
Abstract
The progressive increase of infections produced by extensively drug-resistant carbapenemase-producing Klebsiella pneumoniae (XDR-CPKP) represents an important threat to public health. Unfortunately, optimal therapeutic options are scarce. Retrospective studies have recommended combined therapy with more than one antibiotic and, more recently, a double-carbapenem regimen has been reported to be an effective alternative therapy. Here, we describe an episode of sepsis in an immunocompromised patient after allogeneic hematopoietic stem cell transplantation, caused by an XDR-CPKP. Several in vitro synergy tests revealed a synergistic effect combining ertapenem and meropenem, which were used as combination therapy achieving clinical and microbiological success.
Introduction
I
Nowadays, retrospective studies have recommended combined therapy with more than one antibiotic.2,3 Recently, a double-carbapenem regimen (DCR) has been suggested as an alternative treatment against XDR-CPKP.4–6 However, there is scarce and no clear evidence of the effectiveness of combined therapy to treat CPKP infections in immunocompromised patients. 4 In the present report, we describe a case of sepsis caused by an XDR-CPKP in an immunocompromised patient after allogeneic hematopoietic stem cell transplantation (allo-HSCT). To evaluate the efficacy of combined antimicrobial therapy against the pathogen, we performed several in vitro synergy tests (Etest direct overlay, Etest cross [90° angle], checkerboard, and time-kill assays [TKA]). The results obtained support a synergistic effect combining ertapenem (ERT) and meropenem (MEM). Consequently, the patient was treated with a DCR, achieving clinical and microbiological success.
Case Report
Case description
In April 2015 a 36-year-old Spanish woman was diagnosed with myeloid sarcoma and rapidly underwent induction therapy (idarubicin/cytarabine). One month later, the patient underwent consolidation chemotherapy (high doses of cytarabine), achieving complete remission. In August 2015, the patient was admitted to the Vall d'Hebron University Hospital (Barcelona, Spain) to undergo allo-HSCT from an unrelated donor. Prophylaxis for infectious diseases included fluconazole, nebulized amphotericin, acyclovir, ciprofloxacin (CIP), and pentamidine.
The day of progenitor cell infusion the patient developed fever, dysuria, and neutropenic colitis (absolute neutrophil count 0 × 10E9/L) and empiric treatment with piperacillin/tazobactam and teicoplanin was started. On day 4 after progenitor cell infusion, she remained febrile and with dysuria. Blood cultures were negative, whereas the urine culture yielded an XDR K. pneumoniae (>10.000 CFU/ml) resistant to all β-lactams and susceptible only to gentamicin (MIC = 2 μg/ml) and colistin (MIC = 0.064 μg/ml) according to the European Committee on Antimicrobial Susceptibility Testing clinical breakpoints 7 (Table 1). Piperacillin/tazobactam was empirically replaced by amikacin and tigecycline (TGC), despite the susceptibility to these antibiotics not being initially evaluated. Twenty-four hours later the patient remained febrile and her clinical status worsened, presenting chills and hypotension. On day 6, blood cultures yielded the same microorganism, which was also isolated in rectal screening but not from central venous catheter cultures. Given the limited therapeutic options to treat this patient, combined antimicrobial therapy was considered.
Numbers in boldface indicate resistance values according to EUCAST, except for cefoxitin for which CLSI breakpoints were used since no value is reported in EUCAST guidelines.
EUCAST, European Committee on Antimicrobial Susceptibility Testing.
Strain characteristics and antimicrobial resistance determinants
The CPKP was screened for genes encoding carbapenemases (blaOXA-48, blaKPC, blaVIM, blaIMP, and blaNDM), ESBLs (blaTEM, blaSHV, and blaCTX-M), and plasmid-mediated AmpC, as well as quinolone and aminoglycoside resistance genes [aac(6′)-Ib/-cr, qnrA, qnrB, and qnrS] by PCR and sequencing, 8 showing that the isolate carried blaKPC-3, blaTEM-1, blaSHV-11, and aac(6′)-Ib-cr. PCR mapping showed that the blaKPC-3 gene was located in a Tn4401a transposon. 9 Moreover, characterization of the blaKPC-3-carrying plasmid was accomplished by Southern blot hybridization on S1-digested total DNA. PCR-based replicon typing and detection of plasmid addiction and partition systems (PAS/PPS) were also performed as previously described.10,11 The results showed that blaKPC-3 was located in an IncFIIk plasmid of 290 kb, which also carried three PAS (VagC-VagD, CcdA-CcdB, SrnB-SrnC) and one PPS (SopA-SopB). Finally, multilocus sequence typing, carried out as previously described, 8 revealed that the strain belonged to the epidemic KPC-producing K. pneumoniae ST258 clone.
Antimicrobial synergy tests
To evaluate the efficacy of combined antimicrobial therapy against this strain, in vitro synergy tests were done. The Etest synergy was performed by the MIC:MIC and cross methods using different strip combinations of ERT, imipenem (IPM), MEM, TGC, and CIP, as described previously. 12 The fractional inhibitory concentration (FIC) was calculated for each antibiotic in each combination. The total FIC (ΣFIC) for each compound was calculated as the sum of the FICs of the combined antimicrobials, considering synergy ΣFIC values ≤0.5 as stated previously.12,13 Synergistic effects were observed with IMP+MEM, IMP+ERT, and MEM+ERT combinations by the Etest MIC:MIC method, and with MEM+ERT combination by the Etest cross method, resulting in at least a fivefold decrease in the MIC of any of these antimicrobials (Table 2).
The mean ΣFIC was used for comparison between the Etest synergy methods and checkerboard: SYN (synergy) was defined as ΣFIC ≤0.5, IND (indifference) as ΣFIC >0.5–4, and ANT (antagonism) as >4.
ΣFIC, total fractional inhibitory concentration; ND, not determined.
Subsequently, the checkerboard synergy method (CBSM) and time-kill assay (TKA) were evaluated as described previously.12,14 For the CBSM, IPM+MEM, IPM+ERT, and MEM+ERT combinations were evaluated as these were the unique combinations for which synergy was observed in the MIC:MIC and/or cross methods. CBSM revealed that the lowest ΣFIC value (ΣFIC = 0.56) was obtained on combining 16 μg/ml ERT and 64 μg/ml MEM (Table 2). As for the MIC:MIC assay, the cross method and CBSM showed that MEM+ERT presented the best synergistic combination, TKA was hence evaluated for MEM and ERT alone and in combination at different concentrations. Each experiment was performed in triplicate. For the TKA, 300 μl aliquots were taken from each culture for bacterial count at five different time points (2, 4, 6, 8, and 24 hr). Bactericidal activity was defined as ≥99.9% reduction of the initial bacterial count at each time point. Synergy was defined as ≥2 log10 reduction of the initial bacterial count between the combination and the most active single agent tested at the same concentration after 24 hr. Bactericidal and synergistic activity was achieved for the 0.5 × MIC ERT plus 0.5 × MIC MEM combination at all time points, with a reduction in the bacterial inoculum of 6 log in the first 6 hr, with persistent bactericidal activity up to 24 hr (Fig. 1).
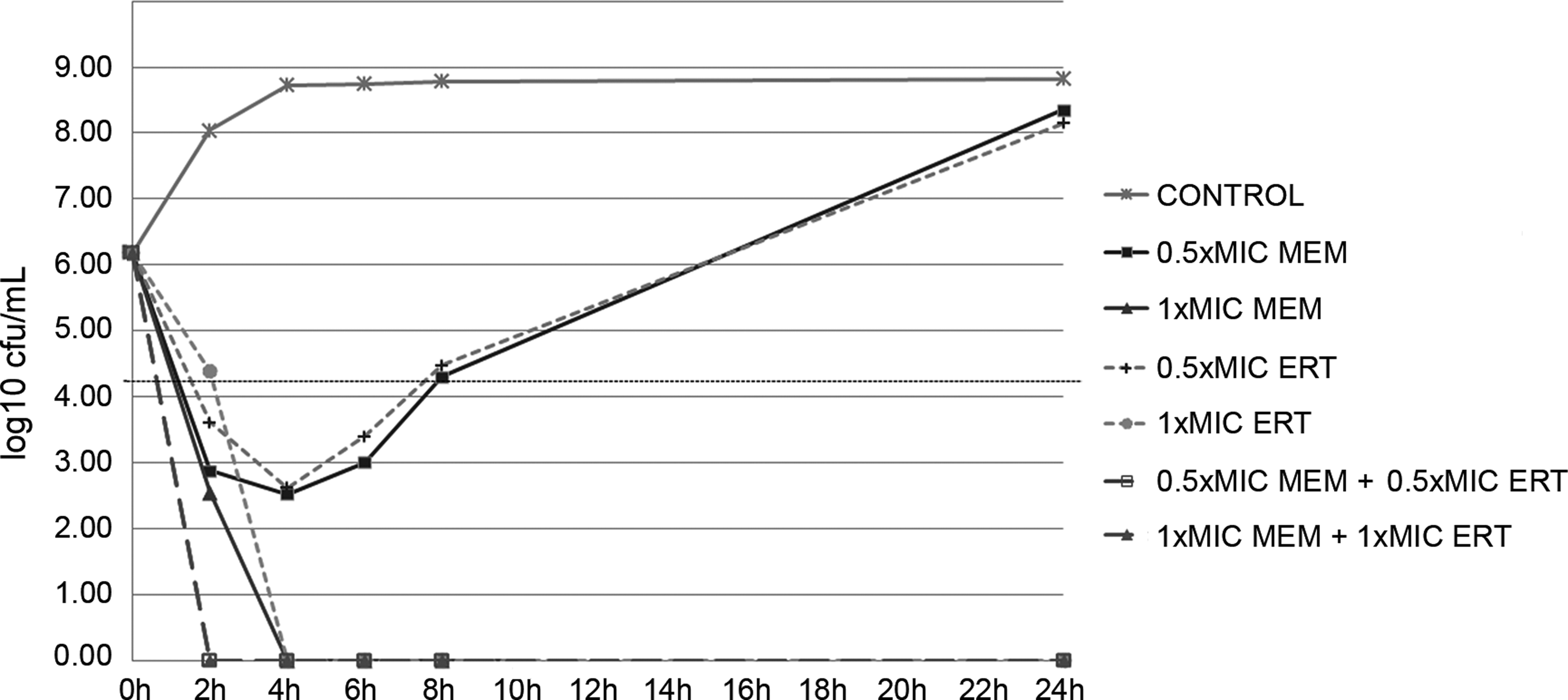
Time-killing assays for ERT and MEM alone and in combination at different concentrations. Synergy was defined as ≥2 log10 reduction of the initial bacterial count between the combination and the most active single agent tested at the same concentration after 24 hr. The broken horizontal line represents a reduction of 3 log10 CFU/ml compared with the initial bacterial count. ERT, ertapenem; MEM, meropenem.
Patient treatment and outcome
The patient was considered to be at high risk of potential antibiotic-induced nephrotoxicity (hemodynamic instability, neutropenia, early after allo-HSCT, and use of other nephrotoxic drugs). Accordingly, colistin and gentamicin were avoided. Due to a lack of alternative regimens, and based on synergy studies and previous success by other authors, DCR with ERT+MEM was started. Carbapenem dosage and posology was chosen according to previous reports4,6: ERT (1 g every 24 hr) was followed 1 hr later by a high dose of MEM (2 g every 8 hr, in extended 3-hr infusion) over 14 days, with no adverse effects. Fever abated in less than 48 hr, and urine and blood cultures became negative. The patient reached clinical and microbiologic success and was discharged 2 weeks later, with no infectious relapse during the following 3 months.
Discussion
Bloodstream infections caused by CPKP generally have a poor outcome, with a mortality of up to 65% in immunocompromised patients with hematologic malignancies.15,16 In these cases, a combination of two or more antibiotics is recommended.2,3,17 Recently, several authors have reported successful treatment of XDR-CPKP with the use of a DCR in clinical practice.4,6 The rationale is based on the higher affinity of carbapenemases for ERT, with a second carbapenem exerting bactericidal activity. Another explanation is that ERT reduces the bacterial load favoring the activity of the second compound. 18 Nonetheless, the efficacy of the DCR was shown to be lower in a neutropenic murine model. 19 In our case, the MEM+ERT combination showed the best synergistic activity. The novelty of our results highlights the effectiveness of this regimen in a severely immunocompromised patient. The treatment of infections caused by XDR-CPKP should be individually tailored and, based on in vitro synergistic tests, DCR could be considered, especially when only nephrotoxic drugs remain available.
Footnotes
Acknowledgments
This study was supported by the Ministerio de Economía y Competitividad, Instituto de Salud Carlos III, cofinanced by the European Regional Development Fund (ERDF) “A Way to Achieve Europe”, the Spanish Network for Research in Infectious Diseases (REIPI RD12/0015/0003), and the Spanish Ministry of Health (FIS PI15/00604 to JGL). N.P.-C. is financially supported by the REIPI RD12/0015/0003.
Disclosure Statement
No competing financial interests exist.