
Abstract
Enzymatic alteration of aminoglycosides by aminoglycoside-modifying enzymes (AMEs) is the major mechanism of resistance to aminoglycosides. The purpose of this study was to determine the frequency of AME genes, staphylococcal chromosomal cassette mec (SCCmec) types, and molecular analysis of the coagulase (coa) gene in Staphylococcus aureus strains isolated from clinical specimens. Totally, 102 S. aureus were tested by disk diffusion and microbroth dilution methods for susceptibility to aminoglycosides. AMEs genes and SCCmec types were determined by multiplex polymerase chain reaction (PCR). For polymorphism analysis, the 3′ end region of the coa gene was amplified by PCR and the products were then subjected to restriction digestion with HaeIII enzyme. Of the 102 S. aureus, 42 (41.2%) were methicillin-resistant S. aureus (MRSA). Thirty-five (83%) of MRSA strains were resistant to kanamycin, 32 (76.2%) to tobramycin, 30 (71.4%) to gentamicin, 25 (59.5%) to amikacin, and 10 (23.8%) to netilmicin. The aac(6′)-Ie-aph(2″) was the most frequent gene among MRSA isolates 19 (45.2%), followed by aph(3′)-IIIa 8 (19%), ant(4′)-Ia 6 (14.3%), and aph(2″)-Id 2 (4.8%). SCCmec types included type I 10 (23.8%), II 1 (2.4%), III 21 (50%), and IV 7 (16.7%). Three (7.2%) isolates were nontypeable. Digestion of the PCR products of the coa gene yielded 19 distinct restriction fragment length polymorphism patterns. In conclusion, given the alarming rate of resistance to aminoglycosides among MRSA, the monitoring of aminoglycoside resistance and AME genes should be performed to limit the spread of aminoglycoside resistance among MRSA isolates. Several variants of the coa gene were found in the studied isolates, although the majority of the MRSA isolates belonged to a limited number of coagulase types.
Introduction
M
Aminoglycosides are broad-spectrum antibiotics that are prescribed in combination with either β-lactams or vancomycin for the treatment of S. aureus infections, as these drugs act synergistically. 4 The principal mechanism of resistance to aminoglycosides is the structural modification of these antibiotics by aminoglycoside-modifying enzymes (AME), such as aminoglycoside phosphotransferase (APH), acetyltransferase (AAC), and nucleotidyltransferase (ANT). The most well-known AME encoding genes among S. aureus strains are the aac(6′)-Ie-aph(2″), ant(4′)-Ia, and aph(3′)-IIIa. 5 Many of these genes are carried on transposons or plasmids and can be potentially integrated into the staphylococcal chromosomal cassette mec (SCCmec) of S. aureus. 4
Molecular typing techniques, such as spa typing, pulsed-field gel electrophoresis, multilocus sequence typing, multilocus enzyme electrophoresis, and coagulase genotyping are commonly used to study the epidemiology of S. aureus strains.6,7 Polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) of the coa gene is a simple, accurate, reproducible, and easy-to-interpret method for typing of S. aureus. 8 Coagulase is produced by most of the S. aureus strains and the ability to produce the coagulase enzyme is routinely used to identify S. aureus in human infections. 9 The coa gene has highly polymorphic tandem repeats at the 3′-end region, the number of which differs between S. aureus strains. By restriction enzyme digestion of the amplified 3′-end region of the coa gene product, it is possible to differentiate between S. aureus strains.7,10
In the current study, we assessed the aminoglycoside resistance profiles, the distribution of aminoglycoside resistance genes, and SCCmec types among S. aureus isolates. Also, the genetic relatedness of these isolates was determined by coagulase (coa) gene typing.
Materials and Methods
Isolation and identification of S. aureus
A total of 102 clinical isolates of S. aureus were collected during January 2014 to April 2015, from clinical samples of three hospitals (Bahonar, Afzalipour, and Shafa), Kerman, south-east of Iran. Isolates were identified to the species level by Gram staining, production of coagulase, catalase, DNase, and oxidation and fermentation of mannitol. 11
Antimicrobial susceptibility testing
The antimicrobial susceptibility to amikacin 30 μg, gentamicin 10 μg, tobramycin 10 μg, kanamycin 30 μg, and netilmicin 30 μg was tested by disk diffusion method according to the Clinical and Laboratory Standards Institute (CLSI) guidelines. 12 For S. aureus isolates displaying gentamicin and amikacin resistance by disk diffusion method, the minimum inhibitory concentration (MIC) was determined in triplicate by using microdilution susceptibility test according to CLSI guidelines.
Detection of nuc and mecA genes
S. aureus DNA was extracted from isolates by the boiling method as previously outlined. 5
Identification of S. aureus was confirmed by detection of the species-specific nuc gene using PCR assay. 1 The presence of mecA gene was then examined by PCR. 13
Detection of AMEs genes and SCCmec types
All S. aureus isolates were investigated for the presence of aminoglycoside resistance genes by the multiplex PCR method as reported previously. 14 Staphylococcal cassette chromosome mec (SCCmec) types were also determined using a multiplex PCR as described by Oliveira and de Lencastre. 13
Amplification of coagulase gene and digestion of PCR products with HaeIII
Coagulase gene typing procedure for S. aureus was carried out with the method described by Hookey et al. with slight modification. 9 Briefly, 7–10 μL of PCR products were incubated with 10 U of HaeIII endonuclease enzyme (Fermentas), 5 μL of restriction buffer, and 34 μL of distilled water for 30 min at 37°C.
Results
Identification and antibiotic resistance
Of the 102 S. aureus isolates included in this study, 42 (41.2%) were MRSA. As expected, the MSSA isolates were mostly susceptible to aminoglycosides, whereas the majority of MRSA isolates were resistant to these antibiotics. The highest rates of resistance among MRSA isolates were detected for kanamycin 83.2% (35), followed by tobramycin 76.2% (32), gentamicin 71.4% (30), amikacin 59.5% (25), and netilmicin 23.8% (10). Among MSSA isolates, all isolates were uniformly susceptible to amikacin, whereas few of them showed resistance to gentamicin 3 (5%) and netilmicin 4 (6.7%). Moreover, resistance to kanamycin and tobramycin were observed in 14 (23.3%) of MSSA isolates. According to MIC results, gentamicin and amikacin MIC ranged between 8 and 1,024 mg/mL. Thirty-three percent of amikacin-resistant and 26% of gentamicin-resistant S. aureus isolates had a MIC of 128 and 512 μg/mL, respectively. All S. aureus isolates, except one, with gentamicin MIC ≥256 μg/mL and amikacin MIC ≥128 μg/mL, were positive for mecA gene.
Detection of AME genes and SCCmec types
Of 102 S. aureus isolates, 37 (25 MRSA and 12 MSSA) harbored 1 or 2 AME genes. Regardless of gene combinations, aac(6′)-Ie-aph(2″) (45.2%) was the most predominant AME gene among MRSA isolates, followed by aph(3′)-IIIa (19%), ant(4′)-Ia (14.3%), and aph(2″)-Id (4.8%). A significant association was seen between the presence of the aac(6′)-Ie-aph(2″) gene and the presence of the mecA gene (p < 0.05). Among MSSA isolates the ant(4′)-Ia gene was detected in 10% of isolates, followed by the aac(6′)-Ie-aph(2″) aph(3′)-IIIa and aph(2″)-Id, found in 6.7%, 6.7%, and 3.3% of isolates, respectively. As shown in Table 1 all S. aureus isolates, except one that contained ant(4′)-Ia gene, were resistant to kanamycin and tobramycin. Three S. aureus isolates were found without phenotypic resistance to aminoglycosides that possessed the AME genes, whereas 21 isolates that were resistant to aminoglycosides did not contain any of the AME genes. Neither aph(2″)-Ib nor aph(2″)-Ic genes were detected among the S. aureus isolates. Of the 42 MRSA isolates identified, 10 (23.8%) harbored SCCmec type I, 1 (2.4%) SCCmec type II, 21 (50%) SCCmec type III, and 7 (16.7%) SCCmec type IV. Three (7.2%) isolates were nontypeable by the Oliveira method.
Relationship Between the Presence of the Aminoglycoside-Modifying Enzyme Genes and Various Aminoglycoside Resistance Phenotypes in Methicillin-Susceptible Staphylococcus aureus and Methicillin-Resistant Staphylococcus aureus Isolates
+, present; −, absent; AK, amikacin; AME, aminoglycoside-modifying enzymes; GM, gentamicin; K, kanamycin; MRSA, methicillin- resistant S. aureus; MSSA, methicillin-susceptible S. aureus; NET, netilmicin; TN, tobramycin.
Amplification of the 3′ end region of the coagulase gene
PCR amplification of the 3′ end region of coa produced 11 different PCR products, ranging approximately from 480 to 920 bp (genotype I–XI). Figure 1 shows some of the coa band patterns. PCR products with 700 bp in size (genotype I) were dominant in S. aureus isolates. Genotype III (500 bp) was only observed in 10 MSSA isolates.
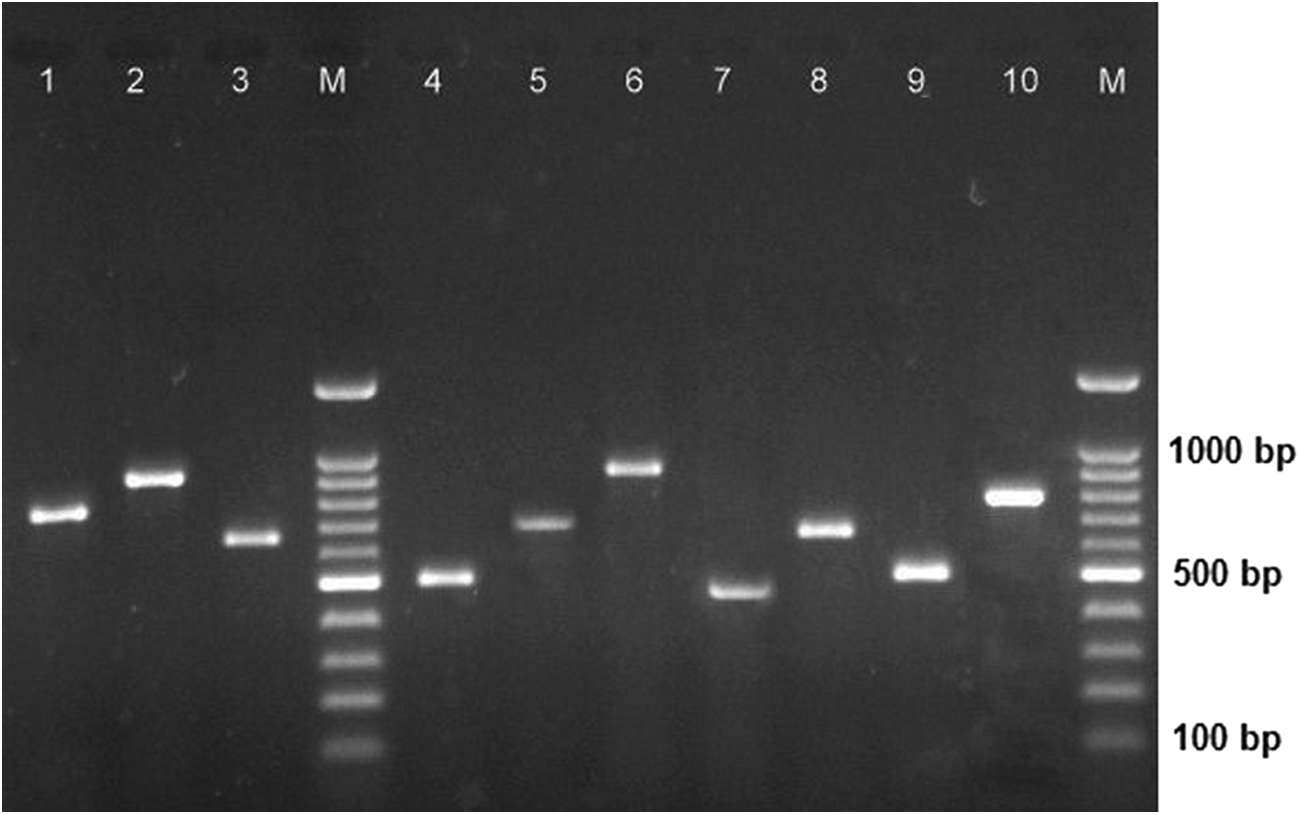
Agarose gel electrophoresis of coa gene PCR products. M, 100-bp molecular size marker; Lane 1, coa genotype V; Lanes 2 and 6, coa genotype VII; Lane 3, coa genotype VI; Lane 4, coa genotype IX; Lane 5, coa genotype I; Lane 7, coa genotype VIII; Lane 8, coa genotype II; Lane 9, coa genotype III; and Lane 10, coa genotype XI. PCR, polymerase chain reaction.
HaeIII restriction enzyme digestion
Digestion of the PCR products with HaeIII produced two to four bands in each isolate (Fig. 2). Based on the number and size of produced bands, 19 distinct RFLP banding patterns were observed (Table 2). RFLP pattern A (320-220-160) and pattern B (310-210-180) were found to be the most common patterns. The strains with RFLP patterns A and B carried different SCCmec cassettes, although none of them was positive for SCCmec type IV. Ten isolates fell into RFLP pattern K, in which all of them were MSSA. Pattern G was only found among eight MRSA isolates. These isolates belonged to SCCmec type III (Table 3). Four isolates that belonged to RFLP pattern M carried SCCmec type IV, and all of them were negative for AME genes.
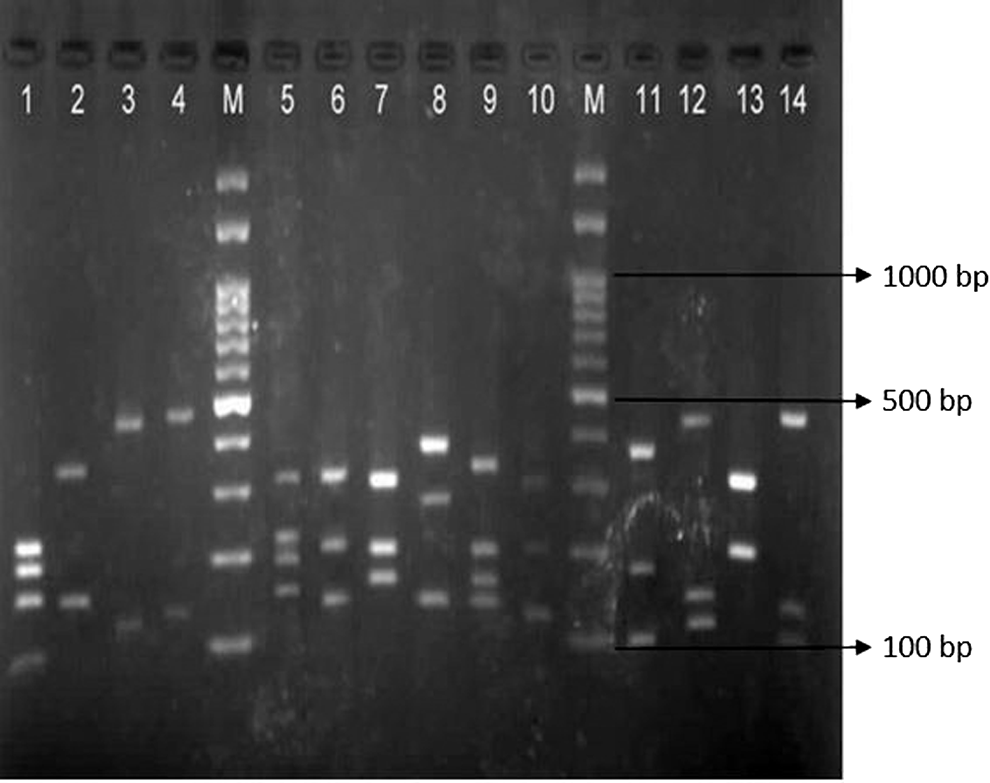
RFLP patterns of the coa gene amplicons following digestion with the restriction endonuclease HaeIII. M, 100-bp molecular size marker; Lane 1, PCR-RFLP pattern J; Lane 2, PCR-RFLP pattern P; Lane 3, PCR-RFLP pattern R; Lane 4, PCR-RFLP pattern L; Lane 5, PCR-RFLP pattern S; Lane 6, PCR-RFLP pattern A; Lane 7, PCR-RFLP pattern B; Lane 8, PCR-RFLP pattern M; Lane 9, PCR-RFLP pattern O; Lane 10, PCR-RFLP pattern G; Lane 11, PCR-RFLP pattern N; Lane 12, PCR-RFLP pattern C; Lane 13, PCR-RFLP pattern K; and Lane 14, PCR-RFLP pattern E. RFLP, restriction fragment length polymorphism.
Coa Genotype and Coa Restriction Fragment Length Polymorphism Patterns of Methicillin-Susceptible Staphylococcus aureus and Methicillin-Resistant Staphylococcus aureus Isolates
PCR, polymerase chain reaction; RFLP, restriction fragment length polymorphism.
Distribution of Aminoglycoside-Modifying Enzyme-Encoding Genes, SCCmec Type and Coa Restriction Fragment Length Polymorphism Patterns of Methicillin-Resistant Staphylococcus aureus Isolates
−, absent; NT, nontypeable; SCCmec, staphylococcal chromosomal cassette mec.
Discussion
The aminoglycosides have been extensively used in combination with other antibiotics, such as β-lactams and glycopeptides for the treatment of S. aureus infections. However, the increasing emergence of the resistant isolates, mostly mediated by AMEs, compromises the therapeutic effectiveness of these antimicrobial agents. Of the aminoglycosides, amikacin exhibited the greatest activity against MSSA isolates, whereas, in accordance with other studies netilmicin had excellent activity against MRSA isolates.15,16 Most of the MRSA isolates were resistant to kanamycin and tobramycin. These findings are similar to previous reports in other studies.4,16,17 As stated in the previous study, most of the isolates with high-level resistance to gentamicin (MIC ≥256 μg/mL) were positive for mecA gene. 17
As reported in some studies, aac(6′)-Ie-aph(2″) was the most prominent AME gene among the S. aureus isolates.18–20 The AAC(6′)-APH(2″) is a bifunctional enzyme that inactivates a broad range of clinically valuable aminoglycosides and confers resistance to the majority of aminoglycosides commonly used in medical practice. 21 In the present study, all of the isolates positive for aac(6′)-Ie-aph(2″) gene showed resistance at least to one of the aminoglycosides.
APH(3′)-IIIa enzyme encoded by the aph(3′)-IIIa gene has also been found to mediate resistance to neomycin and kanamycin in staphylococci. 22 According to our finding, all of the isolates, except one which carried aph(3′)-IIIa gene, were resistant to kanamycin.
Our results are in contrast to reports from Kuwait, Japan, and Poland, where the ant(4′)-Ia is the most common AME gene.16,17,23 However, the results are consistent with the report indicating that the ant(4′)-Ia gene is dominant among the tobramycin- and kanamycin-resistant isolates. 3 The least common gene identified was aph(2″)-Id, which was detected in 3.9% of isolates. Although the frequency of aph(2″)-Id gene was low, in previous studies this gene was not found in S. aureus isolates.5,19,24
Enzymatic inactivation is the main mechanism of S. aureus resistance to aminoglycosides, although, some isolates have exhibited AME-independent resistance to these antibiotics. 25 We found that 20.4% of the isolates that were resistant to some of the aminoglycosides had no AME genes. This result is in agreement with that obtained by Hauschild et al. 16 This could be due to other resistance mechanisms, such as amino acid alteration in ribosomal proteins, decreased permeability of the antibiotics, and the presence of unknown AME genes.19,22 In contrast, we found three isolates, which were aminoglycoside susceptible, but had AME genes. Two studies stated that observation of resistance genes in antibiotic-sensitive strains may be due to amplification of repressed antibiotic resistance gene or lower enzymatic activity of AME of these strains.1,16 The present study reveals an association between the presence of AME genes and mecA gene. These genes may be positioned on the same or related genetic element. For example SCCmec type III, which was the most frequent SCCmec type in the current study, carried not only the mecA gene, but also the genes encoding resistance to several non-beta-lactam antibiotics, including aminoglycosides. 5
SCCmec typing is a useful technique in epidemiological studies of MRSA. Our results are consistent with other studies, in which they found type III as the major type in MRSA strains.4,24,26 The majority of these isolates were resistant to aminoglycosides and possessed the AME genes. However, of the seven SCCmec type IV isolates, only one carried AME genes. Unlike SCCmec types II and III, SCCmec type IV is a small element and carry no other antibiotic resistance genes, except mecA. 27
RFLP of the coagulase gene has been used widely for the typing of S. aureus. Coagulase gene typing is applicable for typing of a large number of strains in a short time, so it is an efficient method for epidemiological investigation of S. aureus infection. A previous study has shown that PCR-RFLP of coa gene has a better discriminatory power than spa typing. 28 Although, in another study, spa typing showed more discriminatory power than coa typing. 29 HaeIII digestion of coa PCR products yielded 19 RFLP patterns among the 102 isolates, and this agreed partly with Abdulghany and Khairy, who reported 10 distinct patterns among 54 isolates. 30 However, our finding disagreed with Mahmoudi et al. who reported 8 patterns in 200 isolates, and that reported in India, 31 AluI RFLP patterns in 85 isolates.31,32 Previous studies showed that the discriminatory power of PCR-RFLP partly depended upon the type of restriction enzyme used.7,32 Different restriction enzymes generate various banding patterns and often different band numbers, which would influence the typing results. In the present study, most cases of MRSA infections were caused by strains with the PCR-RFLP patterns A, B, and G. Additionally, 10 isolates, which had coa genotype III and PCR-RFLP pattern K, were MSSA. It seems that in our hospitals S. aureus infections, especially MRSA, are related to specific clones.
In conclusion, the aac(6′)-Ie-aph(2″) was the most frequent aminoglycoside-modifying enzyme gene identified in S. aureus isolates. Most of the isolates which carried the aac(6′)-Ie-aph(2″) gene also contained the mecA gene. Given the alarming rate of resistance to aminoglycoside among MRSA, the monitoring of aminoglycoside resistance and AME genes should be performed to reduce treatment failure in patients with staphylococcal infections. Coagulase gene typing and PCR-RFLP of the coa gene provide simple, inexpensive, and efficient results for epidemiological investigations during nosocomial outbreaks and are able to partly discriminate between the epidemic and sporadic isolates.
Footnotes
Acknowledgment
The authors acknowledge Kerman University of Medical Sciences for the financial support.
Disclosure Statement
No competing financial interests exist.