
Abstract
The increasing use of chlorhexidine for methicillin-resistant Staphylococcus aureus (MRSA) decolonization has raised concerns about the emergence of resistance to or tolerance of this antiseptic. We examined the frequency and characteristics of qacA/B chlorhexidine tolerance genes among MRSA isolates in a surgical intensive care unit (ICU) where MRSA-colonized patients are decolonized by chlorhexidine bathing. The MRSA isolates were evaluated for chlorhexidine susceptibility, mupirocin resistance, molecular typing, agr functionality, and the heterogeneous vancomycin-intermediate S. aureus (hVISA) phenotype according to the presence of the qacA/B genes. Overall, 119 MRSA isolates were obtained from active surveillance cultures (93, 78.2%) and clinical cultures (26, 21.8%) between 2012 and 2014. Among these isolates, 39 (32.8%) carried the qacA/B genes, and 23 (19.3%) exhibited mupirocin resistance. Most qacA/B-positive isolates (36/39, 92.3%) were identified as ST5-SCCmecII (69.2%) and ST239-SCCmecIII (23.1%), which are common healthcare-associated (HA)-MRSA strains in Korea. Multivariate analysis found that qacA/B-positive MRSA isolates were associated with agr dysfunction (OR, 4.87; 95% CI, 1.71–13.87) and the hVISA phenotype (OR, 4.09; 95% CI, 1.48–11.34). In conclusion, our study showed that qacA/B carriage was common among MRSA isolates in an ICU where chlorhexidine is commonly used for decolonization. qacA/B carriage was significantly associated with agr dysfunction and the hVISA phenotype. These features may confer a selective advantage on HA-MRSA strains, including ST5-SCCmecII and ST239-SCCmecIII, in the ICU setting.
Introduction
D
The qacA/B genes are located mainly on plasmids and may be related to additional antibiotic resistance genes, which may contribute to a survival advantage under chlorhexidine selection pressure. 7 Although some studies have shown that these genes might contribute to the increasing prevalence of ST239 and CC22 clones, a recent U.S. study did not demonstrate such clonal dominance.8–10 In this context, additional data on the prevalence of qacA/B genes among different MRSA strains or their impact on clinical outcome in the setting of chlorhexidine-based decolonization are needed. In this study, we characterize the molecular epidemiology of qacA/B-positive MRSA isolates and correlate these isolates with clinical significance.
Methods
Study setting, infection control programs, and data collection
This retrospective study was conducted at a 14-bed surgical ICU at Gyeongsang National University Hospital (GNUH), an 890-bed community-based tertiary hospital in Jinju, South Korea, between December 2012 and December 2014. The GNUH Institutional Review Board approved this study.
All patients admitted to the ICU had nasal swabs collected to carry out MRSA active surveillance cultures (ASCs). ASCs were performed twice per week and at ICU discharge for patients who stayed 48 hr or longer. All patients identified as MRSA positive were managed with contact precautions and isolation in single rooms or cohorted areas. Decolonization of MRSA carriers was introduced in December 2012 and consisted of whole-body bathing using washcloths soaked in 2% chlorhexidine gluconate solution and intranasal mupirocin for 5 days. Clinical data were reviewed for patients whose MRSA isolates were available for laboratory tests. Persistent colonization of MRSA was defined as three consecutive positive ASCs. 11 ICU-acquired MRSA was defined as a positive result for MRSA from ASCs or clinical cultures obtained more than 48 hr after ICU admission, when ASCs or clinical cultures were MRSA negative at the time of ICU admission.
We compared the clinical and microbiological characteristics of MRSA isolates between qacA/B-positive and qacA/B-negative MRSA. To estimate the transmission of selective MRSA strains in the ICU, we adopted the conventional criteria for patient-to-patient transmission, defined by overlapping stay with a patient carrying the same staphylococcal protein A (spa) type.12,13
Microbiological methods
For ASCs, MRSA was initially identified by using MRSA-selective agar (CHROMagar®; BD Diagnostics, Sparks, MD), and it was confirmed by coagulase testing by using a plasma agglutination assay (BD Diagnostics) and polymerase chain reaction (PCR) for mecA genes. MRSA isolates from clinical cultures were processed for identification and antimicrobial susceptibility tests by using the Vitek-2 system (bioMérieux, Durham, NC).
PCR amplification of the qacA/B genes was carried out by using the forward primers 5′-GCAGAAAGTGCAGAGTTCG-3′ and reverse primer 5′-CCAGTCCAATCATGCCTG-3′. S. aureus TS77 (qacA; RIKEN BRC, Ibaraki, Japan) and TPS162 (qacB; RIKEN BRC, Ibaraki, Japan) served as positive controls. 14 The minimal inhibitory concentrations (MICs) of chlorhexidine were determined by using a broth microdilution method and a 20% (w/v) chlorhexidine gluconate solution (Sigma-Aldrich, St Louis, MO); the final concentrations of the antiseptic were 0.5–32 μg/ml. 7 Resistance to mupirocin was identified by using the disk diffusion method, and high-level and low-level resistance were determined based on the Clinical and Laboratory Standards Institute guidelines. 15
The MIC of vancomycin was determined by using the ETEST (AB BIODISK, Solna, Sweden) according to the manufacturer's instructions. Hetero-resistant vancomycin-intermediate Staphylococcus aureus (hVISA) was detected by using the population analysis profiling area under the curve method as previously described. 16 We used the δ-hemolysin activity to determine agr functionality, as described elsewhere. 17 Spa typing, multilocus sequence typing (MLST), and staphylococcal cassette chromosome mec (SCCmec) typing were conducted according to previously published methods.18–20
Statistical analysis
Continuous and categorical variables were compared by using Mann–Whitney U-test and Fisher's exact test, respectively. All variables with p-values <0.10 in the univariate analysis were included in the multivariate analysis to identify the association between qacA/B carriage and clinical or microbiological findings in MRSA. Independent variables that had less than 10 outcomes for each variable were considered inadequate for analysis and were, therefore, not included in multiple logistic regression. 21 To avoid potential multicollinearity between MRSA strains and virulence profiles, we evaluated two multivariate models: one with and the other without MRSA sequence types. The Hosmer–Lemeshow goodness-of-fit test was performed to assess the overall fit of the models. All tests were two tailed, and a p-value <0.05 was considered statistically significant. All analyses were performed by using IBM SPSS ver. 20.0 (IBM Corporation, Armonk, NY).
Results
A total of 1,056 patients were admitted to the ICU during the study period, and 119 nonduplicated MRSA isolates were collected from 135 patients with MRSA colonization or infection. Among these 119 MRSA isolates, 93 (78.2%) were cultured from nasal swab samples and 26 (21.8%) were cultured from clinical specimens. Thirty-nine MRSA isolates (32.8%) carried the qacA/B genes, whereas 23 (19.3%) were mupirocin resistant, including three isolates (2.5%) with high-level mupirocin resistance.
The clinical characteristics of patients with qacA/B-positive isolates were compared with those of patients with qacA/B-negative isolates (Table 1). Patients with qacA/B-positive isolates were more likely to have ICU-acquired MRSA (p < 0.001), including isolates from clinical specimens (p = 0.006). Patients with qacA/B-positive isolates also had longer ICU stays (p = 0.030) and hospital stays (p < 0.001) than did patients with qacA/B-negative isolates. There was no significant difference between qacA/B-positive and qacA/B-negative isolates in terms of underlying diseases, mortality, or persistent MRSA isolation from ASC.
Data are no. (%) of patients, unless otherwise indicated.
Patients identified with MRSA at ICU admission were excluded.
Persistent MRSA isolation was defined as colonization with MRSA in three consecutive nasal surveillance cultures; 24 patients with less than three cultures were excluded, n = 95.
Patients with at least one positive MRSA clinical culture obtained more than 48 hr after ICU admission, when surveillance or clinical cultures were MRSA negative at the time of ICU admission.
Includes seven sputum, two blood, and one pleural fluid.
Includes four sputum and one surgical site.
MRSA, methicillin-resistant Staphylococcus aureus; IQR, interquartile range; APACHE, Acute Physiologic Assessment and Chronic Health Evaluation; ICU, intensive care unit; ASC, active surveillance culture; LOS, length of stay.
The microbiological characteristics of the MRSA isolates are shown in Table 2. Of the 119 isolates, 116 (97.5%) comprised three MRSA strains: ST5-SCCmecII (51 isolates, 42.9%), ST239-SCCmecIII (10, 8.4%), and ST72-SCCmecIV (55, 46.2%). The qacA/B-positive isolates were classified into three MLST types: ST5 (n = 27, 69.2%), ST239 (n = 9, 23.1%), and ST 72 (n = 2, 5.1%). They were also classified into several spa types: t2460 (n = 16, 41.0%), t037 (n = 9, 23.1%), t9353 (n = 6, 15.4%), and “other” (n = 8, 20.5%). ST5-t2460 (n = 16, 41.0%), ST239-t037 (n = 9, 23.1%), and ST5-t9353 (n = 6, 15.4%) were the dominant clones among the qacA/B-positive MRSA isolates. The proportion of qacA/B-positive MRSA isolates in each MLST type did not differ significantly between isolates obtained within 2 days after ICU admission and isolates obtained later than 2 days after admission (ST72, 2.2% vs. 10.0%, p = 0.799; ST5, 52.9% vs. 52.9%, p = 0.999; ST239, 50.0% vs. 90.0%, p = 0.729).
Data are no. (%) of patients, unless otherwise indicated.
The other MLSTs were ST89 (n = 1) and ST188 (n = 1) in the qacA/B-negative group. One isolate in the qacA/B-positive group could not be typed.
The other spa types were t9363 (n = 2) and t2882 (n = 1) in the qacA/B-positive group and t4359 (n = 5), t148 (n = 5), t2431 (n = 3), t067 (n = 2), t9363 (n = 1), t10557 (n = 1), t10567 (n = 1), t12356 (n = 1), t1346 (n = 1), t189 (n = 1), and t375 (n = 1) in the qacA/B-negative group. Two isolates in the qacA/B-positive group and two in the qacA/B-negative group could not be typed.
When we estimated the cross-transmission of MRSA strains in the ICU, 47.2% (25/53) met the definition of patient-to-patient transmission. Cross-transmission of strains ST5-t2460, ST5-t9353, ST239-t037, and ST72-t4359 was detected in 10, 8, 5, and 2 patients, respectively. Of the 25 possible cross-transmitted cases, 17 (68.0%) carried qacA/B genes and 23 (92.0%) had ST5-SCCmecII or ST239-SCCmecIII. Among the MRSA isolates from patients who had overlapping ICU stays, qacA/B genes were usually identified in specific spa types (t2460, t9353, and t037; Fig. 1).
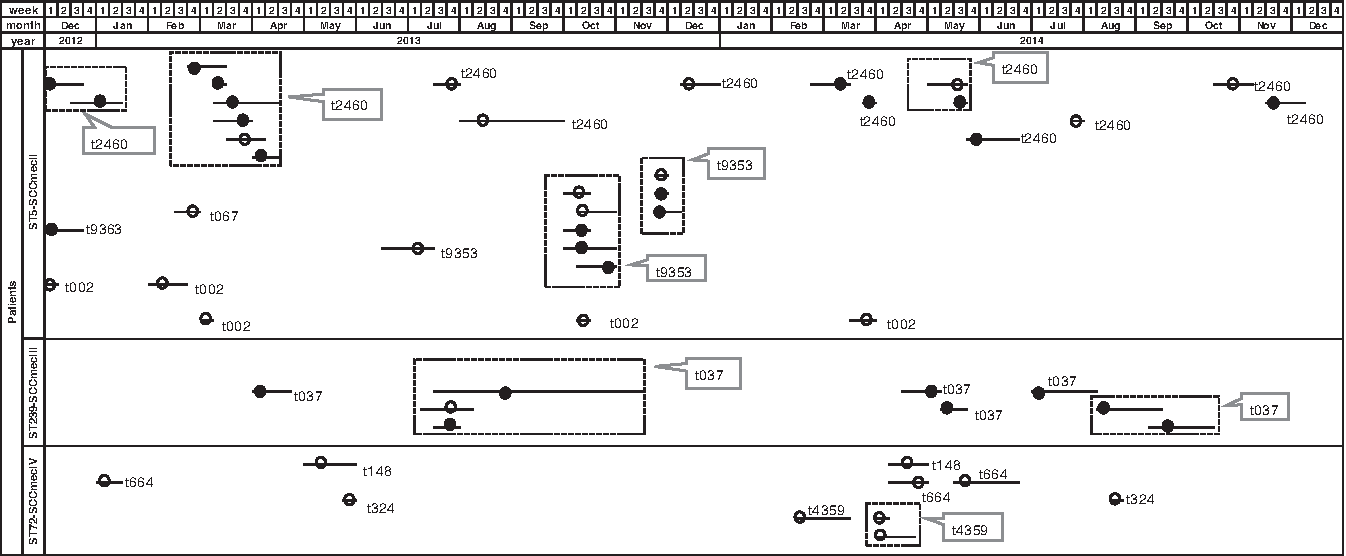
Detailed timeline of 53 patients who acquired MRSA during their ICU stays. Each dot (● or ○) represents a patient who acquired MRSA. The length of the bar indicates the duration of ICU stay. The position of the dot on the bar indicates when the first MRSA strain was isolated. The black dot represents qacA/B carriage. The number indicates the spa type. The dotted box represents possible patient-to-patient transmission. MRSA, methicillin-resistant Staphylococcus aureus; ICU, intensive care unit.
Meanwhile, qacA/B-positive isolates were more likely than were qacA/B-negative isolates to exhibit mupirocin resistance (p < 0.001), a chlorhexidine MIC ≥8 mg/L (p = 0.005), agr dysfunction (p < 0.001), and the hVISA phenotype (p < 0.001). Multivariate analysis revealed that qacA/B-positive MRSA isolates were associated with agr dysfunction (OR, 4.18; 95% CI, 1.43–12.20; p = 0.009), the hVISA phenotype (OR, 4.03; 95% CI, 1.47–11.10; p = 0.007), and ST5-SCCmecII (OR, 3.35; 95% CI, 1.14–9.83; p = 0.028). When multivariate analysis was repeated after removing ST5-SCCmecII from the model to exclude multicollinearity, qacA/B-positive MRSA isolates were significantly associated with agr dysfunction (OR, 4.87; 95% CI, 1.71–13.87; p = 0.003) and the hVISA phenotype (OR, 4.09; 95% CI, 1.48–11.34; p = 0.007). The p-values for the Hosmer–Lemeshow goodness-of-fit test were >0.05, indicating that all models fit the data well.
Discussion
In this study, we found that 32.8% of MRSA isolates carried the qacA/B genes, and these genes were present in a particularly high proportion of ST5-SCCmecII and ST239-SCCmecIII isolates, two dominant healthcare-associated (HA) MRSA clones in South Korea. 22 However, the qacA/B genes were rarely present in the ST72-SCCmecIV strain, a major community-associated-MRSA clone that has also become a common HA clone in South Korea. 23
The clonal association of qacA/B in MRSA has been controversial. In a recent multi-center study from the United States, only 0.99% (4/403) of MRSA isolates were found to carry qacA/B genes in patients undergoing chlorhexidine-based MRSA decolonization. 24 Conversely, another U.S. study showed that 22.7% of 247 nosocomial MRSA isolates carried qacA/B. 10 The qacA/B genes were detected in MRSA strains with diverse sequence types in these two U.S. studies,10,24 whereas a Chinese study found that 15 (60%) out of 25 qacA/B-positive isolates (out of a total of 321 MRSA isolates) belonged to the ST239-SCCmecIII strain. 7 Similarly, a Taiwanese study revealed a high frequency of qacA/B among specific sequence types, including ST239, ST5, and ST241. 25 In this study, spa typing showed that the qacA/B genes are common in the t2460, t037, and t9353 strains, which is consistent with previous reports from China and Korea.7,26 However, these studies did not elucidate the possible transmission of qacA/B genes among the MRSA strains in a hospital environment. When we compared the proportion of qacA/B in each MRSA sequence type between isolates obtained within 2 days after ICU admission and those obtained later, we found no significant difference. In addition, of the MRSA carriers with overlapping ICU stays, qacA/B genes were usually identified in specific spa types. These findings suggest that the spread of qacA/B among MRSA strains in the ICU was unlikely to have occurred during the study period.
To explore the selective advantage of qacA/B-positive MRSA in the hospital setting, we analyzed differences in antiseptic resistance and virulence profiles among our MRSA strains. Multivariate analysis showed that qacA/B-positive MRSA isolates were significantly associated with the hVISA phenotype and agr dysfunction. The clinical significance of the relationship among the carriage of qacA/B, the hVISA phenotype, and agr dysfunction has not been well evaluated. Only one study reported that the carriage of qacA/B genes may confer a selective advantage on VISA during chlorhexidine bathing, which could lead to the spread of VISA strains as a result of vancomycin treatment failure. 27 However, there have been no reports on the relationship between qacA/B carriage and the hVISA phenotype. Chong et al. reported that agr dysfunction was significantly associated with the hVISA phenotype; agr dysfunction is also prevalent in ST5-SCCmecII-agr group II and ST239-SCCmecIII-agr group I MRSA isolates in Korea, strains that were also common among our MRSA isolates. 28 Several studies have reported an association between agr dysfunction and reduced vancomycin susceptibility and suggested that the loss of agr function confers a potential survival advantage under vancomycin selection pressure in healthcare settings.28,29
Some may argue that the association among qacA/B genes, the hVISA phenotype, and agr dysfunction simply reflects a predominance of certain MRSA strains, such as ST5-SCCmecII and ST239-SCCmecIII. However, previous studies reported that agr dysfunction is associated with increased biofilm production, persistence, and prolonged bacteremia, which may confer a survival advantage on agr-dysfunctional strains.29,30 Moreover, other studies have shown that qacA/B genes are located on plasmids, which often share mobile genetic elements with other antibiotic resistance genes, including beta-lactams, aminoglycosides, and trimethoprim. 5 In this context, the presence of chlorhexidine tolerance genes may confer an additional advantage to certain MRSA strains with agr dysfunction or the hVISA phenotype to survive during chlorhexidine bathing.
We also evaluated the relationship between the presence of antiseptic resistance and decolonization failure. We found a relatively high frequency of coexistence of the qacA/B genes with mupirocin resistance (38.5%, mostly low-level resistance), which is in line with previous studies.7,31 Although the association between high-level mupirocin resistance and MRSA decolonization failure has been well documented, there are relatively few data on low-level mupirocin resistance and decolonization failure. 3 When we assessed reduced chlorhexidine susceptibility by using an MIC cut-off of ≥8 μg/ml, 24 we found a correlation between qacA/B carriage and reduced chlorhexidine susceptibility. Persistent MRSA colonization was not significantly associated with the presence of qacA/B genes in this study. However, because decolonization failure and the MIC cut-off for reduced chlorhexidine susceptibility have not been well defined to date,5,9 we should exercise caution in interpreting the decolonization results of this study.
Our study had several limitations. First, it was conducted at a single ICU; because there are considerable geographical differences in qacA/B carriage, our findings should not be generalized to other hospital settings or to other countries. 5 Second, the imperfect sensitivity of nasal surveillance cultures from samples obtained on admission and possible recolonization of the same patients with a different MRSA strain may have caused misclassification of MRSA isolates. 32 Third, we did not evaluate the epidemiologic link between MRSA-colonized patients and subsequent infection, because we collected only a small number of paired isolates from surveillance and clinical cultures from each patient. Fourth, the use of a conventional method to investigate transmission using spa typing could falsely suggest cross-transmission between patients due to its low discriminatory power in comparison with pulsed-field gel electrophoresis or whole-genome sequencing.12,33
In conclusion, this study showed that qacA/B carriage was common among MRSA isolates in an ICU where chlorhexidine bathing is routine. The carriage of qacA/B was significantly associated with agr dysfunction and the hVISA phenotype, which may confer selective advantages on HA-MRSA strains, including ST5-SCCmecII and ST239-SCCmecIII, during decolonization with chlorhexidine.
Footnotes
Acknowledgments
This study was supported by Clinical Research Fund (GNUHCRF-2010-007) from the Gyeongsang National University Hospital.
The pathogen resources for this study were provided by Gyeongsang National University Hospital (GNUH), as the Branch of National Culture Collection for Pathogens (NCCP). This research was supported by the National Culture Collection for Pathogens (NCCP) R&D project of the Ministry of Health & Welfare (2015-ER4701-00).
Disclosure Statement
No competing financial interests exist.