
Abstract
New Delhi MBL (NDM) carbapenemase-producing Klebsiella pneumoniae has become one of the most concerning multidrug-resistant pathogens. The Balkan counties are considered a reservoir for the spread of such strains based on several reports documenting NDM infections after hospitalization in this region. Nevertheless, NDM-producing K. pneumoniae have been only occasionally documented from Balkans. The current study documents the first polyclonal outbreak caused by NDM-1-producing K. pneumoniae in Bulgaria. From July 2015 to April 2016, all 25 single-patient carbapenem-nonsusceptible K. pneumoniae isolates were collected. Phenotypic and molecular screening revealed that 17 produced NDM-1 carbapenemase. All NDM-1 producers harbored blaCTX-M-15, blaCMY-4, blaTEM-1, and blaOXA-2; five also harbored blaOXA-1. In all cases, blaNDM-1 was flanked upstream by ISAba125 element and downstream by bleMBL. Pulsed-field gel electrophoresis (PFGE) clustered NDM-1-positive isolates into four distinct clonal types, A to D. MLST assigned isolates of the dominant clonal type A (n = 14) to sequence type (ST) 11, while isolates of clonal types B, C, and D to ST16, ST15, and ST391, respectively. Of interest, ST11 isolates belonged to the same PFGE type as those of the recently described NDM-1 ST11 clonal outbreak in Greece. Traveling abroad or overseas hospitalization was not reported in any case, suggesting most likely intra- and interhospital dissemination. The study presents the first polyclonal outbreak of NDM-producing K. pneumoniae in the Balkans and underlines the need for larger epidemiological studies in the region to illustrate commonalities in the transmission of NDM clones and possible sources in the community.
Background
C
A variety of acquired Ambler class A (e.g., KPC and GES enzymes), class B metallo-β-lactamase (MBL; e.g., VIM, IMP, and NDM enzymes), and class D carbapenemases (e.g., OXA-48-like enzymes) are increasingly recognized in Enterobacteriaceae and mostly in Klebsiella pneumoniae.2,3 Among the most recently emerged carbapenemases is the newly described New Delhi MBL-1 (NDM-1),4,5 and till now, 15 minor variants of NDM-1 (NDM-2 to −16) have also been identified (www.lahey.org/studies/other.asp). Since first reported in a K. pneumoniae clinical isolate in 2008, NDM-1 has become one of the most concerning carbapenemases since various human and biological factors have led to a large dissemination of blaNDM-1-producing strains, mainly K. pneumoniae and Escherichia coli.4,6,7 Several international surveillance studies have clearly shown that the primary source of NDM-producing clones is the Indian subcontinent.4,5,8,9 It is also evident that the blaNDM-1 gene occurs within the bacterial population in the Indian environment, with important implications in NDM-1 transmission to the community. 10
While most surveys have made a link with the Indian subcontinent, several studies have also documented the international transmission of NDM-producing isolates, involving movement of infected or colonized individuals from Middle East or Balkan countries to other regions.4,5,11,12 In particular, the Balkan region has been highlighted as a possible secondary source for the spread of NDM-positive bacteria, mainly K. pneumoniae, based on several reports from different European countries documenting infections due to NDM-1-possessing pathogens, following previous hospitalization in the Balkan States.5,11,13,14 However, despite this strong evidence, NDM-1-producing K. pneumoniae strains have been only occasionally documented from Balkan countries such as Bulgaria, Croatia, Romania, and Turkey,15–17 and only a clonal outbreak caused by an NDM-1-producing K. pneumoniae sequence type (ST) 11 strain has been described in Greece. 18 Therefore, more evidence is needed to corroborate the hypotheses that the Balkan region is a source of NDM-producing K. pneumoniae clones.
In the Military Medical Academy (MMA), Sofia, carbapenem-resistant K. pneumoniae strains possessing class A carbapenemases were sporadically detected until mid-2015. However, in July 2015, preliminary susceptibility data and phenotypic tests showed the introduction of carbapenem-resistant K. pneumoniae strains that were phenotypically positive for MBL production. This prompted the initiation of a survey to investigate the first outbreak in Bulgaria caused by NDM-1-producing K. pneumoniae.
Materials and Methods
Bacterial isolates and patients
MMA is a large medical complex in Sofia with ∼800 beds. From July 2015 to April 2016, initiated with the identification of the first phenotypically MBL-positive isolate, all nonrepetitive single-patient K. pneumoniae isolates with reduced susceptibility to at least one carbapenem (ertapenem MIC ≥1 μg/ml, meropenem, and/or imipenem MIC ≥4 μg/ml) were collected for further investigation. Following identification and confirmation of NDM carbapenemase production, patients' records were retrospectively assessed for demographic characteristics, medical and travel history, previous antibiotic consumption, underlying diseases, and prior hospitalization.
Bacterial identification, susceptibility testing, and phenotypic assays
Microbial identification was performed with the Vitek 2 automated system (bioMérieux, Marcy l'Étoile, France) and confirmed with the API 20E system (bioMérieux). Susceptibility testing to various antimicrobials was determined by Vitek 2 and results were interpreted according to European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. 19 Carbapenem and tigecycline susceptibility testing was also performed by Etest (bioMérieux). 19 A combined-disk test with meropenem as a substrate without and with phenylboronic acid, EDTA, or both inhibitors was used to screen for class A and B carbapenemase production. 20 Possible coproduction of extended-spectrum β-lactamases (ESBLs) was screened with the modified CLSI ESBL confirmatory test. 21
Polymerase chain reaction amplifications and sequencing
Polymerase chain reaction (PCR) single reactions were used to investigate the presence of Ambler class A, B, and D carbapenemase genes and genes encoding OXA-1 and OXA-2, 16S RNA methylases, plasmid-mediated AmpCs, and ESBLs, including the SHV, TEM, IBC/GES, and CTX-M enzymes.14,18,20,21 Primers NDM-F (5′-GGG CAG TCG CTT CCA ACG GT-3′) and NDM-R (5′-GTA GTG CTC AGT GTC GGC AT-3′) were used to screen for detection of the blaNDM gene. 18 blaNDM-positive isolates were also screened for the presence of the ISAba125 element and the bleomycin resistance gene bleMBL, and mapping of the blaNDM surrounding environment was performed using specific primers. 22 PCR products were subjected to direct sequencing.
Molecular typing
Molecular fingerprinting was performed by pulsed-field gel electrophoresis (PFGE) analysis of XbaI-digested whole genomic DNA using the CHEF-DR III system (Bio-Rad, Hemel Hempstead, United Kingdom), with pulse times ranging from 5 to 37 s and run time of 23 hrs. PFGE patterns were analyzed and compared visually following criteria previously described. 23 Multilocus sequence typing (MLST) was performed on representative isolates by PCR amplification of the seven housekeeping genes using primer sequences described in the K. pneumoniae MLST database (Institute Pasteur MLST Database website). STs were assigned using online database tools.
Conjugation experiments and plasmid analysis
Potential conjugation transfer of carbapenem resistance was investigated. Conjugational experiments were carried out with E. coli strain 26R793 (lac−, RifR) as the recipient strain. Isolates that harbored the blaNDM-1 and blaOXA-1 genes were selected and used. Donor and recipient cells from Luria-Bertani broth cultures were mixed in a ratio of 1: 5 and transconjugant clones were screened on MacConkey agar plates containing rifampicin (100 μg/ml) and amoxicillin (100 μg/ml) or ertapenem (0.25 μg/ml). Conjugation events were studied at both 30°C and 37°C. 24 All β-lactamase genes were sought by PCR amplification. Plasmid DNA was isolated from 50 ml overnight cultures of both donor and transconjugant strains using a Plasmid Midi Kit (Macherey-Nagel, Düren, Germany) according to the manufacturer's protocol. E. coli 39R861 was used as a plasmid size standard for comparison. Plasmid incompatibility groups were identified by using the PCR-based replicon-typing scheme as previously described. 25
Results
NDM-positive clinical isolates and patients' characteristics
During the survey period, 25 single-patient K. pneumoniae clinical isolates with reduced susceptibility to at least 1 carbapenem were collected in MMA. Initial phenotypic screening by combined-disk test showed that 17 isolates produced an MBL and the remaining 8 produced a class A carbapenemase. Further investigation with PCR assays and sequencing confirmed that all 17 presumably MBL-positive isolates possessed NDM-1 carbapenemase, while a blaNDM allele was not amplified in any of the other carbapenem-nonsusceptible isolates. Patients infected or colonized with NDM-1 producers were hospitalized in six different hospital units, mainly in the intensive care, ambulatory, and anesthesiology and resuscitation units. The most common source of isolation from which NDM-1 pathogens were isolated was urine, followed by bronchial secretion, intra-abdominal abscess, blood, and surgical wound (Table 1). In all but one case, treatment with β-lactam antibiotics before NDM-1-possessing isolation was reported. Underlying diseases were identified in all patients, and death attributed to NDM-1 infection was the outcome in five cases.
Index patient.
AMB, ambulatory unit; ARC, anesthesiology and resuscitation unit; GAS, gastroenterology unit; HPS, hepato-pancreatic surgery unit; ICU, intensive care unit; MBL, metallo-β-lactamase; MLST, multilocus sequence typing; NDM-1, New Delhi MBL-1; PFGE, pulsed-field gel electrophoresis; ST, sequence type; URO, urology clinic.
Description of the outbreak and infection control measures
Before the first NDM-1 isolation, there had been no report of MBL-producing K. pneumoniae isolates in the hospital over the preceding 6 months. Therefore, the index NDM-1-possessing outbreak isolate is considered as the one that was harvested from patient 1 in July 2015 (Table 1). The index K. pneumoniae was retrieved from an abscess sample of a female patient, with no history of traveling abroad, on the second day of her hospitalization in the hepatopancreatic surgery ward. The woman suffered from peritonitis and she was recently hospitalized in another hospital, possibly implicating introduction of the NDM-1-producing clone in our hospital, even though active screening samples were not taken upon admission. The patient condition improved after treatment.
It is of note that in three additional NDM-1 cases, the clinical specimens were collected within 48 hrs after their admission and this may suggest that not only intrahospital but also interhospital dissemination or community acquisition contributed to this outbreak. Moreover, medical history revealed that three of the four patients with community-onset infections were hospitalized over the preceding 3 months, while the remaining patient had no history of prior hospitalization or exposure to healthcare facilities and the case was considered as community-acquired.
Prior hospitalization of patients harboring NDM enzymes was established in total in five cases; however, there were no active screening samples requested upon admission and thus a possible importation of NDM-1-producing strains from other hospitals could not be confirmed. Traveling abroad or overseas hospitalization was not reported in any case, adding to the previous assumption that intrahospital dissemination and interhospital dissemination were the main transmission routes of the outbreak.
After detection of the first cases in July 2015, the standard infection control procedures were reinforced. Thus, additional precautions were taken, including frequent hand hygiene audits, educational session at the ward level, microbiological investigation of healthcare personnel, equipment, and hospital environment, additional disinfection in affected units, and patients' cohorting or isolation when available. The implementation of these measures was followed by the absence of new NDM-1 cases during August to September 2015. However, in October 2015, NDM-1-producing clonal strains reemerged in several hospital units, possibly suggesting lower compliance with reinforced infection control measures (Table 1 and Fig. 1). In addition, although additional infection control practices were taken, carbapenem-resistant MBL-positive K. pneumoniae clinical isolates were still sporadically recovered after the end of the current investigation (data not shown).
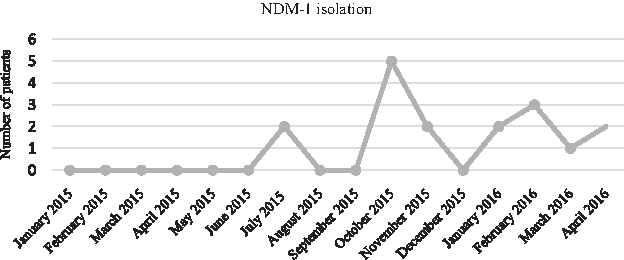
Schematic presentation of the identification of NDM-1-producing Klebsiella pneumoniae isolates during the study period. NDM-1, New Delhi MBL-1.
Susceptibility testing
Susceptibly testing showed that all NDM-positive K. pneumoniae were resistant to β-lactam antibiotics, including cefoxitin, cefotaxime, ceftriaxone, ceftazidime, cefepime, and piperacillin/tazobactam, as well as to aztreonam, suggesting the presence of additional β-lactamases in all cases. All isolates exhibited resistance to carbapenems (imipenem MICs 12 to >32 μg/ml, meropenem MICs 8 to >32 μg/ml, and ertapenem MICs 12 to >32 μg/ml), except two that were intermediate susceptible to imipenem and meropenem (MIC 4 μg/ml). Different susceptibilities were observed for amikacin, gentamicin, and trimethoprim/sulfamethoxazole, while all isolates were resistant to ciprofloxacin. One isolate was found resistant to colistin (further investigation revealed the absence of the mcr-1 gene). Finally, seven isolates were susceptible to tigecycline (MICs 0.5–1 μg/ml), six intermediate (MICs 2 μg/ml), and the remaining four were resistant (MICs 3–16 μg/ml).
Phenotyping and molecular testing
Phenotypic testing by the modified CLSI ESBL confirmatory test showed in all cases the coproduction of an ESBL enzyme. Screening by PCR and sequencing analysis confirmed that all 17 blaNDM-1-possessing isolates harbored blaCTX-M-15 ESBL. All isolates also harbored blaCMY-4 AmpC, blaTEM-1, and blaOXA-2 genes; in addition, five of them contained the blaOXA-1 gene. 16S RNA methylase production was not detected in any of the isolates. Furthermore, DNA amplification followed by sequencing showed that in all cases, the blaNDM-1 gene was flanked upstream by a nontruncated ISAba125 element and downstream by the bleMBL gene.
PFGE and MLST typing
PFGE analysis clustered the 17 NDM-1-possessing isolates into four distinct clonal types, A to D, which differed from clonal types detected among the remaining carbapenem-nonsusceptible isolates of the study period (Fig. 2). The majority of NDM-1 producers (n = 14) belonged to clonal type A, while single isolates were assigned to the remaining clonal types (Table 1). The dominant clone was observed in 2015 and remained prevalent throughout the whole period of investigation. Clonal type B was observed also in 2015, while clonal types C and D were observed in 2016.
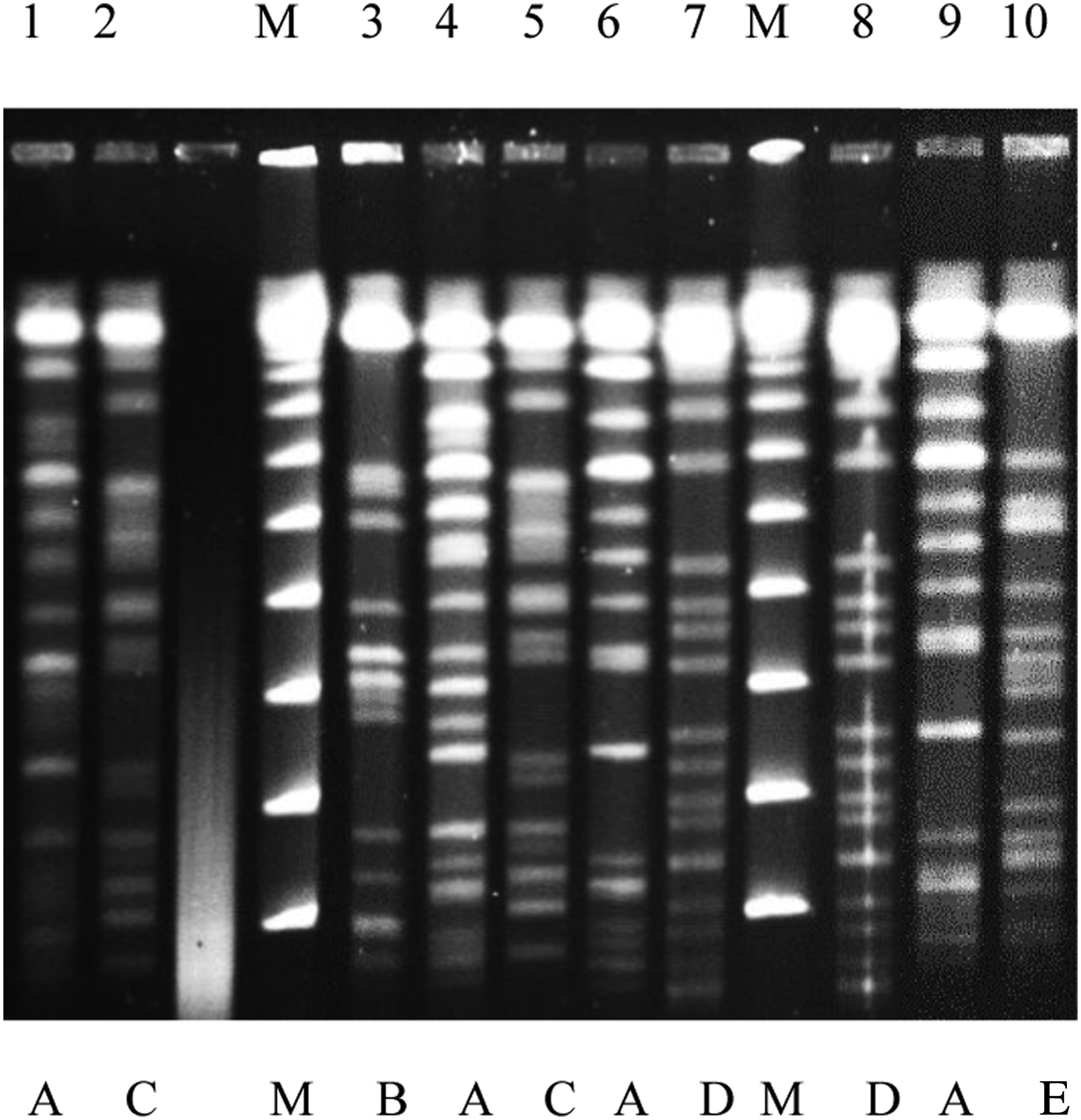
Representative PFGE clonal types of XbaI-digested genomic DNA of K. pneumoniae isolates. Lanes 1, 2, and 3–7: NDM-1-producing K. pneumoniae isolates of the current outbreak belonging to the four clonal types (A to D); Lane 8: PFGE pattern deriving from a different gel plug of the same isolate as in lane 7; Lane 9: Representative NDM-1-producing K. pneumoniae isolate of the ST11 clonal type A Greek outbreak (Ref. 17); Lane 10: non-NDM-1-producing K. pneumoniae isolate recovered in Military Medical Academy (clonal type E).; Lane M: multimers of phage lambda DNA (48.5 kb) molecular mass ladder. PFGE, pulsed-field gel electrophoresis; ST, sequence type.
MLST typing of NDM-1-positive isolates revealed four distinct STs. The isolates belonging to the dominant PFGE clonal type A were assigned to MLST type ST11, a single-locus variant of the pandemic clone ST258. 2 The isolates of clonal type B were assigned to ST16, while that of clonal type C to ST15 and that of clonal type D to ST391. It is of note that ST11 isolates of the current outbreak belonged to the same PFGE clonal type (A) as those of the recently described NDM-1 ST11 clonal outbreak in Greece (Fig. 2). 18
Plasmid analysis
Conjugational experiments were able to transfer at 37°C and, at a very low rate, (∼10−7) carbapenem resistance in representative isolates of clonal types A and B, but not of clonal types C and D. Analysis of the selected transconjugants proved that they acquired the blaNDM-1 gene along with blaCTX-15 and blaCMY-4 genes. In both cases, resistance to aminoglycosides was also transferred. Downstream plasmid analysis indicated the presence of ∼100 kb plasmids belonging to the incompatibility groups IncA/C and IncL/M, respectively.
Discussion
The ongoing emergence of NDM-producing Enterobacteriaceae remains a disturbing fact. Since its rise in the Indian subcontinent, NDM carbapenemase has achieved worldwide dissemination. 6 Several reports have shown the dissemination of such isolates in Europe, North and South America, Asia, Australia, New Zealand, and the Middle East.1,3,4,9,11,12 In the European region, outbreaks of NDM-producing Enterobacteriaceae remain restricted and uncommon26–28 with reports of an incremental spread initially not only from Sweden and the United Kingdom but also from countries such as Austria, Belgium, France, Germany, Switzerland, the Netherlands, and Norway.1,6,9,29,30
In the Balkan Peninsula, the sporadic appearance of NDM-1-producing K. pneumoniae has been also described and a large clonal outbreak was documented in a single Greek hospital.15,17,18,31 In addition, the region has been highlighted as a secondary reservoir for the spread of NDM-producing K. pneumoniae to other European countries due to cross-border transfer of patients.4,5,11,13,14,32,33 The introduction of these clones in the Balkan countries is still debatable; however, studies commenting on epidemiological characteristics of NDM-1 in the Balkans have suggested that introduction of NDM producers to the Balkans is linked to travel for medical care in the Indian subcontinent.11,13
Until 2012, the only NDM-producing pathogens recognized in Bulgaria were E. coli isolates, 34 while recently four sporadic cases of K. pneumoniae harboring NDM-1 from different hospitals settings have been also reported.16,35 Our study describes the first outbreak of NDM-producing K. pneumoniae isolates in a tertiary care hospital in Bulgaria. The outbreak patients were hospitalized in several different units of the hospital, but a crossover transmission between patients was not established. Environmental and air sampling that was undertaken during the survey was also not able to link patient cases with environmental contamination. However, the retrieval of most NDM pathogens at least 3 days following hospital admission and the overlapping periods of hospitalization noted possibly suggest that intrahospital dissemination was the main route. Moreover, in some NDM-1 cases, clinical samples were collected within 48 hrs after their admission and this may suggest that interhospital dissemination or community acquisition may have contributed to this outbreak. However, since active surveillance was not undertaken, a possible importation of such strains was not established. As with the four sporadic Bulgarian NDM-producing K. pneumoniae isolates,16,35 the same ST11 was identified as the predominant clonal lineage in the current outbreak. Of great interest, our ST11 PFGE clonal type A was found to be identical to the one that caused the large outbreak in Greece, 18 indicating that this clone is widely disseminated and possibly underestimated in the Balkan countries. Nevertheless, incompatibility grouping of NDM-1 plasmids showed that different plasmids belonging to different groups have been transferred into the Greek and Bulgarian sublineages. This is opposite to the interspecies transfer of the same resistance plasmid documented recently on an NDM-1-producing K. pneumoniae outbreak in the Netherlands. 26
NDM-1-producing ST11 K. pneumoniae clones have also been reported in several European countries, United States, South America, Australia, New Zealand, India, Thailand, China, and United Arab Emirates, giving further confirmation to the scenario of dissemination and establishment of this successful clonal lineage.6,29,36–39 Especially, in the Balkan States, this lineage has been detected only in Bulgaria and Greece,16,18,35 suggesting that the clone is disseminated in these two particular Balkan countries. Regarding our less commonly identified STs—ST15 and ST16—they have been also repeatedly detected in the Indian subcontinent and other regions8,39; they have been also associated with NDM cases following previous hospitalization in Serbia, Montenegro, and Croatia,17,33 implicating that these clones are widely spread in the Balkan Peninsula. Finally, our NDM-1 ST391 clone has been detected previously only in a single case from the Indian subcontinent 8 and this further supports the assumption that NDM clones have been introduced in Balkans through medical tourism or migration from the Indian subcontinent.11,13
In summary, our study presents the first polyclonal outbreak of NDM-producing K. pneumoniae isolates in the Balkan States. The same dominant clone has been circulating in the Balkan region since 2011; however, in the current survey, three additional clonal types were detected. This may suggest a difference from the situation described in Greece 18 as additional NDM clonal lineages have been introduced in Bulgarian hospitals. This also underlines the significance of consistent surveillance of NDM-producing isolates at the local level as well as the need for larger epidemiological studies in the Balkan region to illustrate commonalities in the transmission of NDM K. pneumoniae clones and possible sources in the community.
Footnotes
Acknowledgment
This study was supported by internal funding.
Disclosure Statement
No competing financial interests exist.