
Abstract
In this study, we have attempted to report the first clonal spread of colistin-resistant Klebsiella pneumoniae coproducing KPC and VIM carbapenemases in the neonatal unit of Rabta Teaching Hospital of Tunis (Tunisia). This retrospective study was performed from January 1, 2014 to December 31, 2014 in the Microbiology Laboratory at the Rabta University Hospital of Tunis. Twenty-one nonreplicate colistin-resistant K. pneumoniae were isolated from 19 patients hospitalized in the neonatal unit and 2 patients in the adult intensive care unit (ICU). Most of the strains were isolated from invasive specimens. Pulsed-field gel electrophoresis (PFGE) and PCR analysis and nucleotide sequencing of the blaKPC and blaVIM genes were performed. Mortality was reported in 92% of cases. All the strains were resistant to colistin (minimum inhibitory concentration [MICs] ranged from 8 to 12 mg/L). The MICs for imipenem of K. pneumoniae isolates ranged from 3 to 256 mg/L for 13 strains that were characterized as intermediate or resistant. The MICs for ertapenem were higher than 32 mg/L for the 19 resistant strains. All the isolates were sensitive to tigecycline and chloramphenicol. PFGE analysis revealed two clones (I and II). Twenty of the 21 colistin-resistant, carbapenem-resistant K. pneumoniae isolates belonged to clone I. Only one strain was related to clone II. PCR analysis and nucleotide sequencing revealed that the 20 isolates belonged to clone I, coproduced the blaKPC and blaVIM genes. A single strain (clone II), which was isolated in the ICU, did not produce KPC and VIM carbapenemases. All strains did not produce OXA-48.
Introduction
D
Materials
This retrospective study was performed from January 1, 2014 to December 31, 2014 in the Microbiology Laboratory at Rabta University Hospital in Tunis (Tunisia). Among a total of 709 K. pneumoniae isolated in our laboratory, 21 nonreplicate colistin-resistant K. pneumoniae: the resistant strains were isolated from clinical samples (blood, catheters, and pus and transtracheal aspiration) from 19 patients hospitalized in the neonatal unit and 2 patients in the adult intensive care unit (ICU). In 14 cases, the epidemiological and clinical data of patients were collected retrospectively by consulting patient files. Patient consent to the study was not required as all samples were collected as part of routine management and surveillance, and were anonymized before being used in the study.
Methods
Microbial identification and antibiotic susceptibility testing
Bacterial identification was performed on all strains using the GN card of the VITEK2® system (bioMérieux, France). Antibiotic susceptibility was assessed by disk diffusion (DD) in Mueller-Hinton agar according to the recommendations of the CA-SFM 2013. 9 Escherichia coli ATCC 25922 was used as the quality control strain. Colistin resistance was defined by an inhibition diameter around the colistin disk (50 μg) less than 15 mm and a minimum inhibitory concentration (MIC) less than 2 mg/L according to CA-SFM criteria. MIC of colistin was carried out by E-test® in keeping with manufacturers' instructions (bioMérieux, France). Extended-spectrum β-lactamase (ESBL) was detected by a double-disk synergy test between amoxicillin–clavulanic acid and a third-generation cephalosporin. An ertapenem disk (10 μg; Biorad) was used because of its high sensitivity in detecting carbapenemase-resistant strains. A reduced susceptibility to carbapenems was defined by an inhibition diameter less than 28 mm around the ertapenem disk. The MIC of ertapenem and imipenem was determined by E-test. The modified Hodge test was utilized for the detection of carbapenemase.
Molecular study of colistin-resistant K. pneumoniae strains
DNA extraction was performed by an alkaline lysis protocol as previously described. 10 Three carbapenemases simplex PCR were conducted for the detection of the following carbapenemase genes: blaKPC, blaVIM, and blaOXA-48. 11 Bidirectional sequencing was performed by Eurofins/Genomics in Germany on selected blaKPC- and blaVIM-positive isolates.
The study of colistin-resistant K. pneumoniae strains' clonality was performed by pulsed-field gel electrophoresis (PFGE) with GenePath (Bio-Rad, France) using the XbaI restriction enzyme according to the manufacturer's recommendations. The PFGE patterns were interpreted in keeping with Tenover criteria. 12 The different pulsotypes were determined with Fingerprinting II (Bio-Rad, France) according to the Dice similarity index.
Results
Clinical data of patients infected with colistin-resistant CRKP infections
The gender ratio male:female was 2:1 The strains were isolated from blood samples in 15 cases (71.5%), catheters in 4 cases (19%), and pus and transtracheal aspiration in 2 cases (9.5%). The yearly distribution of colistin-resistant CRKP strains is presented in Fig. 1. The prevalence of colistin-resistant K. pneumoniae in 2014 was 2.96%. There were no detected cases of colistin resistance in Enterobacteriaceae at Rabta University Hospital in 2013, and there have been no further cases reported since the 2014 outbreak. Fourteen relevant patient files from the neonatal unit were studied. Table 1 shows the clinical characteristics of newborns with colistin-resistant CRKP. We found prematurity in 11/14 cases (78.5%), low birthweight in 12/14 cases (85.7%), delivery by caesarean section in 11/14 cases (78.5%), and underlying maternal pathology in all the cases (100%). Mortality was reported in 12/13 cases (92%).
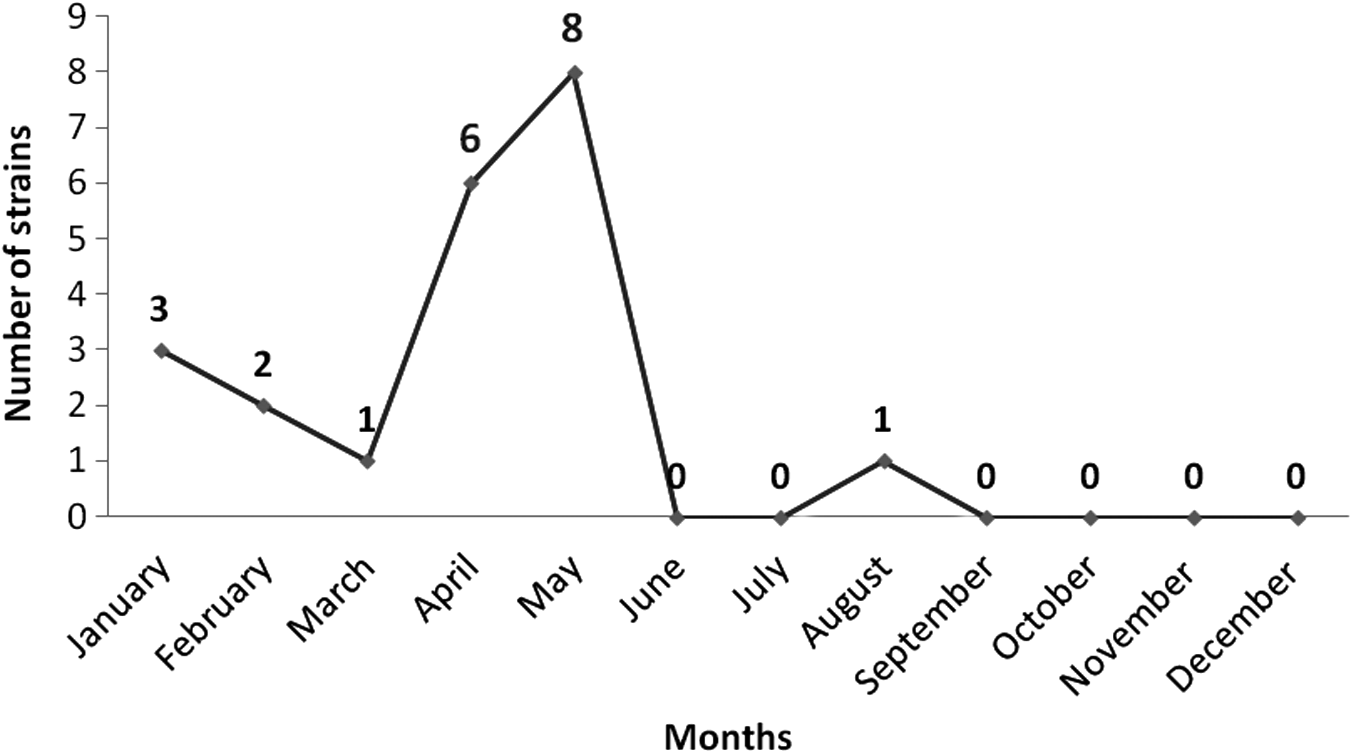
Temporal distribution of colistin-resistant CRKP strains from January 2014 to December 2014 (n = 21). Five strains were isolated between January and March, six in April, eight in May, and only one in August. CRKP, carbapenem-resistant Klebsiella pneumonia.
AMP, ampicillin; AN, amikacin; CA, chorioamnionitis; CIP, ciprofloxacin; COL, colistin; CRKP, carbapenem-resistant Klebsiella pneumonia; CT, caesarean section; CTX, cefotaxime; F, female; IMP, imipenem; M, male; MTZ, metronidazole; PRM, premature rupture of membranes; PTZ, piperacillin–tazobactam; RIF, rifampicin; VAN, vancomycin; WA, week of amenorrhea.
Patients had received multiple antimicrobial agents before the isolation of strains: colistin in 10/14 cases (71.4%), imipenem in 9/14 cases (64.3%), and ciprofloxacin in 10/14 cases (71.4%). An association of broad-spectrum antibiotics and/or antifungal therapy was observed in all cases (Table 1).
Antimicrobial susceptibility of strains
In this study, antimicrobial susceptibility testing of K. pneumoniae strains using the DD method and E-test for MIC determination revealed high rates of resistance to many drugs. With the DD method, it was observed that all isolates were resistant to amoxicillin, piperacillin, ticarcillin, amoxicillin/clavulanic acid, ticarcillin/clavulanic acid, piperacillin/tazobactam, cefotaxime, ceftazidime, ceftriaxone, cefepime, aztreonam, ofloxacin, ciprofloxacin, and aminoglycosides (gentamicin, tobramycin), but not to amikacin, which was sensitive at a rate of 61.9%. The susceptibility to fosfomycin and sulfamethoxazole/trimethoprim were 66.6% and 75%, respectively. All the isolates were sensitive to tigecycline and chloramphenicol.
The phenotypic test for ESBL production based on the synergy between third-generation cephalosporins and amoxicillin/clavulanic acid was positive in all isolates. The modified Hodge test was positive in 14 cases. The MICs for colistin ranged from 8 to 12 mg/L for all the strains that had been characterized as resistant. The MICs for imipenem of K. pneumoniae isolates ranged from 3 to 6 mg/L for 11 strains that were characterized as intermediate and 32 and 256 mg/L for two other resistant strains. Eight strains were sensitive (MICs from 0.19 to 2 mg/L). The MICs for ertapenem were higher than 32 mg/L for the 19 resistant strains. The two other strains were characterized as intermediate (MICs were, respectively, 0.75 and 1 mg/L).
Molecular study of colistin-resistant K. pneumoniae strains
The PFGE analysis results displayed in Fig. 2 reveal two clones (I and II). Twenty of the 21 colistin-resistant, CRKP isolates belong to the major clone designated clone I (Fig. 2): 19 strains from the neonatal unit and 1 from the ICU. Only one strain was related to clone II (strain Kp 6 in Fig. 1). PCR analysis and nucleotide sequencing revealed that the 20 isolates belonging to clone I coproduced the blaKPC and blaVIM genes. Only one strain, isolated in the ICU, failed to produce KPC and VIM carbapenemases (Kp 6 in Fig. 2), although its modified Hodge test was positive. All strains failed to produce OXA-48.
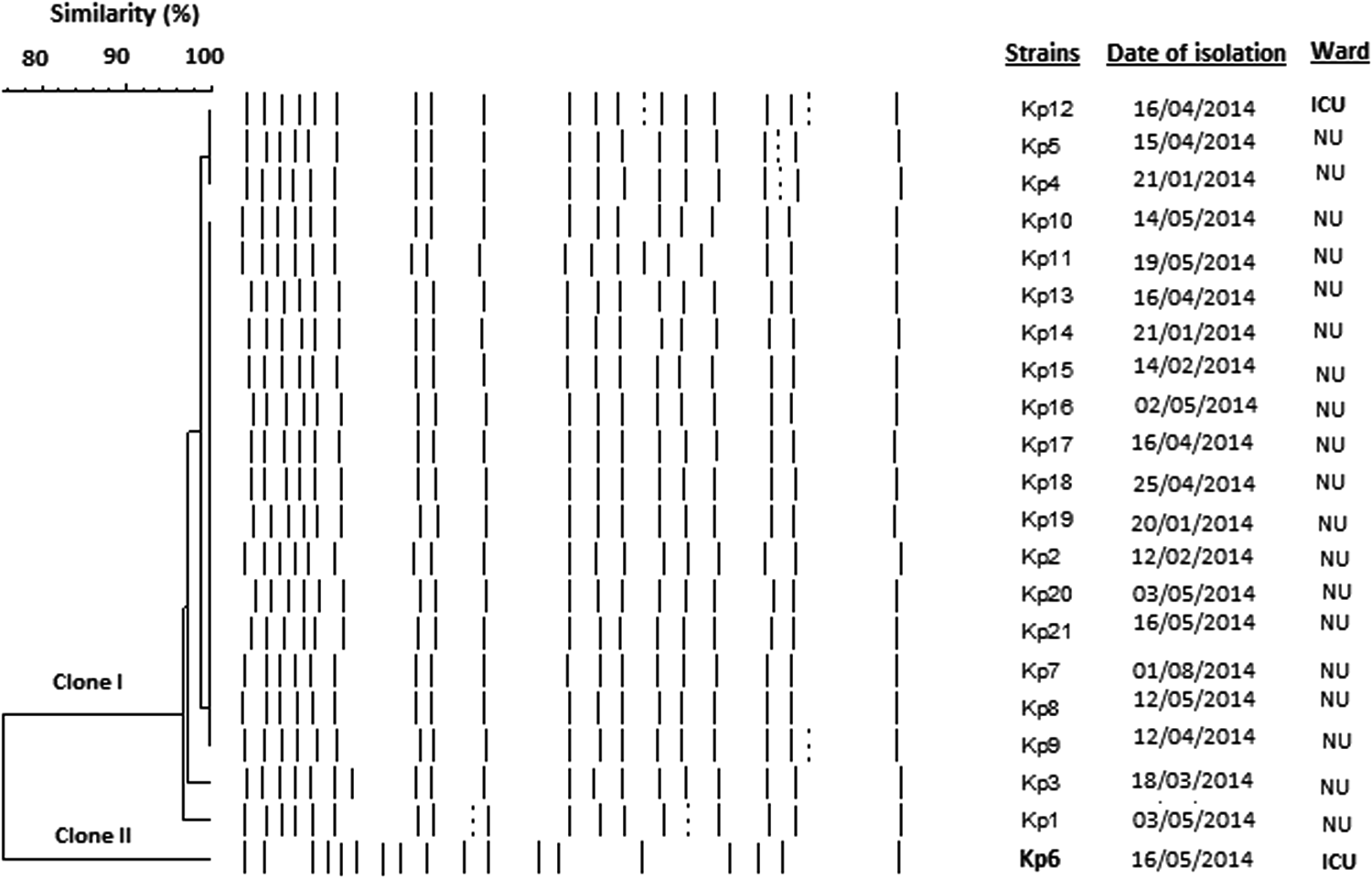
Simplified comparison of colistin-resistant K. pneumoniae pulsotypes with PFGE. A cutoff of 95% similarity (vertical line) was chosen for determination of clonal relatedness. The horizontal bar on the top left indicates the percentage similarity within the strains. The dendrogram demonstrates two clones (I and II). Twenty of the 21 colistin-resistant CRKP isolates belonged to clone I: 19 strains from the NU and 1 from the ICU. Kp6 strain was related to clone II. ICU, intensive care unit; NU, neonatal unit; PFGE, pulsed-field gel electrophoresis.
Infection control measures and interventions
Environmental sites (various surfaces in the bathrooms and patient rooms) were investigated for colistin-resistant CRKP. Screening of cultures from environmental samples did not reveal any colistin-resistant CRKP strains. Infection control measures such as hand hygiene and environmental disinfection procedures were implemented in the two wards.
Discussion
In our study, colistin-resistant K. pneumoniae were only isolated in 2014 and the prevalence was lower (2.96%) than in Taiwan (17%) and Italy (43%).13,14 Since that year, no strain of colistin-resistant K. pneumoniae has been isolated. This could be explained by an improved use of this antibiotic by physicians as well as improved environmental disinfection measures.
In our study, the outbreak of colistin-resistant K. pneumoniae strains, coharboring blaKPC and blaVIM genes, was generally limited to newborns. However, two strains were reported in adults (in the ICU). In contrast, other studies6,14 have discovered such strains in immunosuppressed adults. Most of our colistin-resistant K. pneumoniae strains were isolated from invasive specimens (blood, probably in relation with immunosuppressive factors such as prematurity, low birth weight, underlying maternal diseases) or with multiple therapies of antimicrobial agents, including colistin. The selective pressure of antibiotics, especially colistin, could be the main factor of the resistant strains' emergence and clonal spreading.1,15,16 Mortality was high (92%). Akturk et al. 1 reported a similar situation in pediatric and neonatal ICUs in Turkey, but mortality due to colonization or infection with CRKP was much lower (16.6%) in infected patients.
Clonality was evaluated by PFGE analysis, indicating the presence of a major clone (clone I). In contrast, Mezghani-Maalej et al. 5 reported a multiclonal emergence of colistin resistance in Enterobacteriaceae with 40 different pulsotypes at Sfax Hospital in Tunisia. This could be explained by a common source of contamination.
PCR analysis and nucleotide sequencing revealed that 20 isolates coproduced the blaKPC and blaVIM genes. This phenomenon of coproduction is rarely described. Usually, colistin-resistant K. pneumoniae produce carbapenemases separately.17–19 K. pneumoniae strains coharboring KPC and VIM carbapenemases have only been reported, to the best of our knowledge, in Greece, 20 Germany, 6 and Columbia. 7 Greece, among the European countries, presents the highest rates of carbapenem resistance, which is considered endemic for KPC and VIM carbapenemases. 21 All our strains of CRKP were resistant to colistin, whereas other authors found rates of resistance between 0% and 43%.7,14,22
The copresence of these two carbapenemases associated with colistin resistance is worrisome due to the possibility of widespread dissemination and further limitations on therapeutic options especially in newborns. That is why it is essential to streamline the use of antibiotics and apply infection control measures to prevent the emergence of colistin resistance.
Footnotes
Acknowledgment
We thank Dr. Ben Hassen Assia from the Bone Marrow Transplants Center from Tunis for her precious help.
Disclosure Statement
No competing financial interests exist.