
Abstract
Acinetobacter baumannii is a major threat to public health due to the emergence and dissemination of antibiotic-resistant strains. The purpose of this study was to determine the molecular epidemiology of antibiotic-resistant A. baumannii isolates collected from four tertiary hospitals in Thailand during the period November 2013–February 2015. We screened 339 A. baumannii, nonrepetitive clinical isolates to determine drug susceptibility. Among all isolates, we found that 7.9% was nondrug-resistant A. baumannii (NR-AB). Carbapenem-resistant A. baumannii (CR-AB) strains accounted for 84.9% of the total isolates, with extensively drug-resistant A. baumannii (XDR-AB) accounting for 7.9% of the total isolates. We further investigated class D carbapenemase genes using multiplex-PCR amplification and class B metallo-β-lactamase genes, including blaIMP, blaVIM, and blaNDM-1 genes, using PCR and sequencing methods. We found that 300 (88.5%) isolates carried acquired class D carbapenemase genes, including blaOXA-23 (82.6%), blaOXA-24 (0.3%), and blaOXA-58 (6.5%). The genes blaIMP and blaVIM were not detected in any isolates. The blaNDM-1 was detected in 31 isolates from two hospitals (9.1%). All of the blaNDM-1-positive A. baumannii (NDM-AB) had ISAba125 sequences upstream of the blaNDM-1 gene. A coexistence of three resistance genes—blaOXA-23-blaOXA-58-blaNDM-1—was found in one isolate. A repetitive element palindromic-PCR (REP-PCR) revealed that all A. baumannii isolates were genetically diverse and could be divided into 33 genotypes. Only three genotypes were found to be predominant in all hospitals. Data from our study indicate the widespread emergence of multiple resistance determinants in A. baumannii isolates in Thailand, suggesting the need for more stringent infection control measures.
Introduction
A
MBLs have potent carbapenemase activity which resists β-lactamase inhibitors but is susceptible to inhibition by metal ion chelators. 2 Since the 1990s, several MBLs encoded by mobile DNA elements have emerged in A. baumannii in many countries, of which blaNDM-1, a novel type of MBL, is a major concern. New Delhi Metallo-beta-lactamase-1 (NDM-1) producing bacteria were first reported in 2009. 3 Since then, there have been many reports of blaNDM-1-positive bacteria disseminated worldwide. 4 The first identification of NDM-1-producing bacteria in Thailand have been detected in Escherichia coli, Klebsiella pneumoniae, and Citrobacter freundii but not found in any Acinetobacter spp. 5 Class D carbapenemases are encoded by acquired antibiotic resistance genes blaOXA-23, blaOXA-24, and blaOXA-58, as well as intrinsic blaOXA-51.6,7 These genes are chromosomally encoded or carried on plasmids. 6 The most commonly acquired class D carbapenemase genes in Asia is blaOXA-23, which is highly disseminated among A. baumannii in Thailand.8,9
A. baumannii is the leading cause of nosocomial pathogen in Thailand, but the genes essential for antibiotic resistance remain largely unknown. The need to conduct an epidemiology survey to identify the genetic mechanisms of antibiotic resistance remains. Thus, in this study, our objective was to determine the prevalence of class B MBLs and class D carbapenemase genes in A. baumannii isolates, from four tertiary hospitals in Thailand.
Materials and Methods
Bacterial isolates and geographic characteristics of hospitals
A total of 339 samples were collected from the inpatient units of four tertiary hospitals in Thailand during the period November 2013–February 2015. The specimens were isolated from the outpatient department (OPD) and various hospital wards, including Medicine, Intensive Care Units (ICUs), Surgery, Monk, Very Important Person, Pediatrics, and Trauma. For the purpose of our analysis and discussion, the four hospitals are designated as HA, HB, HC, and HD (Table 1). HC is located in a tourism region and border area of Thailand, and HD is surrounded by a cluster of industrial factories with a substantial population of transient foreign workers. Standard biochemical tests were carried out on the samples collected from the hospitals to identify A. baumannii, and this was confirmed by the PCR method to detect the 16S rRNA gene and the intrinsic blaOXA-51 gene.7,10,11 A. baumannii ATCC 19606 was used as control.
ICU, intensive care unit; OPD, outpatient department; VIP, very important person; REP, repetitive element palindromic.
Antimicrobial susceptibility testing
The antibiotic susceptibility of all the isolates was determined using the disc diffusion method. The results were interpreted according to Clinical and Laboratory Standards Institute guidelines.12,13 Disc diffusion tests were performed with the following 15 antibiotics (Oxoid, Basingstoke, England): amikacin (30 μg), cefepime (30 μg), cefotaxime (30 μg), cefoperazone/sulbactam (105 μg), ceftazidime (30 μg), ceftriaxone (30 μg), ciprofloxacin (5 μg), colistin (10 μg), gentamicin (10 μg), imipenem (10 μg), meropenem (10 μg), piperacillin/tazobactam (100/10 μg), tetracycline (30 μg), tigecycline (15 μg), and trimethoprim/sulfamethoxazole (1.25/23.75 μg). Multidrug-resistant A. baumannii (MDR-AB), CR-AB, and XDR-AB were classified as previously described by Magiorakos et al. 14
Detection of antibiotic resistance genes
DNA was extracted from all isolates and subjected to multiplex PCR to detect blaOXA-23, blaOXA-24, blaOXA-58, and intrinsic blaOXA-51 genes. 7 PCR was used to screen for MBL genes: blaIMP, blaVIM, and blaNDM-1. 15 The ISAba125 of blaNDM-1 gene was determined in all blaNDM-1 positive strains using PCR with a primer pair (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/mdr) designed by the Primer-BLAST program (www.ncbi.nlm.nih.gov/tools/primer-blast). The blaNDM-1 gene from Acinetobacter lwoffii strain WJ10621 plasmid pNDM-BJ01 (GenBank Accession No. JQ001791) was used as a control. An upstream of the ISAba125 was determined using primers ISA125-F/blaNDM-R (Supplementary Table S1). PCR products of the blaNDM-1 genes were purified and sequenced. BLAST was used to compare the sequences of blaNDM-1 genes against the GenBank database (https://blast.ncbi.nlm.nih.gov BLAST). All PCR products were analyzed by electrophoresis in 1% agarose gel containing 0.5 μg/ml ethidium bromide.
MBL production
All metallo-β-lactamase positives found by PCR were further analyzed for MBL production by the combined disk test. An increased inhibition zone with a diameter of ≥7 mm with imipenem-EDTA disk compared to imipenem disk alone was considered as MBL positive. 16
Repetitive element palindromic-PCR
The genetic diversity among A. baumannii isolates was studied using repetitive element palindromic-PCR (REP-PCR) typing. The REP-PCR analysis was performed in all isolates using the ERIC-2 primers (Supplementary Table S1) according to the minor modification of previous study. 17 The condition of ERIC-2 PCR was one cycle at 95°C for 5 minutes, followed by 45 cycles at 94°C for 1 minute, 45°C for 1 minute, and 72°C for 2 minutes. The REP-PCR was analyzed by the banding patterns. The isolates were assigned to the same REP-PCR type if their patterns differed by fewer than two bands, according to previously defined criteria.17,18 Using REP-PCR, a strain was considered to be “epidemic” when it had one or two predominant genotypes that isolated from various patients in each hospital. In contrast, a strain was considered as “sporadic” when it had many genotypes, and each genotype had a few isolates in each hospital.
Results
Isolation and identification of antibiotic-resistant A. baumannii
A. baumannii isolates were collected from sputum (82.0%), urine (4.1%), pus (9.1%), blood (1.8%), body fluid (pleural fluid, ascitic fluid, and drain) (1.2%), wound (1.2%), and medical devices (0.6%) (Table 1). Most of the A. baumannii isolates in our study were isolated from the medical ward (46.3%) (Table 1). All isolates were positive by PCR for detecting the 16S rRNA gene and the intrinsic blaOXA-51 gene. The antimicrobial susceptibility of all A. baumannii isolates to 15 antibiotics is shown in Fig. 1. Among the 339 isolates, 27 isolates (7.9%) were susceptible to all the antibiotics tested. All isolates were sensitive to colistin and tigecycline. More than 70% of the A. baumannii isolates were resistant to cefotaxime (CTX), ceftazidime (CAZ), ceftriaxone (CRO), and ciprofloxacin (CIP). More than 65% of the A. baumannii isolates were resistant to imipenem and meropenem. The prevalence of MDR-AB from the four hospitals was 90.3%. CR-AB was found in 84.9%, and XDR-AB was found in 7.9%. XDR-AB strains were found in each hospital with the prevalence range of 5.7–12.9%. All XDR-AB were CR-AB (Fig. 2A).
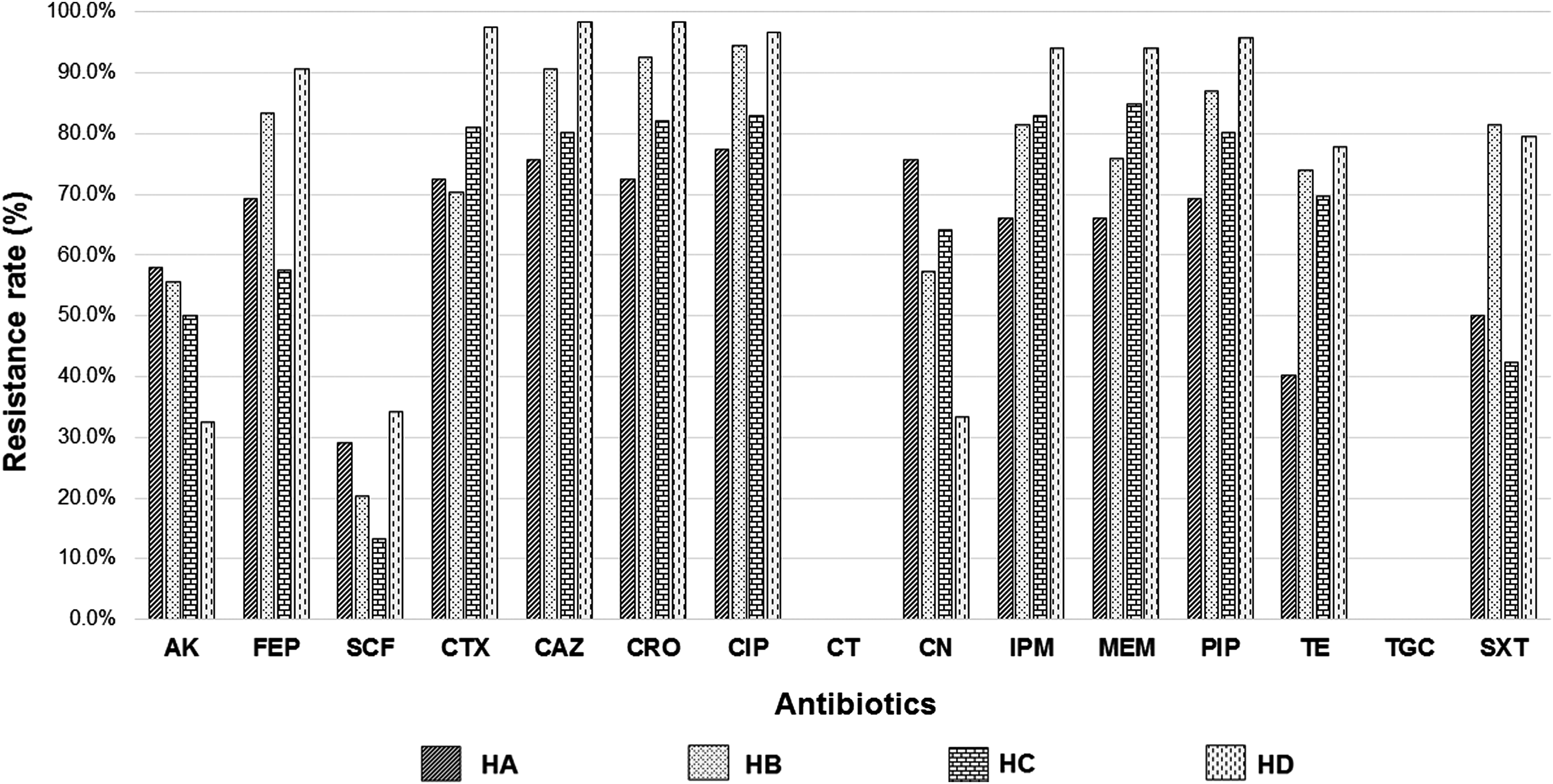
Antibiotic resistance patterns of 339 Acinetobacter baumannii isolates from patients of four hospitals in Thailand. AK, amikacin; FEP, cefepime; SCF, cefoperazone/sulbactam; CTX, cefotaxime; CAZ, ceftazidime; CRO, ceftriaxone, CIP, ciprofloxacin; CT, colistin; CN, gentamicin; IPM, imipenem; MEM, meropenem; PIP, piperacillin/tazobactam; TE, tetracycline; TGC, tigecycline; SXT, trimethoprim/sulfamethoxazole.

Prevalence (%) of MDR-AB, CR-AB, and XDR-AB
Detection of class D carbapenemase and MBL genes
We found high prevalence of blaOXA-23 in all isolates which was 82.6% (280/339). The prevalence of blaOXA-58 and blaOXA-24 was 6.5% (22/339) and 0.3% (1/339), respectively (Supplementary Fig. S1A). The blaOXA-23 gene was detected in 79.1% of the CR-AB strains from the four hospitals, while the blaOXA-24 gene was detected only in HA with a prevalence of 1.6% of all isolates from HA (Fig. 2B). The genes blaIMP and blaVIM were not detected in any isolates. Among the 339 isolates, blaNDM-1 was detected in 31 (9.1%) isolates from two hospitals [2.6% (9/339) HC and 6.5% (22/339) HD]. In all the blaNDM-1 positive strains, ISAba125 was detected upstream of the blaNDM-1 gene (Supplementary Fig. S1B). A coexistence of two resistance genes—blaOXA-23-blaNDM-1—was detected in HC (0.9%) and HD (18.8%) (Fig. 2B). A coexistence between the two pairs of resistance genes blaOXA-23-blaOXA-58 (1.9%) and blaOXA-58-blaNDM-1 (3.8%), and also among the three resistance genes, blaOXA-23-blaOXA-58-blaNDM-1 (0.9%), was found only in HC (Fig. 2B). The MBL production by the combined disk test demonstrated that 100% of 31 isolates of the blaNDM-1 positive strain were MBL-producing isolates.
Epidemiological typing
The fingerprinting represented 33 different DNA patterns consisting of amplicon sizes ranging from 400 to 5,000 bp. The genotype was named R1 to R33 (Table 1). As shown in Fig. 3A, A. baumannii isolates from HA, HC, and HD represented 14, 19, and 13 genotypes, respectively, while isolates from HB could be typed only into six genotypes, which were R4, R6, R11, R12, R14, and R16. We found only three genotypes (R4, R12, R16) distributed in all the four hospitals (Fig. 3A). In this study, we divided A. baumannii isolates into three different groups, which were nondrug-resistant A. baumannii (NR-AB) 27 isolates, NDM-AB 31 isolates, and XDR-AB 27 isolates. One isolate with a phenotype of both NDM-AB and XDR-AB represented genotype R1. REP-typing analysis of three different groups is shown in Fig. 3B. NR-AB isolates belonged to 12 genotypes, while XDR-AB was characterized by only four genotypes. The NDM-AB belonged to five genotypes, which were R1 to R5. REP-PCR genotypes R1 and R4 were presented in all three groups. In addition, A. baumannii blaOXA-23 positive isolates were divided into 26 genotypes. Only one isolate which harbored blaOXA-24 gene was genotype R16. Twenty-two A. baumannii isolates carried the blaOXA-58 gene and had three genotypes, which were R1, R12, and R16.

Genetic diversity using REP-PCR of all Acinetobacter baumannii from Thailand.
Sequencing analysis
The sequences of the blaNDM-1 gene from hospitals HC and HD yielded 100% sequence identity to the blaNDM-1 gene from A. lwoffii strain WJ10621 plasmid pNDM-BJ01 (Accession: JQ001791) obtained from the GenBank database. The nucleotide sequences of the blaNDM-1 genes of the isolates from these two hospitals were similar, and these nucleotide sequences from each hospital were deposited in the GenBank database under the following accession numbers KX447524 and KX495193.
Discussion
A. baumannii infection is a major global concern of nosocomial origin worldwide. In the present study, we confirmed the potential impact of A. baumannii on respiratory infections in Thailand. Eighty-two percent of the specimens were isolated from sputum. This result is consistent with the data of A. baumannii isolates obtained from Hua Hin hospital, Thailand in 2014. 19 The prevalence of CR-AB has been increasing in Thailand and worldwide. Unfortunately, carbapenems, the first antibiotic used to treat the A. baumannii infection, can no longer be used to treat CR-AB, due to its resistance. 20 In our study, we observed that most of the A. baumannii isolates (84.9%) are resistant to the carbapenem antibiotic group, including imipenem and meropenem. High rates of MDR-AB (90.3%) and CR-AB (84.9%) were found in all A. baumannii isolates from all the four hospitals. However, we found lower rates of XDR-AB (5.7–12.9%) than were previously reported in Thailand. 21 Our study also showed that tigecycline and colistin are still effective drugs for the treatment of MDR-AB, since we found no resistance to these antibiotics.
The mechanisms of carbapenem resistance in A. baumannii are mostly associated with class D β-lactamase, 22 but the prevalence of class B MBL in A. baumannii has been increasingly reported in some parts of the world. 1 The blaOXA-58 gene is highly prevalent among A. baumannii isolates in Mexico and Spain.23,24 The first reported presence of this gene in Thailand was in 2013. 25 Subsequent reports from Thailand in 2013 and 2015 indicated the presence of CR-AB, which carries blaOXA-23, blaOXA-24, and blaOXA-58; and further the blaOXA-23 gene was found in 85–100% of A. baumannii isolates.8,9 In our study, we showed that most of MDR-AB and CR-AB harbored the blaOXA-23 gene. The lowest occurrence of blaOXA-24 (1.6%) was found in samples from HA, located in the central part of Thailand. A previous study which analyzed A. baumannii isolates from hospitals in the central region of Thailand found high prevalence (50%) of blaOXA-24 among A. baumannii strains producing MBL. 25
The first identification of New Delhi MBL-1 (blaNDM-1) in Thailand, in 2012, was in Enterobacteriaceae—two isolates of E. coli, two isolates of K. pneumoniae, and two isolates of C. freundii. 5 We identified the blaNDM-1 gene in A. baumannii in two hospitals in Thailand, one located in the northern region and the other in the eastern region. The first hospital HC is located in the northern tourism region and border area adjoining Myanmar and the second hospital HD in eastern Thailand, surrounded by a cluster of industrial factories with many foreign workers. A horizontal gene transfer of antibiotic-resistant genes might occur due to the movement of tourists and foreign workers. 26 The presence of the blaNDM-1 gene was found in 8.5% (9/106) of A. baumannii isolates taken from HC and 18.8% (22/117) of A. baumannii isolates from HD. These results are similar to those from several previous studies, which variously reported that the blaNDM-1 gene was found in 1.7–11.4% of A. baumannii isolates tested during 2013–2014 in Bangladesh, Pakistan, and India.27–29 The blaNDM-1 gene is known to be carried by chromosome and plasmids, which are the major causes of the spread of antibiotic-resistant genes among many bacteria, through horizontal gene transfer.30,31 ISAba125 (IS30 family) has been reported to relate to the acquisition of blaNDM-like genes in A. baumannii. 32 In our study, all of the blaNDM-1 positive isolates were positive for ISAba125. The ISAba125 element, which has been located upstream of the blaNDM-1 gene, is a strong promoter of the expression of this gene. 33 It is possible that ISAba125 may be a vehicle for the dissemination of blaNDM-1 gene in A. baumannii. 29
We found class D β-lactamase genes and blaNDM-1 coexisting in two hospitals in Thailand. This result was similar to previous studies in Japan and Switzerland, which found the coexistence of blaOXA-23 and blaNDM-1 genes.34,35 In addition, the coexistence of blaOXA-58 and blaNDM-1 genes was found in Acinetobacter junii and Acinetobacter pittii.36,37 The coexistence of three resistant genes—blaOXA-23, blaOXA-69, and blaNDM-1—in A. baumannii isolated from rectal swabs was also reported in Switzerland. 38 Furthermore, in the Czech Republic, Krizova et al. found that A. baumannii ANC4097 harbored five genes encoding β-lactamase, including blaNDM-1, blaOXA-23, blaOXA-69, blaTEM-1, and blaAmp-C. 39 In our study, we found only one isolate (0.3%) from HC hospital which was positive for blaOXA-23, blaOXA-58, and blaNDM-1, from a total of 339 A. baumannii isolates taken from four hospitals in Thailand. This study is the first report of blaNDM-1, blaOXA-23, and blaOXA-58 genes in A. baumannii in the same isolates.
The REP-PCR method has previously been used to discriminate A. baumannii isolates worldwide.17,18,40 Our REP-PCR typing revealed a high genetic diversity (R1–R33) among A. baumannii isolates. Our epidemiological study highlighted the fact that most of the isolates belonged to genotype R16 (157/339). This type was the major epidemic strains in HA, HB, and HD. In contrast, we found genotype R16 and genotype R24 as two major epidemic strains in HC. A previous study showed the presence of blaOXA-23 and blaOXA-58 genes in the same major REP-PCR clone of A. baumannii. 40 Our study displayed the blaOXA-23 positive isolates (151/280) in all the four hospitals representing the major genotype, R16. The major REP-PCR typing presented in XDR-AB was genotype R4 (22/27). This strain was epidemic in all XDR-AB from four hospitals. Furthermore, we found that all XDR-AB genotype R4 isolates were positive for the blaOXA-23 gene. Most of A. baumannii harbored blaNDM-1 gene isolates (NDM-AB) collected from HC and HD hospitals were genotype R1 (17/31), and all of NDM-AB genotype R1 were classified as the epidemic strain. In contrast, NR-AB strains had 12 genotypes and each of the genotype had a few isolates. All these strains were considered as sporadic strains.
In conclusion, our study indicated an increase in the prevalence of antibiotic-resistant A. baumannii bacteria. This study indicated the dissemination of class D β-lactamase genes and blaNDM-1 in many regions of Thailand. The blaOXA-23 harbored A. baumannii isolates are found most abundantly. A greater effort for infection control is essential to prevent the dissemination of the A. baumannii harboring class D β-lactamase and blaNDM-1 determinants in hospitals in Thailand.
Footnotes
Acknowledgments
The authors thank staff of four hospitals for providing the A. baumanni isolates. Many thanks to Mr. Roy Morien of the Naresuan University Language Centre for his English editing in this document. This study was funded by Thailand Research Fund (RSA5780015). U.L. was supported by a Graduate student scholarship from Naresuan University. R.T. was supported by The Royal Golden Jubilee PhD Program (PHD/0031/2558).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.