
Abstract
This study was conducted to evaluate the rate of fecal carriage of Gram-negative bacilli (GNB) resistant to third-generation cephalosporins (third GC) in patients hospitalized in the intensive care unit (ICU) of Charles Nicolle Hospital of Tunis and to identify the enzymatic mechanisms involved. From February to April 2014, rectal swabs were collected from all patients (n = 38) at admission and once weekly thereafter to identify acquisition. They were cultured on desoxycholate-lactose-agar plates supplemented with cefotaxime (2 mg/L). The rate of fecal carriage of GNB resistant to third GC was 0% (0/38) at admission and the acquisition rate was 45.16% (14/31). Nineteen GNB resistant to C3G were collected from 14 patients. The major species collected were Acinetobacter baumannii (n = 5), Klebsiella pneumoniae (n = 5), and Enterobacter cloacae (n = 5). Thirteen extended-spectrum β-lactamase (ESBL) producing GNB were found; CTX-M-15 (n = 10) and CTX-M-14 (n = 1) among Enterobacteriacae and GES-12 (n = 2) among A. baumannii. Ten strains were carbapenem resistant. OXA-48 (n = 4) and NDM-1 (n = 1) were detected among Enterobacteriacae and OXA-23 (n = 5), and GES-11 (n = 1) were detected in A. baumannii. Gene encoding the ACT-16 AmpC-type-β-lactamase was detected in two isolates. All Escherichia coli isolates were assigned to group B2. Among virulence genes, prevalence of fimH, fuyA, ompT, pai, and usp were highest observed in all E. coli isolates. Among K. pneumoniae mrkD and entB were the most frequent (n = 5) followed by ybtS (n = 4) and kfu (n = 2). This study revealed a high prevalence of fecal carriage of multidrug-resistant GNB, including ESBLs, carbapenemases, and cephalosporinases producing bacteria in patients hospitalized in ICU.
Introduction
I
Materials and Methods
Study design
A prospective study, including all patients with fecal colonization due to GNB resistant to third GC was conducted in the ICU of Charles Nicolle Hospital of Tunis (Tunisia) from February 2014 to April 2014. The unit had 12 beds located in private rooms. One fecal sample per patient was analyzed at admission. For original noncarriers, follow-up cultures were performed at weekly intervals until hospital discharge. The samples were inoculated on desoxycholate-lactose-agar (DLA) plates supplemented with cefotaxime (2 mg/L) and were incubated at 37°C overnight. One colony of each morphotype was selected. Imported carriers were defined as patients found to be colonized with GNB resistant to third GC at admission.
The acquisition rate was defined as the number of patients who were not colonized at admission but become colonized afterward, divided by the number of patients not colonized at admission.
Identification and antimicrobial susceptibility testing
The API 20 E system (Bio-Merieux, Marcy L'Étoile, France) was used for the biochemical identification of all Enterobacteriaceae. Nonlactose-fermenting organisms were identified at the species level using the API 20 NE system (Bio-Merieux) and then confirmed by PCR amplification of the endogen blaOXA-51-like gene for A. baumannii. 9 Antibiotic susceptibility was determined using the agar diffusion method, as recommended by the French Society of Microbiology. 10
ESBL production was detected by the double disk synergy test (DDST). In the DDST, ceftazidime, cefotaxime, and ceftriaxone 30 mg each were placed at a distance of 15 mm edge to edge from a centrally placed augmentin disc containing 20 mg of amoxicillin +10 mg of clavulanic acid. Result was inferred if the inhibition zone around the third-generation antibiotic disks increased toward the disc containing clavulanate that is, augmentin. For enterobacteria resistant to ertapenem and for A. baumannii, the minimal inhibition concentrations (MICs) of carbapenems were determined by E-test (Bio-Mérieux SA, Marcy L'Étoile, France).
Phenotypic detection of carbapenemase
Isolates with reduced susceptibility to carbapenems: imipenem (diameter zone ≤22 mm) and/or ertapenem (diameter zone ≤18 mm) were subjected to the modified Hodge test (MHT) for carbapenemase detection as previously described. 11
Detection of metallo-beta-lactamases (MBLs) (class B): MBLs require divalent cations of zinc as cofactors for their activity. The combined disk test (IMP+EDTA) was performed as described. 12 A zone diameter difference of >4 mm between imipenem disks, and imipenem plus EDTA was interpreted as MBL positive.
Detection of class A β-lactamases: For the detection of Klebsiella pneumoniae carbapenemase, a combined disk test (MER+Boronic Acid) was performed. 13
Characterization of genes encoding β-lactamases
Whole-cell DNA was extracted by boiling a colony suspension at 100°C for 10 min, and supernatant was used as template DNA. All phenotypically confirmed ESBL-positive isolates were screened by PCR for the presence of genes encoding ESBLs (blaCTX-M, blaTEM, blaSHV, blaPER, blaVEB, and blaGES). 14 Detection of plasmid-mediated AmpC β-lactamase genes in different strains was performed by using a multiplex PCR. 15 The presence of blaIMP, blaVIM, blaNDM, blaOXA-48, blaOXA-23-like, blaOXA-24-like, and blaOXA-58-like genes encoding carbapenemases were detected by PCR as described previously. 16
PCR products were purified using a purification kit (Biomatik). DNA sequencing was performed by the dideoxy chain-termination method with BigDye_Terminator v.3.1 Cycle Sequencing Kit (Applied Biosystems) and analyzed using an ABI Prism_3100 genetic analyzer (Applied Biosystems).
Transfer of resistance determinants
Five isolates were investigated for the transferability of ESBL encoding genes. Conjugation assays were performed with overnight cultures of the donor strains and rifampin-resistant Escherichia coli J53, which were mixed in a ratio of 1:1 and incubated overnight on the surface of DLA at 37°C. Transconjugants were selected on DLA plates containing rifampin (0.1 mg/L) and cefotaxime (2 mg/L). Cotransfer of resistance markers to non-β-lactam antibiotics via conjugation was tested by the disk diffusion test. The presence of the ESBL encoding genes in transconjugants was confirmed by PCR using amplification primers and conditions previously cited.
Virulence factor-encoding genes and phylogenetic groups
PCR was used to screen E. coli isolates for the presence of 18 virulence factors and K. pneumoniae for detection of 7 virulence factors and K1/K2 capsular serotypes using previously published primers and conditions.17,18 The phylogenetic group of the E. coli isolates was determined by the PCR method developed by Clermont et al. 19
Molecular typing
The molecular epidemiology of all strains has been done by Enterobacterial repetitive intergenic consensus-polymerase chain reaction (ERIC-PCR) as previously described. 20
Results
Study population and carriage rate of GNB resistant to third GC
There were 38 admissions to the ICU during the study period. All patients had at least two swabs (range two to five swabs). GNB resistant to third GC prevalence at admission was 0% (0/38).
Of the 38 noncarriers, follow-up rectal swabs for only 31 patients resulted in a GNB resistant to third GC acquisition rate of 45.16% (14/31). The seven remaining patients were excluded (three were discharged or transferred and four died before the scheduled follow-up sampling) (Fig. 1). The median time between admission in ICU and acquisition of carriage was 6 days (range 5–15 days).
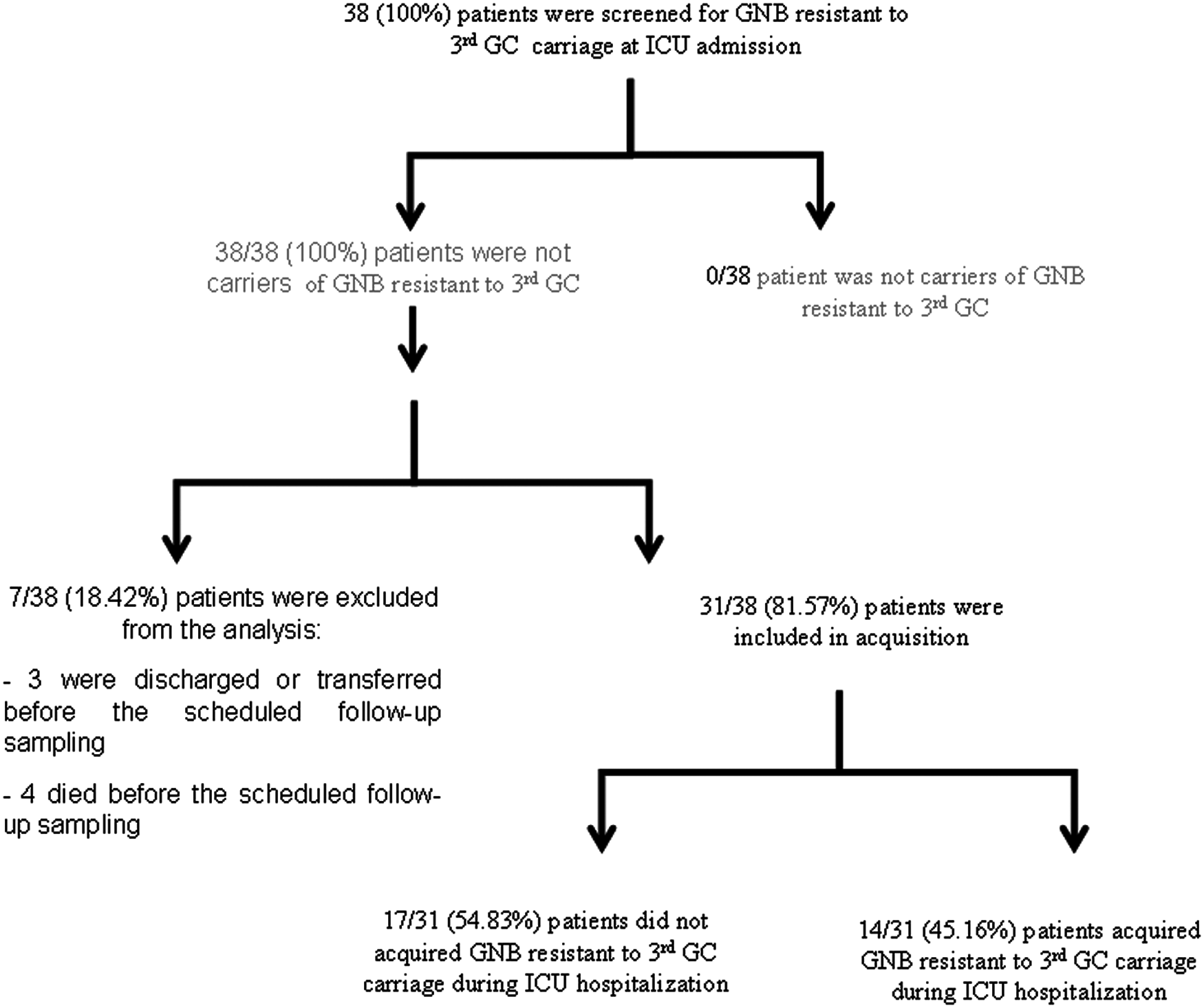
Flowchart of the patients.
A total of 19 GNB resistant to third GC were isolated: K. pneumonia (n = 5), Enterobacter cloacae (n = 5), E. coli (n = 3), Enterobacter aerogenes (n = 1), and A. baumannii (n = 5). Two different bacterial species were isolated in three patients and three in one patient (Table 1).
ERIC-PCR pattern are indicated by the letters (A, B, C, D, E, F, G, H, I, K, L).
Ecl, Enterobacter cloacae; Kp, Klebsiella pneumoniae; Ec, Escherichia coli; Ea, Enterobacter aerogenes.
ST, ESBL synergy test; S+, synergy positive; S+*, synergy positive observed after addition of cloxacillin; S−, synergy negative; +, positive; −, negative.
AKN, amikacin; CHL, chloramphenicol; CIP, ciprofloxacin; ERIC-PCR, Enterobacterial repetitive intergenic consensus-polymerase chain reaction; ESBL, extended-spectrum β-lactamase; GM, gentamicin; KMN, kanamycin; MIC, minimal inhibitory concentration; MHT, modified Hodge test; MNO, minocyclin; NAL, nalidixic acid; NET, netilimicin; NXN, norfloxacin; OFX, ofloxacin; SXT, cotrimoxazole; TET, tetracyclin; TMN, tobramycin.
Main characteristics of patients and risk factors
Among the 14 patients, there were 10 men and 4 women. Mean recipient age was 40 years (range 17–70 years). All patients had no previous hospitalization, and six patients had taken antimicrobial drugs during the last 6 months. One patient had a chronic renal failure, two had diabetes, and one had leukemia. Clinical outcomes were favorable for six patients.
The parameters for the risk factors for fecal carriage observed in our study were extreme age, sex (male), prolonged hospitalization in ICU (range: 17 days to >2 months), comorbid condition (invasive procedure, central venous catheterization, urinary catheter) observed in all patients, and underlying diseases (n = 3).
Beta-lactamases screening and antibiotic susceptibility testing
Eleven strains of enterobacterie showed a DDST positive. The antimicrobial resistance rates of E. coli, K. pneumoniae, and E. cloacae were as follows, respectively: gentamicin (67%/80%/60%), netilimicin (33%/80%/0%), tobramycin (100%/80%/60%), kanamycin (67%/80%/40%), ofloxacin (100%/100%/40%), ciprofloxacin (100%/100%/60%) norfloxacin (100%/80%/40%), nalidixic acid (100%/100%/60%), chloramphenicol (0%/20%/80%), cotrimoxazole (100%/100%/80%), tetracyclin (100%/100%/100%), and minocyclin (100%/100%/80%) (Table 1). Positive MHT were detected in 10 isolates: enterobacterie (n = 5) and A. baumannii (n = 5). Detection of MBLs was positive for only one isolate (K. pneumoniae) and detection of class A β-lactamases was negative for all isolates. The MICs of carbapenems are shown in Table 1.
Characterization of β-lactamases
Thirteen isolates (68%) harbored ESBL genes: blaCTX-M-15 and blaCTX-M-14 were detected in Enterobacteriaceae in 10 and 1 strains, respectively, and blaGES-12 (n = 2) was detected in A. baumannii isolates. Carbapenemase encoding genes were detected in 10 isolates: blaOXA-48 and blaNDM-1 were detected, respectively, in 4 and 1 enterobacteria and blaOXA-23 and blaGES-11 were detected in 5 and 1 A. baumannii, respectively. The blaTEM-1 and blaSHV-1 genes were detected in eight and seven isolates, respectively (Table 1). The gene encoding ACT-16 AmpC β-lactamsase enzyme was detected in two isolates (Ecl3 and Ecl4) (Table 1).
Transfer of resistance determinants
Transfer by conjugation of the ESBL to E. coli J53 was successful for all strains tested after the first attempt (four blaCTX-M-15 and one blaCTX-M-14 positive strains). However, cotransfer of ACT-16 enzyme was not successful despite three separate attempts. blaTEM-1 and blaSHV-1 genes were not cotransferred in any isolates tested. Depending on the strain, other resistances were cotransferred, mostly minocyclin (n = 3), tetracycline (n = 3), chloramphenicol (n = 2), rarely nalidixic acid (n = 1), tobramycin (n = 1), gentamicin (n = 1), and trimethoprim–sulfamethoxazole (n = 1) (Table 2).
Molecular characterization of E. coli and K. pneumoniae strains
Molecular typing of E. coli isolates revealed that they belonged to B2 phylogroup (n = 3) with virulence score varied from 6 to 14 (Table 3). No K. pneumoniae isolate exhibited the virulent capsular serotype K1 or K2. Among the genes encoding adhesins, only mrkD was detected. However, all K. pneumoniae isolates harbored the genes entB. Only one was negative for ybts. The ferric iron uptake system encoded by kfu was detected in two isolates (Table 3).
Molecular typing
Molecular analysis evidenced two clones among E. coli strains. Three of the five K. pneumoniae strains, which were producing CTX-M-15, were indistinguishable and four E. cloacae isolates were genetic related. Three clones were observed among the five A. baumannii strains (Table 1).
Discussion
Digestive microflora is characterized by its complexity and diversity. It is an important reservoir for potentially pathogenic GNB for patients at high risk, who include those hospitalized in ICU. 20 Various studies have focused on the digestive carriage of ESBL-producing Enterobacteriaceae during nosocomial outbreaks.21,22 This is the first survey conducted in Tunisia on the intestinal carriage of GNB resistant to third GC in ICU.
The main finding from this study is the absence of fecal carriage of GNB resistant to third GC at ICU admission. However, GNB resistant to third GC acquisition rate was alarming 45.16% (14/31), but lower than that in the report from Afghanistan (70%). 23 This rate was higher than those in a 2012 report from France (15%) 24 as well as one from Spain (11.8%) 25 and Israel (8%). 26
In our study, the main risk factors for acquisition by these strains identified are mechanical ventilation, length of extended stay, and heavy use of antibiotics, particularly broad spectrum.27,28 In this context, a study showed that even a short exposure to third GC was followed by a significant increase in digestive porting GNB resistant to third GC. 29 In our study, the notion of antibiotics within 6 months was observed in six patients, but the notion of surgery within 12 months has not been found in any of our patients. Other own individual factors may be involved as a severe underlying disease, such as diabetes, immunosuppression, and frequency of invasive techniques. The notion of invasive procedures was found in all patients. The most commonly performed maneuvers were urinary catheter (n = 14) and tracheal intubation (n = 14). The studies by Falagas and Karageorgopoulos in 2009 and Wendt and al in 2005 are consistent with our results.30,31
In our study, A. baumannii and different Enterobacteriacae species were found (K. pneumoniae, E. cloacae, E. coli, and E. aerogenes). Our results confirm those of the previous studies performed in ICU in Canada 32 and France. 33 In total, five patients carried at least two or three different third GC-resistant GNB, which might increase the risk of conjugative transfer and dissemination of plasmids carrying resistance genes. 34
The production of ESBLs is one of the most important mechanisms of antimicrobial resistance. In Tunisia, epidemiological data of the spread of ESBL-producing GNB showed a rapid diffusion since their first description in 1984. 35 Recent increase in number of ESBLs attributes to the emergence of CTX-M β-lactamase producing Enterobacteriaceae.36,37 In our study, 13 isolates were found to be ESBL producers. Among them 11 were Enterobacteriacae and 2 A. baumannii. Among the 11 ESBL producers, 10 isolates were positive for CTX-M-15 and 1 for CTX-M-14 confirmed by PCR and sequencing. Our study is in accordance with other studies, in which the most common CTX-M-type ESBL was CTX-M-15.36,38 However, many studies have confirmed that CTX-M-1 enzyme is the most dominant ESBL type in enterobacteria isolates among intestinal microbiota of healthy chickens.39–42 These enzymes have spread widely through various enterobacteria, by the transmission of plasmids and mobile genetic elements rather than by clonal dissemination of a bacterial species. 38
Moreover, two isolates (E. cloacae) carried CTX-M-15 with a novel ampC gene, ACT-16. To our Knowledge, this is the first report of this enzyme in Tunisia. Recently, ACT-16 has been reported in two NDM-1 carrying Enterobacteriaceae isolated in India. 43
GES-12 ESBLs was observed in two A. baumannii isolated in our study. These results were noteworthy because it is the first survey conducted in Tunisia on the intestinal carriage of ESBL in A. baumannii. The emergence of ESBL-producing A. baumannii strains (GES) has been described previously. 44
Another interesting finding is that we have isolated several strains (52.63%, 10/19) of A. baumannii (n = 5) and Enterobacteriaceae (n = 5) having different carbapenemase-encoding genes. Carbapenem-resistant GNB have been reported worldwide as a consequence of the acquisition of carbapenemase genes.45,46 The carbapenemases reported in the present study were OXA-48 (n = 4), NDM-1 (n = 1) found in Enterobacteriaceae and OXA-23 (n = 5), and GES-11 (n = 1) in A. baumannii. To the best of our knowledge, this is the first study reporting the NDM-1 gene in Enterobacteriacae on the intestinal carriage in our country. In Tunisia, different reports have described OXA-48 in Enterobacteriaceae, 45 and resistance to carbapenem in A. baumannii isolates has been found to be associated with the production of OXA-97 and OXA-23.46–48 To date, there are numerous reports available from many countries regarding intestinal carriage of OXA-48-producing Enterobacteriacae 49 and OXA-23-producing A. baumannii. 50 Recently, Bonnin et al. reported A. baumannii carrying NDM-1. The strain was recovered in France from a Tunisian patient. 51
The transconjugants obtained in transferability assays were positive for ESBL production according to conventional DDST and PCR. It is worth mentioning that CTX-M β-lactamase genes are widely known to be carried on a plasmid linked to mobile genetic elements that are utilized as vehicles for resistance genes horizontal movement, in addition to carry on resistance to other antibiotics such as aminoglycosides and fluoroquinolones. 52
Phylogenetic analysis of ESBL-producing E. coli isolates in our study showed that belonging to group B2, and they have a high virulence scores. Our results are in agreement with those reported in the literature. 49 In this study, fimbrial adhesins (mrkD) and siderophore (entB) were observed in all K. pneumoniae strains. This situation shows that these virulence factors are important for Klebsiella pathogenicity. Molecular epidemiologic analysis showed the circulation of clonally related strains (mainly E. cloacae) showing that cross-transmission plays a major role on their acquisition.
In conclusion, a higher prevalence of fecal carriage of GNB resistant to third GC has been detected. This higher prevalence was associated with a higher ESBLs corresponded to CTX-M-type enzymes and carbapenemases. Our results denote the importance of the intestinal tract as a reservoir for ESBL-producing isolates. The alarmingly high rates of ESBL production and emergence of carbapenemases emphasize the urgent need to develop antimicrobial stewardship initiatives and to maintain antimicrobial resistance surveillance systems. Screening on admission allows early detection and limits dissemination of these strains with application of appropriate control measures.
Footnotes
Acknowledgment
This study was financially supported by the Ministry of Scientific Research Technology and Competence Development of Tunisia.
Disclosure Statement
No competing financial interests exist.