
Abstract
Aims:
We aimed to develop a simple scoring system to predict risk for methicillin resistance in community-onset Staphylococcus aureus bacteremia (CO-SAB) by identifying the clinical and epidemiological risk factors for community-onset methicillin-resistant S. aureus (MRSA).
Methods:
We retrospectively analyzed data from three multicenter cohort studies in Korea in which patient information was prospectively collected and risk factors for methicillin resistance in CO-SAB were identified. We then developed and validated a risk-scoring system.
Results:
To analyze the 1,802 cases of CO-SAB, we included the four most powerful predictors of methicillin resistance that we identified in the scoring system: underlying hematologic disease (−1 point), endovascular infection as the primary site of infection (−1 point), history of hospitalization or surgery in ≤1 year (+0.5 points), and previous isolation of MRSA in ≤6 months (+1.5 points). With this scoring system, cases were classified into low (less than −0.5), intermediate (−0.5–1.5), and high (≥1.5) risk groups. The proportions of MRSA cases in each group were 24.7% (22/89), 39.0% (607/1,557), and 78.8% (123/156), respectively, and 16.7% (1/6), 33.8% (112/331), and 76.9% (10/13) in a validation set.
Conclusions:
This risk-scoring system for methicillin resistance in CO-SAB may help physicians select appropriate empirical antibiotics more quickly.
Introduction
S
CO-MRSA infections can be classified into healthcare-associated (HA) and community-associated (CA) infections according to the presence of risk factors for MRSA acquisition: history of hospitalization, surgery, dialysis, or residence in a long-term care facility within 1 year of the MRSA culture date; presence of an indwelling catheter or percutaneous device at the time of culture; and previous isolation of MRSA.12,13 CA-MRSA has emerged in North America and Europe, and distinctive clinical factors of CA-MRSA have also been identified in previous studies.14–16 There have been attempts to develop tools for predicting methicillin resistance in CO invasive S. aureus infections based on these risk factors, but the tools had low sensitivity and specificity.17–21
CA-MRSA infections are less common in Korea than in North America, and HA-MRSA clones circulate more frequently in the community. 5 Because of this difference in molecular epidemiology, the risk factors for methicillin resistance in CO S. aureus infections in Korea will not be same as those in North America. We, therefore, investigated the clinical and epidemiological factors associated with methicillin resistance in CO S. aureus bacteremia (CO-SAB), and developed and validated a simple clinical scoring system for predicting methicillin resistance.
Materials and Methods
Study design and patients
This retrospective cohort study used data from three multicenter cohorts of invasive S. aureus infections in Korea obtained using a similar study design: (1) a prospective cohort from July 2009 to June 2011 at 9 hospitals, 4 (2) a prospective cohort from May to December 2012 at 16 hospitals, 5 and (3) a prospective cohort from September 2013 to March 2015 at 10 hospitals. 22 For validation, we collected additional patient data from April 2015 to March 2017, which was included as a last cohort. All studies were conducted with a standardized protocol and the institutions of the Korea INfectious Diseases (KIND) study group participated as much as possible. The individual authors and affiliations within this group are listed in the acknowledgments section.
CO-SAB was defined when S. aureus was isolated from blood cultures within 48 hr of hospitalization or in the emergency room. 13 Infectious diseases specialists at each hospital checked the results of blood cultures routinely. When repeated blood cultures were positive in the same patient during the study period, only the first case was included. Patients who were discharged or died before the results of blood culture tests were available were excluded because we were unable to obtain the relevant information. Clinical and epidemiological information was collected by trained research nurses or infectious diseases specialists, and assessed for the following potential risk factors for MRSA infection: age, sex, underlying illness, primary site of infection, history of recent hospitalization or surgery, long-term care facility, indwelling device, dialysis, previous isolation of MRSA, acupuncture, and steroid or immunosuppressant use. To take into account comorbid conditions, Charlson's weighted index of comorbidity (WIC) was calculated. 23 The primary sites of SAB were established according to the best judgment of an infectious diseases specialist at each hospital as follows: catheter-related infection, pneumonia, skin and soft tissue infection (SSTI), bone and joint infection (BJI), endovascular infection (endocarditis, mycotic aneurysm, septic thrombophlebitis and infected implanted vascular device such as graft infection or arteriovenous fistula), intra-abdominal infection, urinary tract infection (UTI), central nervous system infection, other, and bacteremia of unknown primary focus. All the data were additionally reviewed by two infectious diseases specialists in Seoul National University Bundang Hospital.
This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital.
Statistical analysis
Univariate analysis was performed to test for differences between groups. We used Student's t-test and the chi-square test or Fisher's exact test, depending on the type of variable. For multivariate analysis, potential covariates with p-values <0.10 in the univariate analyses were included.
Multivariate logistic regression models were tested with adjustment for covariates. Adjusted odds ratios (aORs) and their 95% confidence intervals (CIs) were calculated, and p-values <0.05 were considered statistically significant. Charlson's WIC was excluded from multivariate analyses because of multicollinearity with other underlying illnesses. The risk-scoring system was based on the beta coefficients in the logistic regression model. All statistical analyses were performed with IBM SPSS Statistics, version 22.0 (IBM Corp., Armonk, NY).
Results
A total of 1,802 cases of CO-SAB (716, 516, and 570 cases, respectively) were included, 752 (41.7%) of whom were MRSA infections. The mean age was 62 years, and 53.6% (968/1,802) of the patients were male. Bone and joints were the most common identifiable primary sites of infection. The mean Charlson's WICs of the three cohorts (see Study design and patients section) were 3.0 ± 2.7, 2.4 ± 2.3, 2.1 ± 2.2, and 4.6 ± 2.9, respectively, with relatively higher value of WIC in the third cohort. A total of 39.1% (691/1,766) of the patients had histories of hospitalization or surgery within the previous year, and 24.6% (425/1,727) of the patients had history of residence in a long-term care facility within the previous year.
The clinical and epidemiological factors associated with methicillin resistance in CO-SAB were identified by univariate analysis (Tables 1 and 2). Older age (≥65 years), presence of renal disease, solid tumor, cerebrovascular disease, chronic pulmonary diseases, peptic ulcer diseases as underlying illnesses, Charlson's WIC ≥3, catheter-related infection, and UTI were risk factors for methicillin resistance in univariate analysis (Table 1). In contrast, presence of hematologic disease as underlying illnesses, SSTIs, and BJIs were significantly more frequent among MSSA infections. The risk of MRSA infections was increased in patients with HA risk factors such as history of hospitalization, surgery, dialysis, or residence in a long-term care facility within the previous year; presence of an indwelling catheter or percutaneous device; and a history of isolation of MRSA within the previous 6 months (Table 2).
There are some missing data.
Others include ocular infection, mediastinal infection, and ostitis.
AIDS, acquired immune deficiency syndrome; BJI, bone and joint infection; CNS, central nervous system; IAI, intra-abdominal infection; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-susceptible S. aureus; SSI, surgical site infection; SSTI, skin and soft tissue infection; UTI, urinary tract infection; WIC, weighted index of comorbidity.
Within past 1 year.
Some data were missing.
Within 6 months.
In a multivariate regression model, the risk factors for MRSA infection in CO-SAB were older age ((aOR, 1.70; 95% CI, 1.41–2.06), history of hospitalization or surgery (aOR 2.05; 95% CI 1.64–2.56), residence in a long-term care facility (aOR 1.68; 95% CI 1.30–2.17), and dialysis (aOR 1.48; 95% CI 1.08–2.02) within ≤1 year, and history of previous isolation of MRSA (aOR 4.46; 95% CI 2.97–6.68) within ≤6 months. In contrast, MRSA bacteremia patients had less hematologic disease (aOR 0.45; 95% CI 0.23–0.85), and their primary infections were less frequently SSTIs (aOR 0.57; 95% CI 0.41–0.79), BJIs (aOR 0.65; 95% CI 0.48–0.88), and endovascular infections (aOR 0.46; 95% CI 0.26–0.79).
To develop the scoring system, we chose the four most powerful predictors and allocated them points: underlying hematologic disease (−1 point), endovascular infection as primary infection (−1 point), hospitalization or surgery within ≤1 year (+0.5 points), and history of previous isolation of MRSA within ≤6 months (+1.5 points) (Table 3). We classified the risk of MRSA bacteremia according to the total score, which ranged from −2 to +2 points, into low (score < −0.5), intermediate (−0.5 ≤ score <1.5), and high (score ≥1.5). The proportions of MRSA in each group were 24.7% (22/89), 39.0% (607/1,557), and 78.8% (123/156), respectively (Fig. 1).
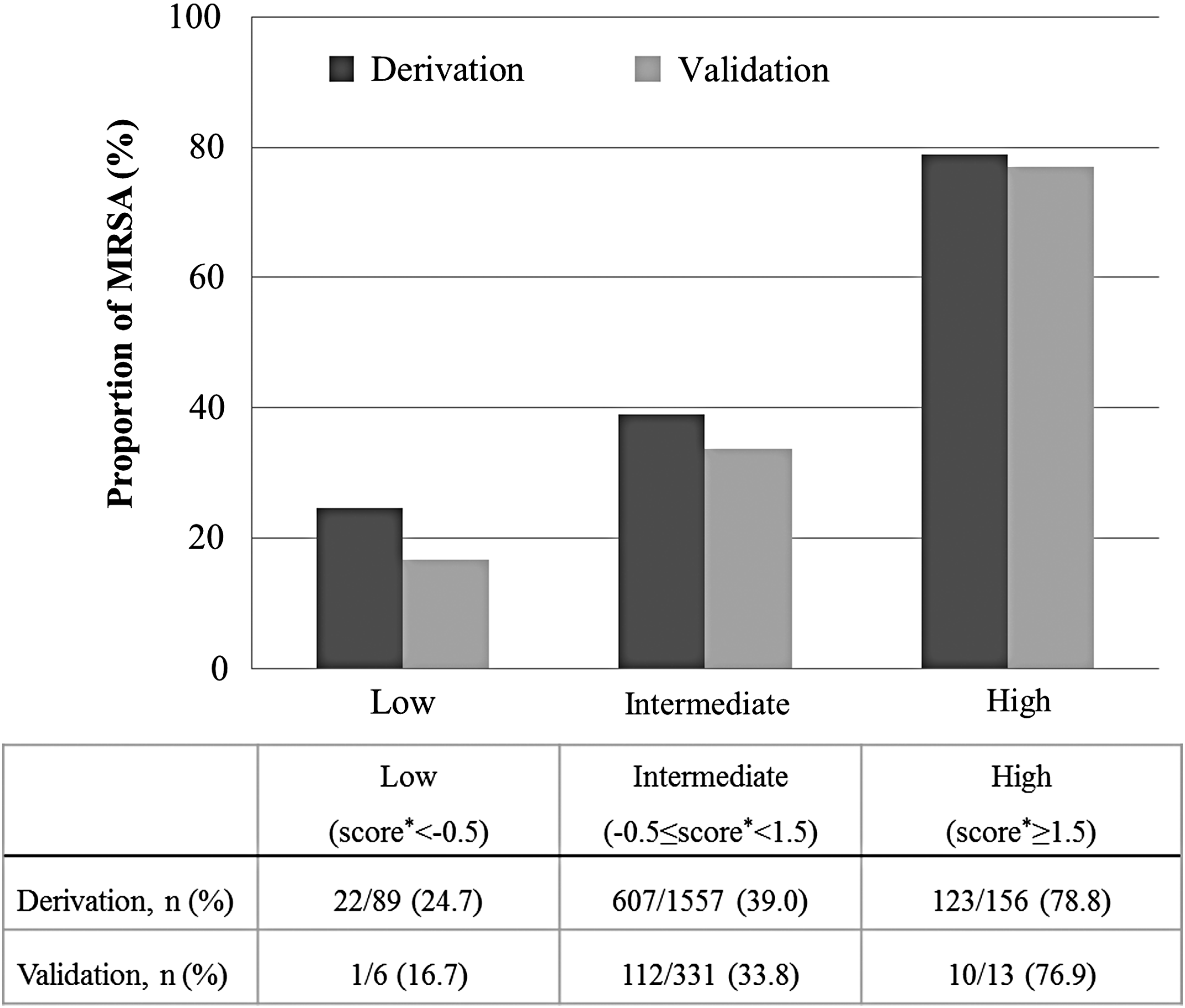
The proportion of MRSA among community-onset Staphylococcus aureus bacteremia patients in each risk group. *The score ranged from −2 to +2 points. MRSA, methicillin-resistant S. aureus.
Within past 1 year.
Within 6 months.
In addition, a total of 350 patients were enrolled in the validation set, 35.1% (123/350) of which were MRSA infections. In this set, the proportions of MRSA in each group were 16.7% (1/6), 33.8% (112/331), and 76.9% (10/13), respectively (Fig. 1).
Discussion
Of the 1,802 patients with CO-SAB, 752 (41.7%) had MRSA infections. In the three cohorts of CO-SAB cases enrolled at different times between 2009 and 2015, the proportions of CO-MRSA infections were 42.3% (303/716) in the cohort from 2009 to 2011, 45.3% (234/516) in the cohort in 2012, and 37.7% (215/570) in the cohort from 2013 to 2015. The proportions of CA-MRSA infections among the CO-SABs were 11.3% (81/716), 10.1% (52/516), and 8.8% (50/570), respectively, with no significant difference between them. These proportions were higher than in our survey of CA-MRSA infections in 2005, 24 and there are other studies that suggest that CA-MRSA infections are increasing in Korea.5,24–26 However, the proportion of CA-MRSA infections has not been increasing rapidly according to these large scale studies.
Currently, we do not recommend routine use of MRSA-targeting antibiotics as initial empirical therapy for patients with CO infections in Korea. 27 However, there are no local practical guidelines concerning the possibility of methicillin resistance among CO-SABs. In multilocus sequence typing analysis of CA-MRSA, the most common sequence type in Korea was ST72 (USA700), but ST5 (USA100) and ST239, which are generally found among HA MRSAs, were also circulating widely in the community.24,28 This suggested that the boundary between community and healthcare settings is sometimes unclear. Hence, by analyzing a large number of prospectively and systematically collected multicenter CO-SAB cases, we hoped to develop a simple clinical and epidemiological risk factor-based system for predicting methicillin resistance in cases of CO-SAB in Korea.
In this study, we identified several risk factors for methicillin resistance that were different from those identified in studies in other countries. In our case, the risk of MRSA was higher in the elderly, whereas the corresponding results in previous studies were inconsistent: some reported results similar to this study, 29 others suggested that the risk was not related to age14,30,31 or even that lower age was associated with increased risk of MRSA.18,19 These disparities may reflect cultural differences. For example, there is a unique caregiver culture involving family members in Korea, and it is common for the elderly to be main caregivers. Hematologic diseases were also more likely to be non-MRSA in another study, but this effect was not statistically significant. 18 In addition, SSTIs, BJIs, and endovascular infections were more likely to be due to MSSA in our study, whereas other studies found that these factors had less impact or were unrelated to MSSA infections.19,30,31 In particular, SSTI was found to be associated with CO-MRSA in North America. 32 Because of these diverse results, the relationships between specific underlying illnesses or primary sites of infection and methicillin resistance observed in this study should not be generalized, and further studies are needed.
We classified the risk of MRSA in the CO-SABs as low, intermediate, or high using a simple scoring system. As a result, in both the derivation set and the validation set, the frequency of MRSA infections was <25% in the low-risk group and >75% in the high-risk group. This scoring system could be helpful for determining the initial choice of MRSA-targeted antibiotic when SAB is suspected in the early course of hospitalization of patients. If there is a high score (≥1.5 points) in this scoring system, administration of empirical MRSA-targeted antibiotics may be considered, whereas they can be deferred in cases with low probabilities of MRSA infection. Although empirical MRSA-targeted antibiotics can be permitted in severe cases, this policy should allow an adequate choice of empirical antibiotic in CO-SAB cases, in terms of both appropriateness of antibiotic spectrum and avoidance of unnecessary antibiotic use.
This study has several limitations. First, the data were analyzed retrospectively; they were collected from three different studies, and there might be some heterogeneity including comorbidities among the patients participating in those studies. Although each study was prospective with a similar design, and ∼40% of the hospitals contributed to at least two of the cohorts, this heterogeneity could bias the results. Second, since we used three cohorts for 8 years, epidemiological changes may have affected our results. Third, since we targeted SAB, the results could be different from those obtained for invasive S. aureus infections. SSTIs, especially, are difficult to grow in blood culture, so caution is needed in interpreting the results. In addition, not all patients were evaluated for endovascular infections using transthoracic or transesophageal echocardiography, so endovascular infections could be underestimated. Fourth, although we tried to construct an effective system for analyzing risk, substantial number of patients fell into the intermediate-risk group. Hence, additional early detection techniques such as polymerase chain reaction, which can detect antibiotic susceptibility, are needed. Fifth, since only Korean hospitals participated in this study, the results may not be applicable to other countries with different clinical and epidemiological situation. Finally, there were some missing values for several factors, which reduced statistical significance. However, we included a large number of cases, and most of the factors with large number of missing values did not have statistically significant effects on risk in the univariate analysis and were not included in the multivariate analysis.
In conclusion, we have developed a simple clinical risk-scoring system to predict methicillin resistance in CO-SAB, and have stratified cases into low-, intermediate-, and high-risk groups. This stratification according to a scoring system based on clinical and epidemiological risk factors may help physicians identify appropriate empirical antibiotics early in the course of CO-SAB.
Footnotes
Acknowledgments
We thank the members of the KIND study group and associated staff for their cooperation in this study. The collaborators in the KIND Study Group were Taek Soo Kim, Sue Shin, Kyoung Un Park, and Eui-Chong Kim, Department of Laboratory Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea; Shinhye Cheon, Nak-Hyun Kim, and Wan Beom Park, Department of Internal Medicine, Seoul National University Hospital, Seoul, Republic of Korea; Sun Hee Lee, Department of Internal Medicine, Pusan National University Hospital, Busan, Republic of Korea; Ki Tae Kwon, Department of Internal Medicine, Daegu Fatima Hospital, Daegu, Republic of Korea; Chisook Moon, Department of Internal Medicine, Inje University College of Medicine, Busan, Republic of Korea; Ji Hwan Bang and Sang Won Park, Division of Infectious Diseases, Seoul Metropolitan Government—Seoul National University Boramae Medical Center, Seoul, Republic of Korea; Hee Jung Choi, Department of Internal Medicine, Ewha Womans University, School of Medicine, Seoul, Republic of Korea; Eun Jung Lee, Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Seoul, Republic of Korea; Eun Ju Choo, Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Bucheon, Republic of Korea; Yeong Keun Kim, Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea; Min Hyok Jeon, Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Cheonan, Republic of Korea; Jeong-Hwan Hwang and Chang-Seop Lee, Department of Internal Medicine, Chonbuk National University Medical School, Jeonju, Republic of Korea; and Hee-Chang Jang, Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Republic Korea.
This study was performed using data from three multicenter cohorts. The first cohort from July 2009 to June 2011 was supported by grant No. 2009-E00609-00 from the Korea Centers for Disease Control and Prevention. The second cohort from May to December 2012 was supported by grant No. 2012-E44003-00 from the Korea Centers for Disease Control and Prevention. The last cohort from September 2013 to March 2015 was the prospective cohort study, “Korea INfectious Diseases Study Group/Staphylococcus aureus Bacteremia 2013 (KIND-SAB 2013) cohort” with project name, “Establishment of Network for Clinical Research of Staphylococcus aureus Infection”. The KIND-SAB 2013 cohort was supported by Grant No. HI10C2020 from the National Strategic Coordinating Center for Clinical Research, which is run by the Ministry of Health and Welfare, Government of Korea. We have registered the protocol of the last KIND-SAB 2013 cohort study (KCT0001070) and the present comparative study (KCT0001088) with the Clinical Research Information Service of the Republic of Korea (![]() ) in cooperation with the WHO International Clinical Trials Registry Platform.
) in cooperation with the WHO International Clinical Trials Registry Platform.
Disclosure Statement
No competing financial interests exist.