
Abstract
Aims:
The present study aims to evaluate the predominance of uropathogens responsible for urinary tract infection (UTI) and determine their resistance patterns, to assess if the recommended empirical treatment is appropriate for the studied population. Samples were collected in Aveiro (Portugal) from an ambulatory service between June 2011 and June 2014.
Results:
From the 4,270 positive urine samples for UTI, 3,561 (83%) were from women and only 709 (17%) were from men. The bacterium Escherichia coli was the most frequent uropathogen, followed by Klebsiella sp., Enterococcus sp., and Proteus mirabilis. E. coli was also the uropathogen presenting less resistance to antibiotics, including those recommended as first and second line UTI treatment. In general, bacteria isolated from men were more resistant to antimicrobials than bacteria isolated from women.
Conclusions:
The results of this study emphasized the relevance to consider sex as a differentiating factor in the choice of UTI empirical treatment, mainly due to differences in antimicrobial resistance. From the first line drugs recommended by the European Association of Urology (EAU) to empirical treatment of uncomplicated UTI, nitrofurantoin is the most appropriate drug for both sexes. Ciprofloxacin, although appropriate for treatment in women, is not appropriate to treat UTIs in men. From the second line drugs, both trimethoprim–sulfamethoxazole (TMP-SMX) and amoxicillin–clavulanic acid (AMX-CA) are appropriate drugs for treatment of uncomplicated UTI in women, but not as effective for men.
Introduction
U
The diagnosis of asymptomatic bacteriuria is defined by the presence of bacteria in the urine without clinical signs or symptoms suggestive of a UTI. 4
Community-acquired UTIs are mainly uncomplicated, when occurring in nonpregnant young women with a normal genitourinary tract. The bacteria from fecal flora commonly colonize the bladder causing cystitis.5,6 In some cases, bacteria may ascend through the ureters to the kidneys and cause more severe infections such as pyelonephritis.5,6 Moreover, specific subpopulations are more likely to have UTI, such as patients with catheters, urologic abnormalities, diabetes, immunodeficiency, infants, pregnant women, and the elderly. UTI can be more severe in these patients. 7
To reduce the number of therapeutic failures it is quite important to carry out periodic monitoring studies, including the main uropathogens implicated in community-acquired UTI and their respective antimicrobial resistance pattern. 8
Studies realized in the community at an international level have shown that uropathogens such as Escherichia coli (46.4–74.2%), Klebsiella sp. (6.0–13.45%), Proteus sp. (4.7–11.9%), and Enterococcus sp. (5.3–9.54%) are the most prevalent in UTIs.9–18 E. coli has been indicated as the most frequent uropathogen involved in community-acquired UTI, probably because it belongs to the normal flora of the human intestine and therefore is able to colonize the urinary tract.11,14,15,19
According to the European Association of Urology (EAU), the empirical first line treatment recommended for acute uncomplicated UTI (U-UTI) is ciprofloxacin, fosfomycin, and nitrofurantoin. Ampicillin, amoxicillin–clavulanic acid (AMX-CA), and trimethoprim–sulfamethoxazole (TMP-SMX) are indicated as second line treatment by the EAU. The European Society for Microbiology and Infectious Diseases (ESCMID) recommends fosfomycin due to minimal resistance and lower likelihood of side effects 20 as first line therapy for acute U-UTI. Ciprofloxacin is suggested as an effective 3-day regime. However, for treatment in men it should last a period of 10 to 14 days. 21 Nitrofurantoin is also an appropriate choice for therapy due to minimal resistance and low collateral damage. 20
The EAU recommends β-lactam agents for the second line therapy only when the first line agents cannot be used due to their inferior efficacy and more adverse effects. Despite wide diffusion in the international guidelines, the use of TMP-SMX must be based on an antimicrobial susceptibility test (AST) and it should only be prescribed if the local resistance rates of uropathogens do not exceed 20%. 22 According to the Uncomplicated Urinary Tract Infection Guidelines (1999) by the Infection Disease Society of America, amoxicillin (AMX) or ampicillin (AMP) should not be used for empirical treatment given the relatively poor efficacy and the very high rates of resistance to these agents worldwide. 20
The high rates of resistance among pathogenic bacteria suggest the failure of the previous preventive guidelines to slow down the antimicrobial resistance.8,14,23–25 In the absence of regional surveillance community studies, the use of empirical treatment in an early phase of the disease to decrease the rate of morbidity should be guided by national resistance surveillance data.8,24,25 The surveillance should be continuous since the bacterial resistance patterns change over time. To administer an appropriate empirical therapy, it is crucial to know not only the main bacteria usually involved in the UTI but also their respective antibiotic resistance patterns.13,22,26,27 The surveillance procedures control the increase of antimicrobial resistance and the spread of resistant bacterial strains that represent a public health problem worldwide.
The goal of this study is to evaluate the predominance of uropathogens responsible for UTIs and their resistance patterns, in North Aveiro (Portugal) between 2011 and 2014, to assess if the empirical recommended treatment by EAU of UTI is appropriate for this population.
Methods
Data samples
All the samples were collected in the ambulatory system, from outpatients attending family physicians and from daily care institutions, from June 2011 to June 2014 at Centro Médico da Praça Lda, located in São João da Madeira municipality, district of Aveiro in the north-western region of Portugal. The urine cultures were collected from patients presenting clinical manifestations that suggested the presence of a UTI, including urethral pathologies and other diseases that have similar clinical symptoms to UTI. Samples from UTI posttreatment pregnant women and from catheterized patients were also included. Although some patients, such as the elderly or pregnant women, had multiple urine samples, multiple samples from the same patient were not regarded for analysis. Samples with negative urine screenings (dipstick) and with polymorphic bacterial growth were not considered. The positive UTI samples were registered in the database with a code and a process number for each patient. Each process had a profile with name, gender, age, bacterial strain, and the corresponding antimicrobial susceptibility testing (AST) from the VITEK® 2 (bioMérieux SA) report.
Sampling
First morning urine samples (no more than 4 hours storage in bladder) were collected by the patients after their personal hygiene. The first and final urine was rejected; a midstream clean catch urine was collected in a sterile specimen container to avoid contamination. Samples were transported in their primary containers and stored at 4°C until they could be processed. 28 Urine samples from children <2 years of age were collected using a sterile bag that was attached to the skin surrounding the urethral area. The bag was controlled every 15 minutes. After micturition the bagged urine sample was removed, closed, and stored at 4°C until processing.
Microscopic examination
Ten milliliters of urine was transferred from the container to examination tubes and then applied to the dipstick. The samples were tested for nitrite and leukocyte esterase. Then the tube was centrifuged at 1,500 rpm for 5 minutes, and the supernatant was decanted. The pellet was homogenized and mounted on slides that were directly examined or stained by the Gram technique.
Urine culture
One microliter of the urine sample was inoculated with a disposable plastic loop on CLED media or chromID™ CPS® plates (bioMérieux) and incubated at 37°C in aerobic atmosphere for 18 hours. These culture media allow direct presumptive identification of E. coli, Proteus sp., and Enterococcus sp. considering the size, color, and shape of the colony-forming units (CFU). 28 After incubation, all the negative cultures (bacteria growth inferior to 103 CFU/mL) were excluded. If bacterial growth was equal or superior to 105 CFU/mL based on the count of the bacterial colonies, the urine culture was defined as positive. Samples were considered contaminated if three or more different colonies had grown in the culture medium. These samples were rejected and classified as “polymorph flora,” and a second sample was requested from the patient. Bacteriuria was defined when bacterial growth was inferior to 105 CFU/mL. In this case, only the bacterial identification (ID) and the antimicrobial sensibility test (AST) were performed on pregnant women and children.
Identification of bacterial isolates
Identification was performed using the VITEK 2 ID card, after the Gram stain to differentiate bacterial species into Gram positive or Gram negative. The isolates were inoculated in a saline suspension, with a density between 0.5 and 0.65 in McFarland scale. According to the characteristics of the colonies, the VITEK 2 GN ID Card was chosen to identify lactose fermenting and nonfermenting Gram-negative bacilli, or the VITEK 2 GP ID Card to identify Gram-positive bacteria.29,30
Three milliliters of a commercial saline liquid medium (0.45%) was previously prepared for each respective ID card based on the established McFarland Turbidity Standard of 0.5 to 0.63 (±0.1). The tips of VITEK 2 ID Cards were emerged in the saline suspension tubes and taken into the VITEK loading dock. The saline suspensions were introduced into the VITEK 2 ID Cards by vacuum pressure. Then, the completed VITEK 2 ID Cards were removed and placed into the VITEK incubator at 36°C. The results were available within 10 hours.29–31
Antimicrobial susceptibility test
The AST was performed with VITEK 2 AST Card: the VITEK 2 AST-GN26 (the Portuguese card for urine samples); VITEK 2 AST-N113 to Gram-negative bacteria with resistance to the majority of the antibiotics from the VITEK 2 AST-GN26; VITEK 2 AST-P586 to Gram-positive Enterococcus sp. and Streptococcus sp.; and VITEK 2 AST P619 to Gram-positive Staphylococcus sp. 32
Three milliliters of a commercial saline liquid medium (0.45%) was previously added to each AST tube.33,34 From the Gram-negative suspensions, 147 μL of the VITEK ID were diluted into the AST tubes. From Gram-positive suspensions, 270 μL of the VITEK ID suspensions were diluted into the AST tubes. The ID cards and AST card tips were introduced into their respective saline suspensions and taken into the VITEK loading dock. After loading, they were incubated at 36°C in the VITEK incubator for 10 hours.29,31
The AST results were validated by the advanced expert system program, which follows the European committee on antimicrobial susceptibility testing (EUCAST). 35 The phenotypic antimicrobial susceptibility testing determination depends on the minimal inhibitory concentration (MIC) breakpoints. Based on breakpoints, bacteria were grouped into three categories as follows: susceptible, intermediate, and resistant.29,36,37
Statistical analysis
Data were stored in Microsoft Excel, while the statistical treatment was done using the Statistical Package for the Social Sciences (SPSS) 16.0 for Windows. The normality, homogeneity, and independence of the variants were checked before analysis. Since the data failed the normality assumptions, nonparametric methods were used to detect significant differences. Mann–Whitney U test was used to evaluate differences between genders. The Kruskal–Wallis test was used to evaluate the age groups and the influence of the study period in the UTI incidence. The chi-square test was used to evaluate the incidence of isolates by age groups. The significant level established was p ≤ 0.05. The main bacteria responsible for UTI, the bacteria that cause at least 1% of the study infections (representing 93.5% of the total UTIs), were selected so as to simplify the statistical treatment. The main bacteria responsible for UTI, such as E. coli, Enterococcus sp., Klebsiella sp., Proteus mirabilis, Pseudomonas aeruginosa, Staphylococcus sp., and Streptococcus agalactiae, were identified as responsible for at least 1% of the infections under study. The remaining bacteria were grouped and classified as “other bacteria” (representing 6.5% of the total infections), including Acinetobacter baumannii, Burkholderia cepacia, Citrobacter sp., Enterobacter sp., Hafnia alvei, Morganella sp., Proteus sp., Providencia sp., Pseudomonas sp., Raoultella sp., Salmonella enteritidis, Serratia sp., Shigella sp., Sphingomonas paucimobilis, and Yersinia enterocolitica.
Results
Characterization of the patients with bacterial UTI
From the 4,270 positive urine samples, 3,561 (83%) were from women and only 709 (17%) were from men. The age ranged from 0 to 104 years of age with an average age of 61 years. The average age for women was 59 and for men 68. The incidence of UTI increased with age (chi-square, p < 0.05). Hence, the elderly group was the most affected, with 2,219 (52%) positive urine samples, followed by 78.1% of the women and 21.9% of the men (Fig. 1a). However, a decrease of 1% in UTI incidence was observed among children (2.4%, 70.3% were female and 29.7% were male) and adolescents (1.2%, 94.3% were female and 5.7% were male). This decreasing tendency was also observed among children and a group of young male adults (2%) (Fig. 1a). In general, women were the most affected in all age groups (chi-square, p < 0.05) and the incidence of UTI increased with the patient's age (Fig. 1a). The largest gender differences among age groups occurred in adults, young adults, and adolescents (Fig. 1b).
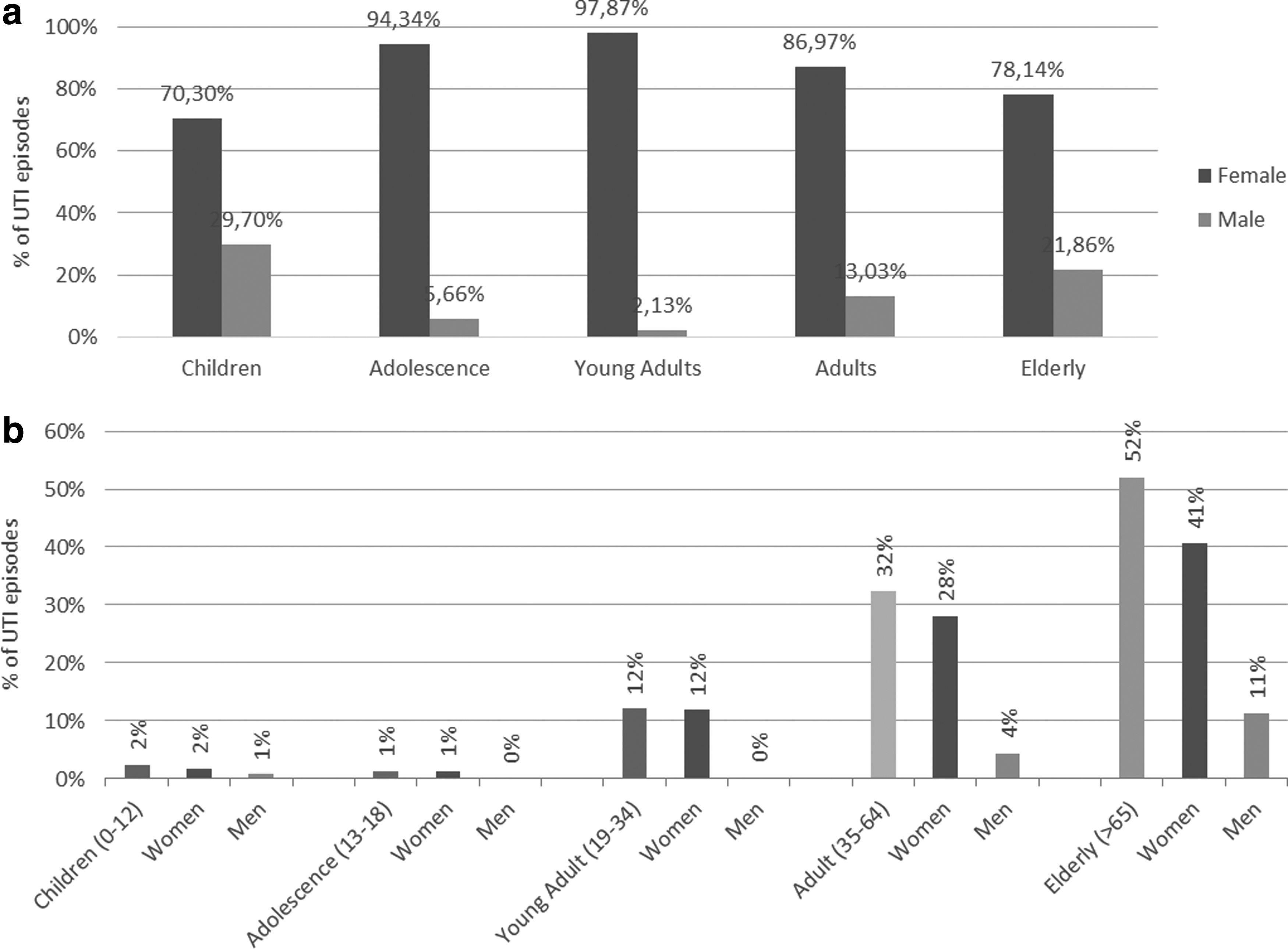
Incidence of the main bacteria implicated in UTI by age groups for both genders considered. Percentage in relation to all UTI episodes (N = 4,270);
Bacteria implicated in UTI
The predominant uropathogen was E. coli (63.8%), followed by Klebsiella spp. (11.8%), Enterococcus sp. (6.8%), P. mirabilis (5.6%), Staphylococcus spp. (2.4%), P. aeruginosa (1.9%), and S. agalactiae (1.2%) (Table 1).
N—frequency of isolates; total %—percentage of isolates in relation to N; women (%)—percentage of isolates in relation to n women; men (%)—percentage of isolates in relation to n men.
The main bacteria implicated in female UTI were statistically different from those implicated in male UTI (Mann–Whitney U test, p < 0.05). The E. coli bacterium was the most implicated in both genders. However, its incidence was higher in women than in men, 67.8% and 43.4%, respectively (Table 2). The incidence of P. aeruginosa was also different among genders, causing more infections in men (5.1%) than in women (1.3%). The same was observed for P. mirabilis, with incidences of 10.7% and 4.6%, respectively, for men and for women (Table 2).
Bold values represent higher than >20%.
AMX-CA, amoxicillin–clavulanic acid; M, men; n total number of resistant bacteria; TMP-SMX, trimethoprim–sulfamethoxazole; W, women.
The analysis of etiology has shown statistically significant differences among age groups (Kruskal–Wallis test, p < 0.05). An increasing incidence of Klebsiella sp. was reported in the age groups. The incidence of P. mirabilis was substantially higher in children compared to the other age groups. There was a higher incidence of Staphylococcus sp. and Enterococcus sp. in adolescents and young adults compared to the other age groups. E. coli was responsible for more than half of the UTI infections in both young adults and adults.
Throughout the study period significant differences were observed in the prevalence of the main bacteria of the UTI (Kruskal–Wallis test, p < 0.05). The incidence of E. coli varied between 60.8% and 66.0% and was always responsible for more than half of the UTI episodes (Fig. 2). The incidence of Klebsiella sp. showed a 3% decrease over the study period (variation 14.8–10.7%). Contrarily, Enterococcus sp. registered a 5.3% increase during the same period (a variation of 4.4–9.7%). The incidence of P. aeruginosa (a variation of 1.7–2.2%), Staphylococcus sp. (a variation of 2.1–2.6%), S. agalactiae (a variation of 0–2.2%), and P. mirabilis (a variation of 4.9–6.6%) was almost constant over the study period (Fig. 2).

Etiology variation of the main bacteria implicated in UTI over the study period. Significant statistical differences were observed between the main bacteria throughout the study period (Kruskal–Wallis test, p < 0.05).
Significant etiologic differences (Mann–Whitney U test, p < 0.05) between genders were observed in 2011 and 2013.
Antimicrobial resistance pattern of the main bacteria implicated in UTI
In this section the focus was given to the antibiotics recommended for the empiric UTI treatment. Nonetheless, the results of all tested antibiotics in positive urine samples, even those not relevant to UTI, such as first and second generation cephalosporins, tetracyclines, and macrolides, were also shown. In this way, it will be possible to compare the results obtained in this study with those obtained in future studies, namely looking at changes in antibiotics recommended for UTI treatment.
Antibiotics which the studied bacteria were intrinsically resistant to were not considered, namely: the ampicillin resistance for Klebsiella pneumoniae and Klebsiella oxytoca, the nitrofurantoin resistance for P. mirabilis and the TMP-SMX, penicillins, fosfomycin, nitrofurantoin, first and second generation cephalosporins, and cefixime and cefotaxime resistance for P. aeruginosa.
Considering the drugs recommended by the EAU, Gram-negative bacteria presented resistance to fosfomycin, nitrofurantoin, and TMP-SMX, reaching values higher than 20% (Table 2). E. coli showed highest resistance to ampicillin (47.9%); this bacterium also showed high resistance to TMP-SMX (25.1%) when isolated from men. Klebsiella sp. presented the highest resistance to fosfomycin (51.5%), but resistance to nitrofurantoin (28.9%), ciprofloxacin (25.3%), and TMP-SMX (24%) was also high. P. mirabilis presented the highest resistance to ampicillin (48.1%), presenting also high resistance to TMP-SMX (39.3%), fosfomycin (34.9%), and ciprofloxacin (30.4%).
With respect to other antibiotics not as relevant in the treatment of UTIs, the Gram-negative bacteria presented high resistance to first and second generation cephalosporins (Table 2). Klebsiella sp. presented high resistance to first (22.9–23.1%) and second generation (25.3%) cephalosporins. P. mirabilis presented high resistance to imipenem (40.9%) and P. aeruginosa showed a high rate of resistance to ertapenem (60%) (Table 2).
Considering the drugs recommended by the EAU, Gram-positive bacteria presented the highest resistance to fosfomycin. Enterococcus sp. presented high rates of resistance to fosfomycin (100%) and TMP-SMX (94.8%). Staphylococcus sp. showed high resistance to fosfomycin (80.0%) and ampicillin (28.6%). S. agalactiae showed high resistance to ciprofloxacin (100%) (Table 2).
With respect to other antibiotics not commonly used in UTI treatment, Gram-positive bacteria also presented high resistance to several drugs. Enterococcus sp. presented high rates of resistance to second generation cephalosporins (94.4%), clindamycin (92.7%), and tetracycline (80.9%). Staphylococcus sp. showed high resistance to carbapenems (83.9–100%) and second generation (82.5–85.7%) and third generation cephalosporins (60–100%). S. agalactiae showed high resistance to tetracycline (87.8%), clindamycin (51.1%), and erythromycin (46%) (Table 2).
The resistance presented by bacteria implicated in UTI was statistically different (Mann–Whitney U test, p < 0.05) between genders. E. coli, Klebsiella sp., P. mirabilis, and Staphylococcus sp., showed higher resistant rates when isolated from male patients than from female (Table 2).
As far as the isolates from both genders are concerned, on average the isolates from women were resistant to two antimicrobials from distinct antimicrobial classes of drugs. However, for the most part the isolates from men were resistant to five antimicrobials belonging to four antimicrobial classes of drugs.
Although the resistance of E. coli has remained constant throughout the study period to the tested antimicrobials (Fig. 3b), the resistance of the other bacteria changed significantly over the study period (Kruskal–Wallis test, p < 0.05) (Fig. 3a, b). Considering the drugs recommended by the EAU, the resistance to penicillin decreased. Furthermore, there was a decrease in other antibiotics, namely concerning second and third generation cephalosporins, lincosamides, fosfomycins, carbapenems, and macrolides. However, S. agalactiae registered an increase in resistance to the tetracyclines, glycopeptides, lincosamides, and macrolides over the study period (Fig. 3a).
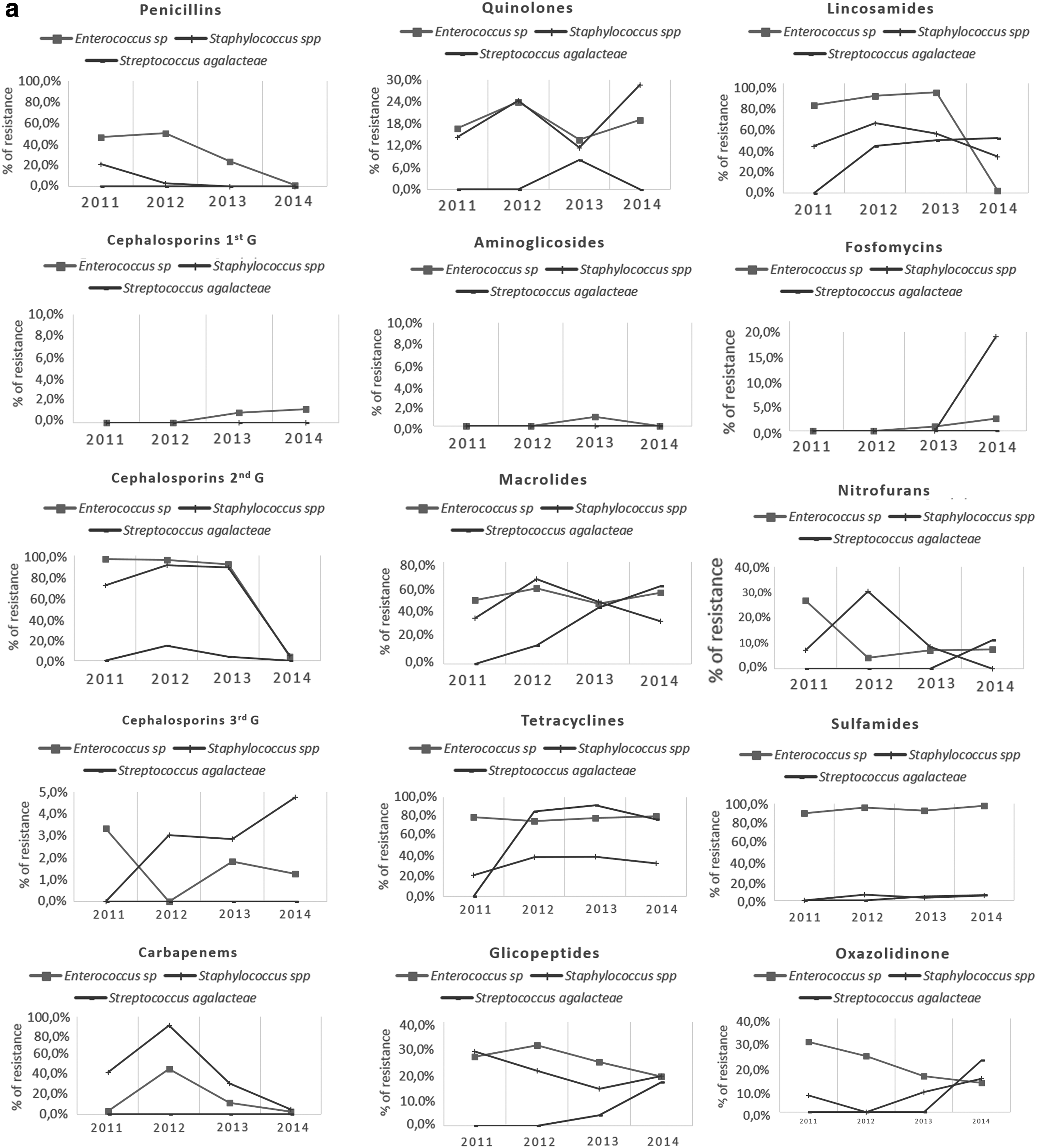
Variation of antimicrobial resistance pattern of bacteria during the study period (2011–2014).
The pattern of bacterial resistance to antibiotics was significantly different among age groups (Kruskal–Wallis test, p < 0.05) (Fig. 1).
The average weighted incidence of UTI was calculated considering that E. coli was responsible for 63.8% of the infections, while the remaining bacteria caused only 36.2% of the infections. The weighted average was calculated through arithmetic average; however, the prevalence of each bacterium was taken into account. The values of antimicrobial resistance of each bacterium were multiplied by its incidence (Table 3).
Bold values represent higher than 20%. First line recommended treatment: CIPRO (%), FOS (%), NITRO (%); second line recommended treatment: AMP (%), TMP-SMX (%), AMX-CA (%); alternative treatment: IMP (%), GEN (%).
The weighted average was calculated through the arithmetic average, but taking into account the incidence of each bacterium. The values of antimicrobial resistance of each bacterium were multiplied by its incidence.
AMP, ampicillin; CIPRO, ciprofloxacin; FOS, fosfomycin; GEN, gentamicin; IMP, imipenem; NITRO, nitrofurantoin; Not considered, natural resistance; INC, incidence; M, men average resistance; T, total average resistance; W, women average resistance.
Considering the first line treatment recommended by EAU, the weighted average incidence of resistance was lowest for nitrofurantoin, but for ciprofloxacin and fosfomycin it was higher than 20%. The weighted resistance for these antibiotics was higher for the bacteria isolated from male patients than those isolated from women (Table 3). The same was observed for antimicrobials recommended as second line treatment by EAU, namely for ampicillin and TMP-SMX (Table 3). AMX-CA presented the lowest weighted average (Table 3).
Discussion
As observed in other studies, E. coli was the most common uropathogen implicated in UTIs covering the population of Aveiro North. E. coli bacterium was responsible for more than half of the UTI (64%). Moreover, Klebsiella sp., P. mirabilis, and Enterococcus sp. were also frequently involved in UTI (6–12%), similar to that observed in other studies performed at community level worldwide.11,14,15,38–41 The high frequency of Enterobacteriaceae and Enterococcus sp. can be an indicative of self-colonization by gastrointestinal pathogens, since these bacteria are very common in gastrointestinal flora and are reported as being largely responsible for R-UTI. 1 Enterobacteriaceae encode a variety of virulence factors that facilitate attachment to host tissues within the urinary tract. 42
UTI was more frequent in women than in men (67.8% and 43.4%, respectively), and the highest difference between female and male patients was observed for P. aeruginosa (an incidence of 5.1%, 3.9 times higher in men) and P. mirabilis (an incidence of 10.7%, 2.3 times higher in men). According to the literature, P. aeruginosa is more frequent in men due to characteristics inherent to the patient, such as sex and age. Furthermore, there is an increased risk for contracting the bacteria in patients who have a previous history of using antimicrobials, undergoing interventions in the urinary tract, and suffering from neurogenic bladder.8,43–45 The higher incidence of P. mirabilis in men than in women is also consistent with published literature. 46 P. mirabilis is a serious medical problem in catheter-associated UTI, due to biofilm production capacity, 47 which explains the greater incidence rate among the elderly. As reported by Nicolle, 48 the elderly age group, especially men, were the most frequent catheter-associated UTI patients. E. coli was the most predominant in both genders; however, its incidence was significantly higher in women (67.8%) than in men (43.4%), which was also observed in other similar studies.8,41
The average age of men with UTI was significantly higher compared with women (average age 68 and 59 years, respectively), which can also explain the etiological differences among genders. The higher incidence of UTI in older men can be due to benign prostate hyperplasia and neurogenic bladder conditions, which are more common at this age,42,44 as well as to increased hospitalizations due to their more advanced age. In fact, the higher incidence of UTI caused by P. aeruginosa, which was preponderant in men, is frequently associated with the hospital environment.44,48 However, hospital-acquired urinary infections caused by P. aeruginosa in community are still uncommon (1.9% in this study). Nonetheless, it should not be ignored, since other community-acquired UTI studies have reported its increasing incidence.8,43,44
The prevalence increases considerably with age in both men and women. The elderly group was the most affected (52%), followed by adults (32%), young adults (12%), children (2%), and adolescents (1%). It is well documented that there is a prevalence of community-acquired UTI that increases with age, affecting both genders in the elderly population.8,41,49 With respect to older women and men, the frequent use of antimicrobials, the increase of surgical urogenital interventions, urinary incontinence, postvoid residual, and frequent hospitalizations explain the increase in UTI.4,38,42,50,51 The relationship between sexual activity, the use of contraceptives, the use of antimicrobials, and pregnancy and UTI has been well established among adults. 38 In adult and elder women, menopause explains the increase of UTI. After menopause the estrogen levels and amount of Lactobacilli decrease making postmenopausal women more susceptible to UTI. 1 This study did not verify the increase of UTIs from children to adolescents who are on the onset of sexual activity contrary to what is stated in the literature.52–54 This can be attributed to the lower number of urine samples collected from adolescents compared to that from children. The incidence of E. coli, responsible for more than half of the UTI isolates, was constant during the study period (a variation of 60.8% to 66.0%). However, Enterococcus sp. registered a 5.3% increase and Klebsiella sp. a 3% decrease. Kuzdan et al. 55 also observed an increase for Enterococcus faecium and a decrease in K. pneumonia incidence in a 3-year study (2008–2010). The more predominant uropathogen, E. coli, presented the lowest antimicrobial resistance compared with the remaining bacteria implicated in UTI. The resistance to the recommended first line three antimicrobials (5.0% nitrofurantoin, 18.7% ciprofloxacin, and 4.7% fosfomycin) indicated by EAU for uncomplicated UTI was low. The E. coli isolates exceed the resistance values of second line drugs recommended by EAU (<20%) for ampicillin and TMP-SMX (31.5% and 25.1%, respectively), but not the value recommended for AMX-CA (11.4%). High resistance to ampicillin and moderate resistance to AMX-CA and SMX have also been reported in other studies for E. coli. 14
The weighted average of resistance was calculated taking into account the incidence and the drug resistance pattern of the most implicated bacteria in UTI. Among the first line choices which cause little collateral damage, nitrofurantoin seems to be the most suitable to be used in the empiric treatment of UTI in the community (weighted average resistance of 10.7%, 20.6%, and 22.5%, respectively, for nitrofurantoin, ciprofloxacin, and fosfomycin). Considering the second line therapy recommended by EAU, AMX-CA is the most appropriate to be used in UTI empiric treatment in the community (weighted average resistance of 17.0% against 43.0% and 29.7%, respectively, for ampicillin and TMP-SMX).
Overall, taking into consideration the resistance of the most implicated bacterium, E. coli, and the weighted values of resistance for all the main bacteria implicated in UTI, the most appropriate antibiotics to treat UTI in the community are nitrofurantoin as first line and AMX-CA as second line. In this study the resistance to fosfomycin, one of the drugs recommended as first line treatment, was higher than that observed in other studies. 56 However, determining the resistance to fosfomycin is challenging. Experts differ on the best approach (MIC strips and disk diffusion vs. agar dilution) to determine the resistance to this drug. 57 In this study, the AST was determined using the commercial platform Vitek. Further studies are necessary to compare the AST results obtained with the Vitek with results of the disk diffusion and agar dilution methods for the same uropathogens. Nevertheless, the resistance of the UTI isolates to fosfomycin and even to ciprofloxacin was near the 20% resistance limit recommended for empiric treatment of UTI.
The antimicrobial resistance results suggest that the choice of empirical antimicrobial therapy should take into account the sex of the patient. On average the uropathogens isolated from men presented resistance to a higher number of antibiotics compared to those isolated from women. These differences were clearly evident for E. coli and Klebsiella sp., namely for the antibiotics ciprofloxacin, AMX-CA, and TMP-SMX. For the remaining bacteria, in general, the difference between women and men was also evident. Overall, the antimicrobials ciprofloxacin, AMX-CA, and TMP-SMX are more suitable to treat female UTI than male UTI. Two recent studies also found differences in antimicrobial resistance among genders. In a recent Portuguese study the fluoroquinolones were found unsuitable to treat men. In addition, in an Indian study, E. coli isolates showed resistance to the majority of antibiotics in men.8,41
The resistance of the main bacteria isolated from young adults and the elderly to the tested antimicrobials showed significant differences. For these two age groups, significant statistical differences were observed for all antimicrobial classes. As observed before in other studies, the resistance tendency increases significantly with age.8,49 The higher rates of resistance in older patients can be due to the more frequent hospitalization of this age group, as a result of the rise of average life expectancy, weak immune system, and recurring infections. It is recognized that hospitalizations increase the transmission of bacterial strains between hospital and community. 2
In general, the resistance of the main bacteria implicated in UTI to the recommended antibiotics to treat UTI, such as quinolones, nitrofurans, sulfamides, was similar during the study period. The resistance to penicillin decreased during the study period. The resistance to the antibiotics not relevant to UTI treatment, such as glycopeptides, aminoglycosides, and oxazolidinones, was also constant throughout the study period. As observed before 8 the resistance of the bacterium most implicated in the UTI, E. coli, was constant throughout the study period to all tested antimicrobials. According to Linhares et al., 8 the pattern of resistance of the main bacteria implicated in UTI also showed significant changes during a 10-year period. However, E. coli did not show significant changes in the resistance to the tested antimicrobials. This can be explained by the fact that E. coli is a self-colonization of the gastrointestinal tract.
The resistance to first and second line therapy is probably the reflection of their misuse and/or overuse. 58 However, Pallett 59 defends that for nitrofurantoin, an agent licensed only for lower UTI treatment, resistance may be developed during treatment. 59 According to the results of this study, carbapenems and gentamicin could be a suitable UTI treatment for both genders. However, both drugs cause renal toxicity, mainly in patients with significant renal impairment, a condition which is more common in the elderly. 58 Moreover, the use of carbapenems would cause increased carbapenem resistance thus creating a big problem. However, carbapenems, with broad spectrum of action and wide diffusion in the body, 58 could be used in only the most severe cases of complicated UTI. Gentamicin, also with a wide spectrum of action, is inappropriate for the lower UTI treatment. It may, on the other hand, be suitable for UTI treatment associated with systematic sepsis. 59 These two drugs involve the inconvenience of parenteral administration and it can be more expensive than those indicated for UTI.
Conclusions
The most prevalent bacteria responsible for UTI were Gram-negative Enterobacteriaceae (E. coli, Klebsiella sp., and P. mirabilis), being that E. coli proved to be responsible for more than half of these infections. However, this bacterium was also the uropathogen that presented less resistance to antibiotics, including those recommended by the EAU as first and second line treatments.
The results of this study emphasized the relevance to consider sex as a differentiating factor in the choice of UTI empirical treatment, mainly due to differences in antimicrobial resistance. From the first line drugs recommended by the EAU to empirical treatment of uncomplicated UTI, nitrofurantoin is the most appropriate drug for both sexes. Ciprofloxacin, although appropriate for female treatment, would not be appropriate to treat UTI in men. With respect to second line drugs, both TNP-SMX and AMX-CA are appropriate drugs for empirical treatment of uncomplicated UTI in women, but would not be appropriate for men. As alternatives to first and second line recommended treatment, imipenem and gentamicin could be used in the most severe cases such as in UTI associated with systemic infection.
Footnotes
Acknowledgments
Thanks are due to the University of Aveiro, Centre for Environmental and Marine Studies (CESAM) for funding the Microbiology Research Group and to the clinical analysis laboratory Centro Médico da Praça Lda. for supplying the data.
Ethical Conduct of Research
This study was approved by the Ethics Committee of the Clinical Analysis Laboratory Centro Médico da Praça Lda.
Disclosure Statement
No competing financial interests exist.