
Abstract
The spread of carbapenem-resistant Klebsiella pneumoniae (CRKp) has become a significant problem worldwide; however, relevant data in children are limited. We performed a retrospective study to better understand the epidemiology of CRKp bloodstream infections at Beijing Children's Hospital. A total of 164 K. pneumoniae strains were collected from blood cultures between January 2011 and September 2014, of which 52 (31.7%) were CRKp strains. All 52 CRKp strains were multidrug resistant; 46 (88.5%) and 49 (94.2%) isolates were resistant to meropenem and imipenem, respectively. Low rates of resistance to amikacin (5.8%), levofloxacin (7.7%), and ciprofloxacin (15.4%) were observed. All isolates were susceptible to colistin. Among the tested carbapenem resistance genes, the predominant gene was blaNDM-1, detected in 28 (53.8%) isolates, followed by blaIMP-4 (19, 36.5%) and blaKPC-2 (4, 7.7%). Multilocus sequence typing identified 31 sequence types (STs), the most predominant of which was ST782 (9, 29.0%). All ST782 strains were New Delhi metallo-β-lactamase-1 (NDM-1) producing. Four novel STs (ST2010, ST2011, ST2012, and ST2013) and two novel alleles (phoE243 and tonB324) were also detected. Hematologic disease was the most common underlying disease (73.1%). All children received initial empirical therapy. A total of 59.6% (31/52) patients received inappropriate empirical therapy, and 45.2% (14/31) changed antimicrobial therapy after blood culture results were obtained. The overall mortality rate was 11.5%. In conclusion, we observed a high rate of CRKp isolates collected from blood cultures and the predominance of NDM-1-producing K. pneumoniae among children from 2011 to 2014.
Introduction
K
The principal types of carbapenem resistance genes in China are KPC-2 and IMP-4.14,15 New Delhi metallo-β-lactamase-1 (NDM-1)-producing CRKp has rarely been reported in China in the past. However, a series of recent studies detected several outbreaks of NDM-1-producing CRKp infections in neonatal wards in China.16–18 These observations suggested NDM-1-producing CRKp is spreading in China, particularly among children. Thus, we conducted this study to investigate the molecular epidemiology and clinical characteristics of bloodstream infections (BSIs) due to CRKp at a tertiary pediatric hospital in China.
Materials and Methods
Bacterial isolates and patients
K. pneumoniae strains were collected from blood cultures obtained from unique children admitted to Beijing Children's Hospital (a 970-bed tertiary pediatric hospital in China) from January 2011 to September 2014. The VITEK 2 system (bioMérieux) and/or the Phoenix100 automated system (Becton Dickinson) were used to identify bacterial strains. CRKp was defined as an imipenem or meropenem minimal inhibition concentration (MIC) of ≥2 μg/ml. Only the first episode of CRKp-associated BSI was included. Medical records were reviewed, and information regarding demographics, antimicrobial treatment, and clinical outcomes was collected. Inappropriate empirical antibiotic treatment was defined as treatment with no in vitro active drugs on the day of blood culture collection.
Antimicrobial susceptibility testing
The MIC values for 15 antimicrobial agents were determined using an automated broth microdilution method (Becton Dickinson). Escherichia coli ATCC 25922 and K. pneumoniae ATCC BAA-1705 were used as quality control strains. The Clinical and Laboratory Standards Institute 2014 criteria for MICs were applied to classify isolates as susceptible, intermediate, or resistant. 19 For colistin, the results were interpreted in accordance with the European Committee on Antimicrobial Susceptibility Testing clinical breakpoints (version 6.0). Data were analyzed using WHONET 5.6 software recommended by the World Health Organization.
Polymerase chain reaction assays and DNA sequencing of carbapenem resistance genes
Polymerase chain reaction (PCR) was performed using a PTC-100-type PCR instrument (MJ Research, Inc.) to detect carbapenem-resistant genes. PCR primers were designed according to previous studies.20–23 The following carbapenem resistance genes were examined: blaKPC, blaGES, blaIMI/NMC-A, blaSME, blaIMP, blaVIM, blaGIM, blaSPM, blaSIM, blaNDM-1, and blaOXA (OXA-48 and OXA-181). The reaction system (total volume, 50 μl) was set up using a PCR master mix that contained 10 × PCR buffer, 3 mmol/L Mg2+, 4.0 μl of dNTPs, and 0.4 μl of Taq DNA polymerase. The following reaction conditions were applied: predenaturation at 95°C for 2 min, followed by 30 amplification cycles of 95°C for 1 min, 55°C for 1 min, and 72°C for 2 min, with a final extension step of 72°C for 5 min. PCR products were sequenced on an ABI PRISMTM377 DNA sequencer (PE, Inc.). DNA sequences were analyzed and compared using the BLAST program (http://ncbi.nlm.nih.gov/blast).
Multilocus sequence typing
Relationships were determined by performing multilocus sequence typing (MLST). Standard primers (http://bigsdb.web.pasteur.fr/klebsiella/primers_used.html) were used to amplify seven housekeeping genes (rpoB, gapA, mdh, pgi, phoE, infB, and tonB) according to established protocols (http://bigsdb.web.pasteur.fr/klebsiella/klebsiella.html). Alleles and sequence types (STs) are available on the MLST online database. Novel alleles and STs were submitted to the administrator of the database and assigned new designations. Clonal complexes composed of related STs were analyzed using eBURST software (http://eburst.mlst.net). 24
Results
Clinical characteristics of the patients
During the study period, 164 patients with BSIs due to K. pneumoniae were observed, of which 52 (31.7%) were caused by CRKp strains. The median age was 4.3 years (range: 3 hours to 16 years), and 67.3% were male. The majority of the patients with CRKp (41/52, 78.8%) were hospitalized in the hematology/oncology ward. Hematologic disease was the most common underlying disease (38/52, 73.1%), followed by congenital heart disease (3/52, 5.8%) and neuroblastoma (2/52, 3.8%). Almost all patients (40/41, 97.6%) from the hematology/oncology ward exhibited chemotherapy-induced febrile neutropenia when BSI occurred. The majority of the CRKp patients (38/52, 73.1%) had an intravascular catheter. The baseline clinical characteristics of the study population are presented in Table 1.
Antimicrobial susceptibility patterns of CRKp isolates
The antimicrobial susceptibility profiles of the CRKp isolates are listed in Table 2. Almost all isolates were resistant to cephalosporin and β-lactam/β-lactamase inhibitor combinations. Only 9.6% of strains remained susceptible to aztreonam. The rates of resistance to meropenem and imipenem were 88.5% and 94.2%, respectively. Low rates of resistance to amikacin (5.8%), levofloxacin (7.7%), and ciprofloxacin (15.4%) were observed. All isolates were susceptible to colistin (100%).
Detection of carbapenem resistance genes
blaNDM-1, blaIMP-4, and blaKPC-2 were detected in 53.8% (28/52), 36.5% (19/52), and 7.7% (4/52) of the isolates, respectively; no carbapenemase gene was identified in the remaining isolate. The predominant gene was blaNDM-1, and the proportions of blaNDM-1-carrying isolates in 2011, 2012, 2013, and 2014 were 0% (0/7), 30.0% (3/10), 62.5% (10/16), and 78.9% (15/19), respectively. blaIMP-4-carrying isolates accounted for high proportions of the total isolates in 2011 and 2012 (100.0% [7/7] and 60.0% [6/10], respectively), but we observed a decrease in 2013 and 2014 (25.0% [4/16] and 10.5% [2/19], respectively). blaKPC-2-carrying isolates were first detected in 2013, and the rates were 12.5% (2/16) and 10.5% (2/19) in 2013 and 2014, respectively. The distribution of CRKp isolates between 2011 and 2014 is shown in Fig. 1.
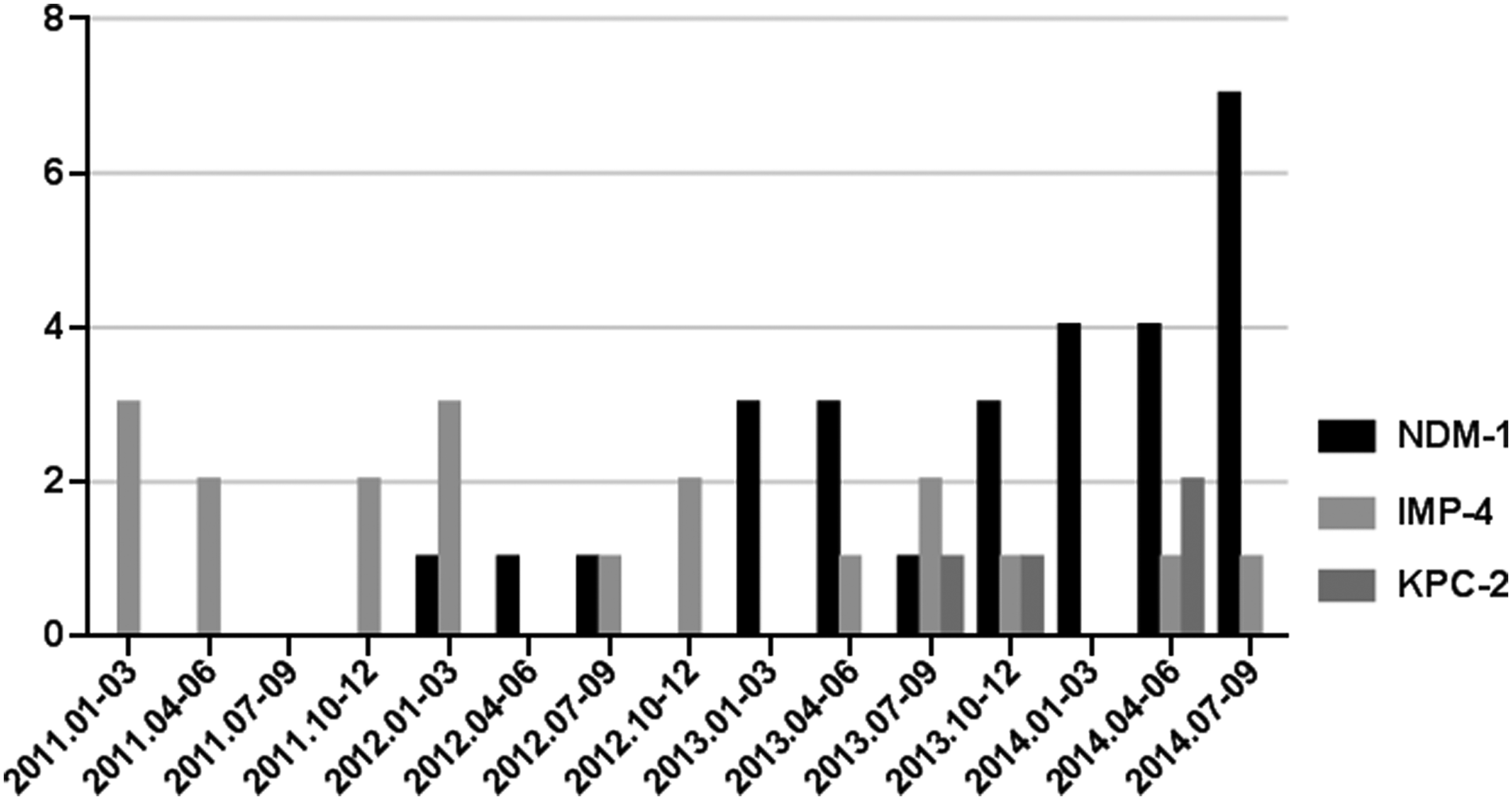
The distribution of CRKp isolates between January 2011 and September 2014. CRKp, carbapenem-resistant Klebsiella pneumoniae.
MLST analysis of CRKp isolates and the identification of clonal complexes
Among the 52 CRKp isolates, 31 different STs were identified by MLST. These 31 STs were further separated using eBURST software into one clonal complex (including ST11 and ST1326) and 29 singletons (Fig. 2). Four of the 31 STs had not been identified previously; they were submitted to the curator and designated ST2010, ST2011, ST2012, and ST2013. Two novel alleles (phoE243 and tonB324) were detected in ST2010 and ST2013, respectively. The predominant ST was ST782 (9/31) followed by ST107 (4/31); ST307, ST571, ST896 (3/31 each); and ST48, ST54, ST1767, ST2012 (2/31 each). The remaining 22 STs were found in single isolates. Of the 31 STs, ST896, ST292, and ST17 were the putative founders of clonal complexes; ST11 possessed a single locus variant (tonB) derived from ST1326. Among the NDM-1-, IMP-4-, and KPC-2-producing isolates, 15, 14, and 4 different STs were identified, respectively. A cluster of nine isolates of clone ST782 were identified in the hematology ward between January and September 2014, and these strains all harbored the blaNDM-1 gene.

Comparative eBURST diagram. This diagram showed the population snapshot of 52 CRKp isolates compared with all STs presented in the multilocus sequence typing database (http://eburst.mlst.net/v3/enter_data/comparative/mlst/default.asp). Each point represents a single ST, the black lines connect single-locus variants. The STs identified in the study are given ST numbers. The size of a point is related to the number of isolates. STs found in both data sets are marked with a box, and those only found in query data set are marked with a circle. The putative founders of each clonal complex are indicated by arrows. ST, sequence type.
Treatment and outcomes
Initial empirical therapy was given to all children. Based on in vitro susceptibility testing results, 59.6% (31/52) of the patients received inappropriate empirical treatment. Of these patients, 45.2% (14/31) changed to active drugs after blood culture susceptibility results were available. A total of 35 (67.3%) children received antimicrobial therapy that included one or two active drugs (meropenem, ciprofloxacin, levofloxacin, and amikacin) after blood culture results were obtained. Antimicrobial treatment modalities and outcomes are presented in Fig. 3. The overall mortality rate was 11.5% (6/52). Of the patients who received inappropriate empirical treatment, four patients (4/31, 12.9%) died (two came from a surgical ward; the others came from a hematology ward).

Antibiotic therapy and outcome for patients with CRKp bloodstream infections. AMK, amikacin; MEM, meropenem; AMC, amoxicillin/clavulanic acid; SCF, cefoperazone/sulbactam; LVX, levofloxacin; FEP, cefepime; CRO, ceftriaxone; MOX, latamoxef; MXF, moxifloxacin; TZP, piperacillin/tazobactam; PEN, penicillin; ZOX, ceftizoxime; CIP, ciprofloxacin. aIncluding meropenem, imipenem, and ertapenem. *The number of antibiotic agents patients received as empirical therapy (including in vitro active drugs and nonactive drugs).
Discussion
During the last decade, there has been a worldwide spread of CRKp.1,2 In China, CRKp has become endemic in many hospitals. 13 In addition, several recent studies suggested the spread of NDM-1-producing CRKp in China, particularly among children.16–18 In this study, we report a high prevalence (31.7%, 52/164) of CRKp isolates collected from blood cultures and the predominance of NDM-1-producing K. pneumoniae among children.
Xu et al. reported an overall prevalence of 5.5% for CRKp strains among blood-origin isolates in 2013 in China, with the highest prevalence of CRKp (20.9%) occurring in the newborn and pediatric group. 13 The rate of CRKp isolates was higher in our study than in Xu's report, revealing a high prevalence of CRKp in our hospital and highlighting the urgent need for enhanced control measures. In China, KPC-2-producing CRKp contributes to the majority of infections among adults.25–27 Our study revealed NDM-1, detected in more than 50.0% of isolates, to be the predominant carbapenemase among pediatric patients. An NDM-1-producing K. pneumoniae clinical isolate was first detected on the tip of a central venous catheter removed from a young male patient in Nanchang in September 2011. 28 Several studies have reported outbreaks of NDM-1-producing K. pneumoniae in different regions of China since the initial report, and most of these outbreaks occurred in neonates and children.16–18 Jin et al. reported outbreaks of NDM-1-producing K. pneumoniae at a neonate unit in Shandong province in 2012 and 201317; similarly, Zhu et al. documented an outbreak caused by NDM-1-producing K. pneumoniae among neonates in Shanghai Children's Hospital between March and June in 2014, for which 77.3% of isolates were blaNDM-1 positive. 18 Wang et al. reviewed articles published from 2010 until 2015 and found that blaNDM-1-positive bacteria were more commonly collected from pediatric departments in China. 29 Thus, based on the results of our study and these reports, we suggest that NDM-1-producing K. pneumoniae infections are more common among children in China.
MLST results indicated our isolates are genetically diverse; several ST clones (such as ST307, ST22, and ST17)17,30 identified in our study have been responsible for CRKp epidemics in other regions, revealing the potential dissemination of carbapenemase genes among different K. pneumoniae clones. 31 The most predominant ST in our study was ST782, which is a two-locus variant (infB, mdh) of ST14; notably, ST14 was the most common NDM-1-positive clone. 32
The majority of BSIs occurred in a hematology ward, particularly among patients experiencing chemotherapy-induced neutropenia. Chemotherapy destroys the continuum of the mucosal barrier and predisposes a patient to BSI, which may help explain this phenomenon. 33 Furthermore, exposure to healthcare environments, antibiotic therapy, and immunocompromised status poses increased risks of infection to patients with hematologic diseases. 34 As shown in other studies, indwelling devices and the extensive presence of comorbidities are risk factors for BSIs. 11 In our study, the majority of patients received an intravascular catheter, and almost all patients displayed one or more comorbidities. Thus, for patients who have risk factors, further surveillance and strict infection control measures are urgently needed to prevent the expanded spread of CRKp.
In our study, almost all strains were resistant to cephalosporin, β-lactam/β-lactamase inhibitor combinations, and meropenem/imipenem, while the majority of strains were susceptible to ciprofloxacin, levofloxacin, and amikacin. Children who received these three drugs had a relatively favorable outcome. However, in China, these agents are not recommended for use in children due to their nephrotoxicity and ototoxicity. Several studies have revealed poor outcomes in CRKp BSIs associated with inappropriate empirical antibiotic treatment,35,36 and a recent study conducted in hematological patients also indicated that inappropriate empirical antibiotic treatment is the only independent risk factor for mortality. 37 However, we were unable to demonstrate a significant association between inappropriate antibiotic treatment and poor outcome in this study. The overall mortality rate in our study was 11.5%, which is lower than the rate reported by Diaz et al., 38 possibly due to underlying debilitating conditions or other contributing factors.
Our study had several limitations. First, it is a single-center study, and the prevalence and molecular characteristics of CRKp in our pediatric patients may not be generalizable to pediatric patients in our country; however, our study included a relatively large pediatric cohort of CRKp BSIs, and the patients came from all over the country. In addition, we did not assess tigecycline MICs. Furthermore, our data were unable to confirm evolutionary relationships between isolates.
Conclusion
We observed a high rate of CRKp isolates collected from blood cultures between January 2011 and September 2014, and NDM-1-producing K. pneumoniae predominated in BSIs among children. The dissemination of CRKp and its limited therapeutic options highlight the urgent need for further surveillance and strict infection control measures, particularly for immunocompromised patients.
Footnotes
Acknowledgments
Ethics Approval
The protocol was approved by the Ethics Committee of Beijing Children's Hospital, Capital Medical University. Informed consent was waived because we used strains that already existed, and we did not cause injury to patients.
Disclosure Statement
No competing financial interests exist.