.
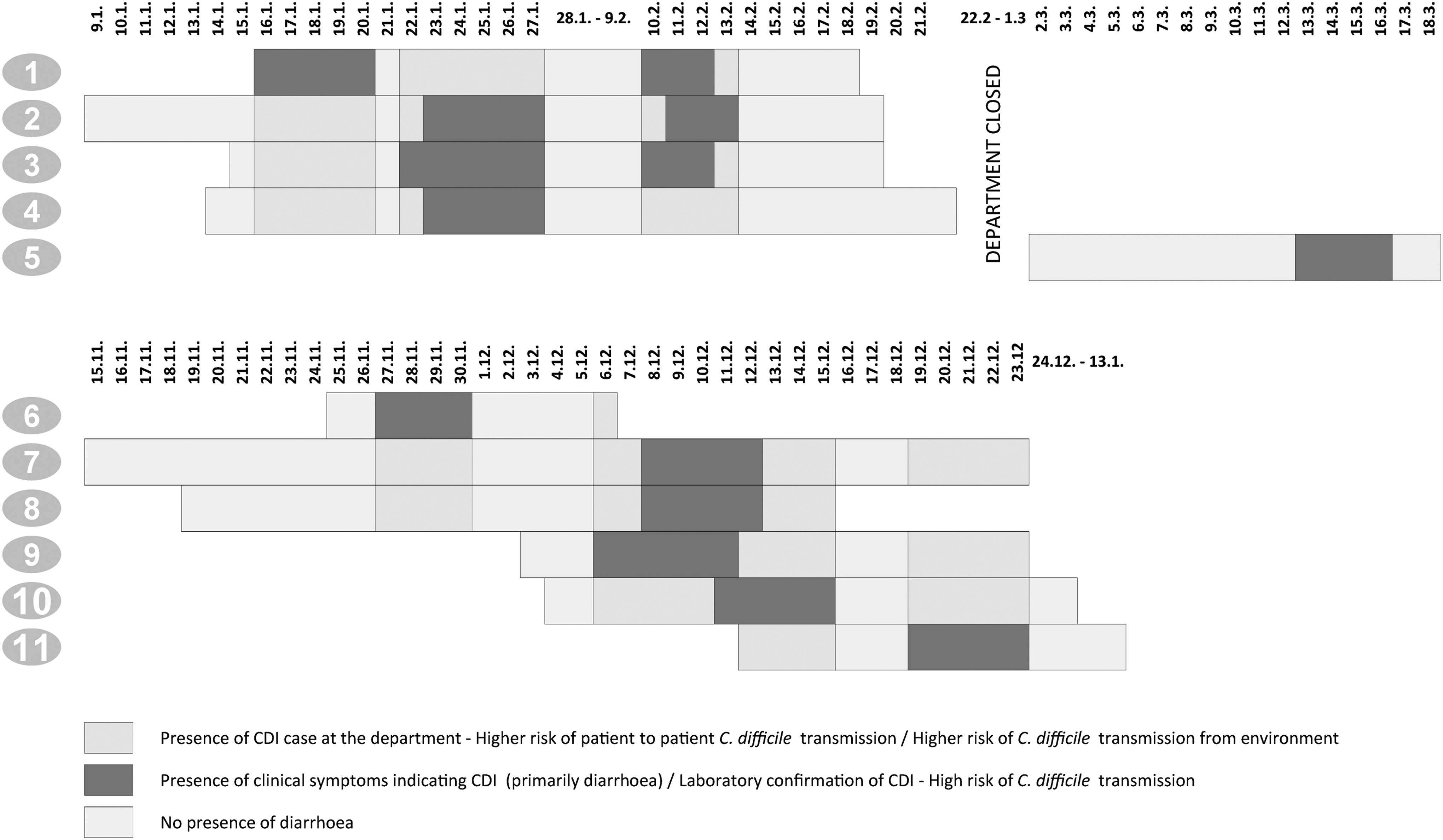
Each line represents the timeline of hospitalization of the patient. The presence and no presence of diarrhea are marked in black and gray color. Dark gray color indicates the higher risk for Clostridium difficile transmission for other patients due to the presence of CDI at the department. CDI, C. difficile infection.
Three patients had a recurrent episode of CDI (patients 1–3). CDI incidence in the surgical ward was 13.7 cases per 10,000 patient bed days or 94.9 cases per 10,000 admissions. The overall hospital CDI incidence was 2.7 cases per 10,000 patient bed days or 23.1 cases per 10,000 admissions.
Of 11 patients, 9 were males and 2 females. Average age was 70.7 years. All patients had used antibiotic therapy in previous months. The spectrum of antibiotics in combination or monotherapy was as follows: lincosamides (n = 5), cephalosporins (1st generation n = 3 and 2nd and 3rd generation n = 1), 2nd generation of fluoroquinolones (n = 3), piperacillin/tazobactam (n = 3), oral penicillins (n = 2), aminopenicillins (n = 1), and carbapenems (n = 1). CDI-specific antimicrobial therapy was initiated in all 11 CDI cases. Metronidazole was used together with vancomycin in all 11 cases, and, in one patient, in combination with fidaxomicin (fulminant CDI, leucocytosis 40.1 × 109/L). All three recurrences were treated with fidaxomicin. Characteristics of patients are summarized in the Table 1. The timeline of individual CDI cases is shown in Fig. 1.
CDI, C. difficile infection.
Microbiological data
A total of 11 C. difficile isolates were sent for molecular typing. CE ribotyping revealed the same electrophoretic profile belonging to PCR ribotype 001.
Subtyping by MLVA divided the isolates into two groups. The first MLVA profile A (5 isolates) was A6Cd = 41, B7Cd = 18, C6Cd = 33, E7Cd = 4, F3Cd = 6, G8Cd = 6, and H9Cd = 1 and the second MLVA profile B (6 isolates) was A6Cd = 35, B7Cd = 21, C6Cd = 35, E7Cd = 4, F3Cd = 6, G8Cd = 6, and H9Cd = 1. The sum of the tandem repeat differences between these two MLVA profiles was 11.
MLVA profiles corresponded with multiple CDI occurrence timelines. The causative C. difficile strain of one solitary CDI case (Fig. 1, patient 5, CDI case in March 2014) had the identical MLVA profile to the C. difficile strain A cluster.
All isolates were susceptible to metronidazole (ranged from 1.5 to 2 mg/L) and vancomycin (ranged 0.5–1 mg/L) and resistant to ciprofloxacin (MIC ≥32 mg/L), moxifloxacin (MIC ≥32 mg/L), and clindamycin (MIC ≥256 mg/L). All isolates (n = 11) revealed amino acid substitution, Thr82Ile, in the GyrA and they were erm(B) negative.
Discussion
In the period January to December 2014, a fivefold higher CDI incidence was observed at the surgical ward (13.7 cases per 10,000 patient bed days or 94.9 cases per 10,000 admissions) compared with the hospital CDI incidence (2.7 cases per 10,000 patient bed days or 23.1 cases per 10,000 admissions).
The hospital CDI incidence showed the constant rates (2.8 cases per 10,000 patient bed days or 20.6 cases per 10,000 admissions in 2013 and 2.8 cases per 10,000 patient bed days or 23.9 cases per 10,000 admissions in 2015) lower than was reported for the Czech Republic (6.2 CDI cases/10,000 patient bed days or 35.1 CDI cases per 10,000 admissions in 2012–13). 4 CDI incidence at the surgical ward, in comparison with the hospital CDI figures, revealed higher changing rates (11.5 CDI cases/10,000 patient bed days in 2012–2013 or 80.0 CDI cases per 10,000 admissions and 4.9 CDI cases/10,000 patient bed days or 34.0 CDI cases per 10,000 admissions in 2015).
The causative C. difficile strains were typed as PCR ribotype 001. This ribotype is one of the successful epidemic ribotypes in Europe 29 with a reported association with the lethal course of CDI. 30
In the Czech Republic, PCR ribotype 001 (20.7%) and PCR ribotype 176 (26.7%) belong to the prevailing RTs in the C. difficile strain collection (n = 2,201). 31 During the period 2013–2015, a total of 97 C. difficile isolates (2, 71, and 24, respectively) were sent for molecular typing from St. Anne's University Hospital. Of these, 54 isolates (55.7%) belonged to PCR ribotype 001 and nine isolates (9.3%) to PCR ribotype 176, which reflects the current unfavorable epidemiological situation in the Czech Republic. 31
Subtyping by MLVA divided the isolates into two groups. Eleven STRDs were found between these two MLVA profiles, which is very close to the MLVA threshold for genetically related strains (≥2 to ≤10 STRD), 17 raising the question of the possibility of their genetic relatedness.
In the Czech Republic, no recommendations for sending C. difficile isolates for molecular characterization are available. The Ontario Ministry of Health has established the threshold number of cases when CDI preventive measures are triggered: for wards of <20 beds, if two HA-CDI cases occur in 1 ward within a 7-day period or four cases of HA-CDI within a 4-week period, and for wards of ≥20 beds, if three cases of HA-CDI occur in 1 ward within a 7-day period or five cases of HA-CDI within a 4-week period. 32 Adopting these thresholds for triggering CDI preventive measures and for sending C. difficile isolates for molecular characterization to a reference laboratory could markedly improve CDI management and control.
Several factors contributed simultaneously to CDI development in patients in the study. Patients hospitalized in the surgical ward belonged to an older age group (>65 years), had chronic underlying disease, and used repeated prolonged antimicrobial therapy with majority representation of cephalosporins, clindamycin, and quinolones. These antimicrobial drugs belong to the group of high-risk CDI-associated antibiotics. 33 The restricted use of these specific groups of antibiotics (cephalosporins, clindamycin, and quinolones) to minimize patient susceptibility was one of the key factors that led to decreasing CDI hospital incidence in several studies. 33
All C. difficile isolates in this study revealed resistance to ciprofloxacin, moxifloxacin, and clindamycin. Resistance of C. difficile PCR ribotype 001 to clindamycin and moxifloxacin was reported in European C. difficile isolates.34–36 All isolates in the study revealed the amino acid substitution Thr82Ile, in the GyrA, which is associated with resistance to fluoroquinolones 27 and was also reported in C. difficile PCR ribotype 001 moxifloxacin-resistant isolates. 35 All isolates resistant to clindamycin were erm(B) negative. The erm(B) negativity in high-level clindamycin-resistant isolates is a well-known phenomenon35,37 and the molecular mechanism of resistance remains unexplained.
In both clusters of CDI, hydrogen peroxide in combination with peracetic acid at a concentration of 5,000 ppm or hydrogen peroxide in combination with quarternary ammonium at a concentration of 2,500 ppm with 30-minute exposure was used for daily cleaning as well as for terminal decontamination of the ward. These concentrations and time of exposure were probably not sufficient since Perez et al. reported that the concentration of hydrogen peroxide required for inactivation of all C. difficile spores in 10 minutes was above 7,000 ppm. 38 The inclusion of chlorine products in the disinfectant scheme would be beneficial.39,40
Implementation of Czech national guidance for infection prevention and control practices and participation in the CDI surveillance organized by the ECDC are the two most important steps for improving management and control of CDI in the Czech Republic.
Conclusion
Two C. difficile PCR ribotype 001 fluoroquinolones and clindamycin-resistant strain clusters were identified at a surgical department of a tertiary care hospital. Ineffective decontamination with suboptimal concentration and time of exposure of sporicidal disinfectants may have resulted in C. difficile spore transmission. The findings of our study stress the need for the implementation of Czech national guidance for CDI prevention and control to standardize environmental decontamination procedures as well as to define the CDI occurrence threshold as to when to send C. difficile isolates for molecular typing.
Footnotes
Acknowledgments
The authors would like to thank the ESCMID Study Group for C. difficile (ESGCD) for their professional support. This study was supported by the MH CZ–DRO, University Hospital Motol, Prague, Czech Republic 00064203.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
For this type of study, formal consent was not required.
Disclosure Statement
The authors declare that they have no conflicts of interest. O.N. received a foundation grant from the Ministry of Health, Czech Republic, in 2013–2015.