
Abstract
Despite global efforts to tackle resistance in extended-spectrum beta-lactamase (ESBL)-producing isolates via old antibiotics, there are limited data on the efficacy of fosfomycin—an old oral antibiotic—against Enterobacteriaceae in the Middle East. The purpose of this study was to evaluate the in vitro activity of fosfomycin against urinary ESBL-producing isolates of Enterobacteriaceae. Between 2004 and 2015, 363 isolates of ESBL-producing Enterobacteriaceae were recovered from high-risk patients suffering from cardiac disorders and were subjected to polymerase chain reaction using specific primers for the blaTEM, blaSHV, and blaCTX-M genes. Antibiotic susceptibility testing was performed for fosfomycin and other antibiotic comparators. For the isolates considered nonsusceptible to fosfomycin by disk diffusion, the minimum inhibitory concentration (MIC) was determined. The susceptibility rate to fosfomycin remained almost steady (90–100%) over a 12-year period, although it fluctuated vis-à-vis ciprofloxacin (0–54%), trimethoprim/sulfamethoxazole (9.1–31.7%), and nitrofurantoin (41.7–100%). Of all the antibiotics tested, fosfomycin was the most active antimicrobial agent (97%) against the ESBL-positive isolates. Fosfomycin maintained higher activity against ESBL-Escherichia coli than against ESBL-Klebsiella pneumoniae. Only 11 (3%) isolates were not susceptible to fosfomycin according to disk diffusion and they had MICs greater than 1,024 mg/ml. All of the fosfomycin-nonsusceptible isolates were positive for the blaCTX-M gene (100%), while 5 (45.4%) and 3 (27.3%) of the isolates harbored the blaTEM and blaSHV genes, respectively. We showed that fosfomycin had a numerically higher susceptibility rate than the other antibiotics against the ESBL-producing isolates of the most common Enterobacteriaceae. Given its low resistance rate and oral administration, fosfomycin may be deemed a promising antibiotic for the treatment of urinary tract infections caused by ESBL-producing Enterobacteriaceae.
Introduction
A
Antibiotic-resistant UTIs are potentially serious problems. In addition, severe consequences of UTIs such as recurrent UTIs, kidney damage, and eventually sepsis may prove life threatening. The treatment of these infections is, therefore, a major therapeutic challenge magnified by the lack of development of new antibiotics.8–11
Reviving old and neglected antibiotics is regarded as a new strategy to overcome antibiotic resistance and to expand the treatment options. Of old antibiotics, fosfomycin has been recommended for the treatment of UTIs, despite the fact that its development dates back to more than four decades. For all the efforts the world over to tackle this problem, there is a dearth of data on the efficacy of fosfomycin against the most common Enterobacteriaceae in Iran—one of the largest countries in the Middle East. We, consequently, aimed to evaluate the in vitro activity of fosfomycin against ESBL-producing E. coli, K. pneumoniae, Klebsiella oxytoca, and Enterobacter cloacae isolates recovered from UTIs in high-risk patients suffering from cardiac disorders.
Materials and Methods
This study was conducted at Tehran Heart Center (THC), a tertiary care center. A 460-bed hospital, THC is affiliated with Tehran University of Medical Sciences and provides a variety of diagnostic, surgical, nonsurgical, therapeutic, and rehabilitation services for substantial numbers of patients with cardiovascular diseases from various districts of Tehran, Iran, and all other cities around the country.
The study population comprised patients who were referred to THC because of cardiovascular diseases such as myocardial infarction, cardiomyopathy, heart failure, congenital heart disease, mitral regurgitation, and arrhythmia between 2004 and 2015. The patients were admitted to units dedicated to high-risk cardiac patients such as the intensive care unit, coronary care unit, heart surgery department, and emergency department. Demographic characteristics and medical histories were collected from medical files.
Isolates
The isolates were identified using standard phenotypic microbiologic tests and commercial strips, API 20 E (bioMérieux, France). 12 The ESBLs were detected using the combination disk test in accordance with the guidelines of the Clinical and Laboratory Standards Institute (CLSI). In this test, a ceftazidime (30 μg) and cefotaxime (30 μg) disk was applied alone and in combination with clavulanic acid (30/10 μg). An increase equal to or greater than 5 mm in the inhibition zone of the agent in combination with clavulanic acid was considered positive for the production of ESBLs. 13 E. coli ATCC 25922 and K. pneumoniae ATCC 700603 strains were used as negative control and positive control, correspondingly. In addition, following the extraction of total DNA, the ESBL genes, namely blaTEM, blaSHV, and blaCTX-M, were identified via polymerase chain reaction using gene-specific primers. 14
Antimicrobial susceptibility testing
The susceptibility of the isolates of E. coli and K. pneumoniae as well as that of the other isolates was determined to fosfomycin (200 μg), imipenem (10 μg), amikacin (30 μg), nitrofurantoin (300 μg), meropenem (10 μg), gentamicin (10 μg), ciprofloxacin (5 μg), ceftazidime (30 μg), trimethoprim/sulfamethoxazole (1.25 μg/23.75 μg), and cefepime (30 μg) using disk diffusion according to the CLSI guidelines. 14 In addition, MIC Test Strips (Liofilchem, Italy) were used to determine the minimum inhibitory concentrations (MICs) of fosfomycin against the isolates considered nonsusceptible (intermediate/resistant) by the disk diffusion method. The results were evaluated using the CLSI breakpoints and interpretive categories for the zone diameter and the MIC. 13 Because no fosfomycin breakpoints for K. pneumoniae were recommended by the CLSI, the disk diffusion breakpoints for E. coli were considered for interpretation. E. coli strain ATCC 25922 was used as the susceptibility test quality control.
Statistical analysis
Data analysis was performed using SPSS version 18.0 (SPSS, Inc.). The descriptive results were shown as frequencies and means.
Results
Cases and isolates
Over a 12-year period, a collection of 363 nonduplicated ESBL-producing E. coli (ESBL-EC), K. pneumoniae (ESBL-KP), K. oxytoca, and E. cloacae were recovered from cardiac patients suffering from UTIs. The number of isolates between 2004 and 2015 ranged from 1 to 103 and from 1 to 11 for E. coli and K. pneumoniae, respectively. The patients' age ranged from 3 to 93 with mean ± SD of 64.6 ± 14.8 years and median of 66 years. Most of the isolates were obtained from individuals admitted as inpatients (either nosocomial or community acquired) (286 out of 356, 80.3%), and the remaining 19.7% of the isolates were obtained from outpatients. Fewer than 50% (47.7%) of the infected cases were hospitalized in the critical care unit; the remaining patients were hospitalized in the heart surgery department (23.0%), the intensive care unit (8.7%), and the emergency department (0.9%). More than half of the ESBL-producing Enterobacteriaceae isolates were obtained from females (n = 251, 69.1%). The demographic characteristics and medical histories of the patients are presented in Table 1.
ESBL, extended-spectrum beta-lactamase; EC, Escherichia coli; KP, Klebsiella pneumonia.
Between 2004 and 2015, the majority of the collected ESBL-producing Enterobacteriaceae were E. coli (n = 313, 86.2%), with the other isolates comprising K. pneumoniae (n = 47, 12.9%), K. oxytoca (n = 2, 0.5%), and E. cloacae (n = 1, 0.3%).
Susceptibility of the isolates
The susceptibility trend of the ESBL-producing isolates to fosfomycin, compared to the other antibiotics of choice for UTI treatment, including ciprofloxacin, nitrofurantoin, and trimethoprim/sulfamethoxazole, during the study period is depicted in Fig. 1. As is illustrated, the susceptibility to fosfomycin ranged from 90% to 100%, which was substantially higher than ciprofloxacin (0–54%) and trimethoprim/sulfamethoxazole (9.1–31.7%). Moreover, the susceptibility rate to nitrofurantoin (41.7–100%) was higher than that to ciprofloxacin, but the in vitro activity of nitrofurantoin was not comparable to that of fosfomycin. While the susceptibility rate to ciprofloxacin and nitrofurantoin fluctuated over the 12-year period, it remained almost steady for fosfomycin.
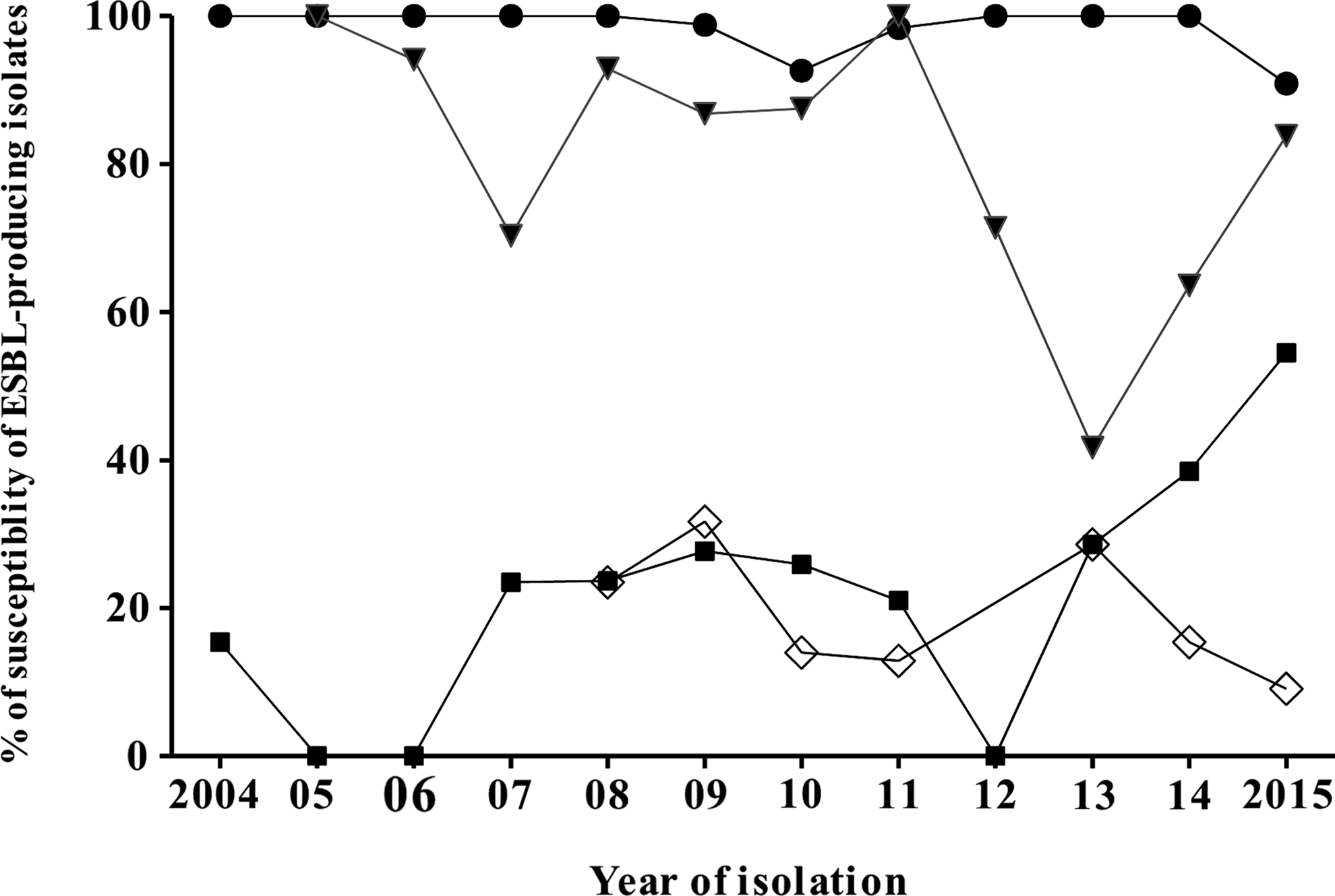
Percentages of susceptibility of ESBL-producing Enterobacteriaceae isolates against fosfomycin (●), nitrofurantoin (▼), ciprofloxacin (■), and trimethoprim/sulfamethoxazole (◊) in relation to year of isolation, 2004–2015. ESBL, extended-spectrum beta-lactamases.
The susceptibility rates of the isolates to fosfomycin and the other antibiotics are demonstrated in Table 2. Among the antibiotics tested, fosfomycin was the most active antimicrobial agent (97%) against the ESBL-positive isolates and imipenem had a notable in vitro activity (94.7%). However, among the ESBL isolates, there were differences in the susceptibility rates to imipenem and meropenem: the susceptibility rate to imipenem was higher than that to meropenem. For 306 (97.8%) of the ESBL-EC isolates, the inhibition zone ranged from 18 to 42 mm, whereas for 42 (91.3%) of the ESBL-KP isolates, the inhibition zone varied from 16 to 30 mm; all were considered susceptible to fosfomycin. Fosfomycin, in particular, maintained higher activity to ESBL-EC than ESBL-KP. Furthermore, the ESBL-EC isolates had a numerically higher susceptibility rate than the ESBL-KP isolates to nitrofurantoin, ceftazidime, and cefepime.
According to the disk diffusion test, in total, only 11/363 (3%) of the isolates were not susceptible to fosfomycin: 7/313 (2.2%) of the ESBL-EC and 4/46 (8.7%) of the ESBL-KP isolates. The isolates classified as “intermediate susceptible” to fosfomycin by the disk diffusion method were found resistant using the MIC Test Strips (MIC >1,024 mg/ml).
Apropos the detection of the ESBL genes, the most frequent gene was blaCTX-M (74.2%), followed by blaTEM (54.6%) and blaSHV (14.4%). Although the distributions of the blaCTX-M and blaTEM genes were almost similar between the ESBL-EC and ESBL-KP isolates (Table 3), the blaSHV gene was more frequently found in the ESBL-KP (91.1%) than in the ESBL-EC (2.6%) isolates. The 11 fosfomycin-nonsusceptible isolates (with intermediate susceptibility or resistance to fosfomycin) were positive for the blaCTX-M (100%) gene, while 5 (45.4%) and 3 (27.3%) of the isolates harbored the blaTEM and blaSHV genes, correspondingly (Table 4).
Discussion
Notwithstanding the high distribution of ESBL-producing Enterobacteriaceae in various regions around the world,15,16 the studies pointing to the activity of fosfomycin against such isolates in the Middle East are few. Fosfomycin has been utilized for the treatment of infections, particularly against veterinary infections, over the past decades.17,18 In addition, the usefulness of fosfomycin has been highlighted in recent CLSI reports, proposing the effectiveness of fosfomycin for the treatment of ESBL-associated UTIs. 13 Due to the increasing rate of antibiotic resistance and resultant limited antibiotics of choice, there is a significant demand for reviving old antibiotics, mainly those prescribed orally such as fosfomycin. Accordingly, we conducted the present study to analyze the activity of fosfomycin against a collection of large series of ESBL-EC and ESBL-KP.
We observed a steady trend of susceptibility of the ESBL isolates to fosfomycin over a 12-year period. Nevertheless, the susceptibility rates of the other antibiotics, including ciprofloxacin, nitrofurantoin, and trimethoprim/sulfamethoxazole, were lower than that of fosfomycin. Another finding of the current study is that the majority of the ESBL isolates exhibited susceptibility to fosfomycin, despite their considerable resistance to several beta-lactams.
Although the overall activity of fosfomycin against ESBL-Enterobacteriaceae was good, it should be taken into account that the ESBL-KP isolates were more likely to be resistant than the ESBL-EC isolates. The higher activity of fosfomycin against ESBL-EC was previously supported by other studies.1,19,20 We found an overall resistance rate of 3% to fosfomycin in the current study, with the resistance rates being 2.23% in the ESBL-EC and 8.7% in the ESBL-KP isolates. A systematic review by Falagas et al. showed an approximately similar resistance rate (3.2%) for ESBL-EC to fosfomycin. 1 A study conducted in Spain via the disk diffusion method reported susceptibility results for ESBL-KP to fosfomycin (7.2%) similar to those in our study. 21 Using the disk diffusion method, other studies have reported resistance rates of 0–13.1% for ESBL-EC1,19,21–28 and 7.2–42.4% for ESBL-KP.1,19,20,22,24–26,28,29 Similar studies using disk diffusion in our neighboring countries such as Turkey and Pakistan have reported 5.9% and 7% resistance rates in E. coli and 33.9% and 36% resistance rates in K. pneumoniae, which are higher than those in our study.24,26 In a study recently conducted in the northwest of Iran with the disk diffusion method, 2.7% of the ESBL isolates were found resistant to fosfomycin. 30 In the present study, we detected 11 isolates as fosfomycin nonsusceptible with intermediate susceptibility or resistance. All the fosfomycin-nonsusceptible isolates harbored at least 1 ESBL gene. A notable issue is that the MICs for these isolates were equal to or greater than 1,024 mg/ml. Despite the low resistance rate to fosfomycin for the tested isolates, the fosfomycin-nonsusceptible isolates exhibited high levels of resistance via the E-test.
First and foremost among the limitations of the present study is that it was performed at only a single tertiary hospital. This single center is a specialty cardiac hospital, which may reduce the generalizability of our results. Another drawback of note is that we used MIC Test Strips (Liofilchem), containing glucose-6-phosphate, while the approved MIC method for MIC determination is agar dilution using agar media supplemented with 25 μg/ml of glucose-6-phosphate. 31
On the contrary, it is of prime importance to assess the susceptibility of ESBL pathogens in a large number of patients at high risk for the acquisition of drug-resistant bacteria and admitted at such long-term care facilities. Fosfomycin was approved by the Food and Drug Administration (FDA) in 1996 and is currently used in some European countries and the United States as an intravenous and/or oral antibiotic; nonetheless, resistance to fosfomycin is rare. The story is somehow different in our country as fosfomycin was not included in Iran's pharmacopoeia for clinical setting until 2015. The low rate of resistance in isolates from clinical setting over the years may imply that fosfomycin has its own mechanisms of resistance and also it has no cross-resistance to other antibiotics. In addition, the very high concentrations of fosfomycin in urine may kill microorganisms and prevent the selection of mutants.32,33
In conclusion, we showed that fosfomycin had a numerically higher in vitro susceptibility rate than other antibiotics against ESBL-producing isolates of the most common Enterobacteriaceae such as E. coli and K. pneumoniae. Given its low resistance rate and oral administration, fosfomycin could be a promising antibiotic for the treatment of high-risk cases. Further research is required to investigate the in vivo efficacy of this antibiotic against UTIs.
Footnotes
Acknowledgment
The authors acknowledge the valuable contribution of the staff of Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran.
Disclosure Statement
The authors declare that they have no conflict of interest.