
Abstract
We sought to detect and determine the genetic diversity of carbapenemase-producing Enterobacteriaceae (CPE) isolated from clinical specimens in Amman, Jordan. From five hospitals, a total of 2,759 isolates had antimicrobial susceptibilities determined via Vitek II, of which 28 (1%) were carbapenem resistant. Species identifications were determined via matrix-assisted laser desorption ionization time-of-flight mass spectrometry and carbapenemase gene detection via real-time PCR indicated that 23 (82.1%) isolates were Klebsiella pneumoniae (OXA-48-like, n = 7; NDM, n = 14; OXA-48-like and NDM, n = 2), four (14.2%) were Enterobacter cloacae complex (NDM, n = 3 and VIM, n = 1), and one (3.5%) was Escherichia coli (NDM). Sequencing of carbapenemase gene amplicons from a subset of isolates identified blaNDM-1, blaOXA-48, and blaVIM-4 alleles. Strain typing detected seven different K. pneumoniae variable number tandem repeat types, consistent with mostly sporadic occurrences along with limited clonal spread. E. cloacae complex isolates were diverse by pulsed-field gel electrophoresis, with a maximum relatedness of 70%. Plasmid restriction fragment length polymorphism (pRFLP) revealed four distinct profiles associated with NDM-encoding plasmids that were positive for replicons of the FII(K)/FIB or FIB incompatibility (Inc) groups via PCR-based replicon typing. OXA-48-encoding IncL/M plasmids differed by two pRFLP bands. The results show diverse CPE produce OXA-48 and NDM-1 enzymes in Jordan and that the carbapenemase genes are distributed on diverse plasmids in Jordanian hospitals, with some limited evidence for related clusters occurring, emphasizing the need for strict infection control measures.
Background
I
Materials and Methods
Bacterial isolates and identification
From May 2013 to April 2014, 2,759 nonduplicate Enterobacteriaceae were isolated from clinical specimens (blood culture, urine, fluid, wound, and sputum) from patients in five of the royal medical services hospitals in Amman, Jordan, ranging in size from 200 to 600 beds. Isolates were referred to the central hospital for antimicrobial susceptibility determinations using Vitek II (bioMérieux, Marcy l'Etoile, France). Susceptibilities were interpreted according to the recommendations of the Clinical and Laboratory Standards Institute (CLSI) guidelines, 2014. 14 Additional susceptibilities for tigecycline and colistin were determined at Public Health England using agar dilution methodology and interpreted according to European Committee on Antimicrobial Susceptibility Testing (EUCAST) v4 breakpoints (www.eucast.org/ast_of_bacteria/previous_versions_of_documents date last accessed: September 20, 2017). Species identification was determined using matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-ToF MS, Bruker Microflex LT; Bruker Daltonik GmbH, Bremen, Germany).
Screening for carbapenemase-producing isolates
Isolates that showed decreased susceptibility to one of the carbapenems (imipenem MIC ≥2 μg/ml, meropenem MIC ≥2 μg/ml, or ertapenem MIC ≥1 μg/ml) were considered as possible carbapenemase producers according to the CLSI guidelines (2014), and selected for further analysis.
Real-time PCR for carbapenemase genes (blaNDM, blaVIM, blaKPC, and blaOXA-48-like)
Carbapenemase genes were detected via real-time PCR 15 using lysates of freshly cultured bacteria. Assays were done using a Rotor-Gene Q instrument (QIAGEN, Crawley, UK) as described previously. 15
Variable number tandem repeat and pulsed-field gel electrophoresis typing
Variable number tandem repeat (VNTR) and pulsed-field gel electrophoresis (PFGE) typing methods were performed to determine the clonal relationships of the isolates. VNTR analysis of nine loci (A, E, H, J, K, D, N1, N2, and N4) was performed for K. pneumoniae isolates as described previously.16,17 PFGE of XbaI-digested genomic DNA was performed as described previously 17 for Enterobacter spp.. VNTR profiles and PFGE gel images were analyzed and compared using BioNumerics (Applied Maths, Sint-Martens-Latem, Belgium) software, version 6.1. PFGE banding patterns were interpreted using a similarity cutoff of ≤86% to identify nonrelated isolates.
Plasmid transfers
Plasmids encoding carbapenemase enzymes were electroporated into Escherichia coli Alpha-Select recipients (Bioline, London, UK). Colonies selected on Luria-Bertani (LB) agar containing 100 mg/L ampicillin were screened for the presence of carbapenemase genes by RT-PCR. 15 Conjugation experiments were attempted from LB broth cultures at 37°C with a donor to recipient (E. coli J-53, azide resistant) ratio of 1:4, incubated on LB agar, followed by selection on agar containing azide and ampicillin (100 mg/L).
Plasmid DNA purification and plasmid restriction fragment length polymorphism
Plasmid DNA was purified from transformants using a phenol/chloroform extraction. 18 Plasmid DNA was digested with restriction enzyme PstI overnight and subjected to electrophoresis on a 0.85% agarose gel.
PCR-based replicon typing
PCR-based replicon typing (PBRT) was performed as previously described19–21 on transformant DNA lysates (above). For PBRT-negative samples, an additional test for the FIB(pQIL) replicon (GenBank Accession No. GU595196) used FIB(pQIL)_F 5′- TCAGAAAAGGATCGGAATGG-3′ and FIB(pQIL)_R 5′- GCTCAGGAAGGCTCTCAATG-3′ (J. Findlay, unpublished).
Allele sequencing
Complete carbapenemase genes from representatives with each combination of carbapenemase gene family type, plasmid replicon, and plasmid restriction fragment length polymorphism (pRFLP) type were PCR amplified and sequenced. Alleles were identified via BLAST against the National Center for Biotechnology Information nucleotide database.
Results
Bacterial isolates, susceptibility testing, and carbapenemase identification
From 2,759 isolates we identified 28 CPE (1%), comprising 23 (82.1%) K. pneumoniae, four (14.2%) Enterobacter cloacae complex, and one E. coli isolate. All were resistant to imipenem, meropenem, ertapenem, fosfomycin, ampicillin, amoxicillin/clavulanic acid, ticarcillin, piperacillin/tazobactam, cephalothin (≥16 mg/L), cefoxitin, cefotaxime, and ceftazidime. Most (60%) were resistant to ciprofloxacin, ofloxacin, nitrofurantoin, and trimethoprim/sulfamethoxazole. At the time of testing (2015), additional antimicrobial susceptibilities to tigecycline and colistin were observed in 94% of the isolates. The 23 K. pneumoniae isolates harbored genes encoding OXA-48-like (n = 7), NDM-1 (n = 14), and both OXA-48 and NDM-1 (n = 2) genes. The four E. cloacae complex isolates encoded either NDM-1 (n = 3) or VIM-4 (n = 1) genes, and the E. coli isolate encoded an NDM-1 gene (Table 1).
A, adult; B, child; F, female; ICU, intensive care unit; Int med, internal medicine department; M, male; MALDI, matrix-assisted laser desorption ionization.
Molecular epidemiology of bacterial isolates
Of 23 K. pneumoniae isolated, 17 were available for further characterization, and of these 14 encoded NDM alone, two encoded OXA-48 alone, and one isolate encoded both NDM-1 and OXA-48. VNTR typing for the 17 K. pneumoniae isolates indicated seven different VNTR profiles as follows: 5,3,5,14,14,2,4,2,1 (corresponding to sequence type (ST) 147) (n = 7 isolates; hospital 1), 5,4,1,1,-,2,4,4,1 (corresponding to ST101) (n = 3; hospital 4), 3,5,2,13,2,1,3,4,1 (corresponding to ST11) (n = 2; hospitals 2 and 5), 2,4,2,8,0,2,2,3,1 (corresponding to ST48) (n = 2; hospitals 1 and 3), 3,2,4,9,2,2,2,4,1 (corresponding to ST327) (n = 1; hospital 1), 6,3,4,0,1,1,4,1,1 (corresponding to ST14) (n = 1; hospital 1), and 3,3,3,0,1,1,4,1,1 (corresponding to ST15) (n = 1; hospital 1). Of the NDM-positive K. pneumoniae isolates, seven were obtained from a single hospital and had VNTR profiles that corresponded to ST147; two isolates with VNTR profiles corresponding to ST11 were identified from separate hospitals. Single isolates of types corresponding to STs 14, 15, and 327 were all obtained from hospital 1, while an isolate with a type corresponding to ST48 was obtained from hospitals 1 and 3 (Table 2). Three K. pneumoniae with OXA-48 were obtained from a single hospital (hospital 4) and had a VNTR type that corresponded to ST101, one of the isolates encoded both OXA-48 and NDM-1. Each of the four E. cloacae complex isolates (Supplementary Fig. S1; Supplementary Data available online at www.libertpub.com/mdr) was distinct by PFGE. Three E. cloacae encoded NDM-1 (from hospitals 3 and 4) and one encoded VIM-4 (from hospital 4) (Table 2). A single isolate of E. coli, which encoded NDM, was obtained from hospital 1 (Table 2).
MLST, multilocus sequence types; ND, not determined; NT, nontypable; PBRT, PCR-based replicon typing; pRFLP, plasmid restriction fragment length polymorphism; VNTR, variable number tandem repeat.
Molecular epidemiology of carbapenemase-encoding plasmids
From our previous work, 9 NDM plasmids were detected in patients of three different nationalities, hospitalized in a single hospital. Conjugation assays did not identify a self-transferable carbapenemase-encoding plasmid, but transformation did reveal NDM was encoded on IncFIB(pQIL) or IncFII(K)/FIB(pQIL) plasmid replicons in 13 K. pneumoniae and within each replicon type there was a high degree of pRFLP relatedness. For example, seven ST147 isolates (from a single hospital) encoded NDM on IncFIB(pQIL) plasmids that were mostly indistinguishable as pRFLP type B (Fig. 1). Six K. pneumoniae isolates encoded NDM on IncFII(K)/FIB(pQIL) plasmids that were indistinguishable as pRFLP type C. The corresponding isolates were diverse by MLST, representing at least four STs. The pRFLP type C profile (Table 2) from the IncFII(K)/FIB(pQIL) NDM replicon found in the E. coli (isolate no. 1, Fig. 1) was indistinguishable from other pRFLP type C plasmids. One NDM plasmid with a novel pRFLP profile and an unknown replicon type occurred in an ST11 isolate (isolate no. 14, Fig. 1). OXA-48 was encoded on IncL/M plasmids that differed by two pRFLP bands in two isolates from the same hospital, which included an ST101 isolate. Another ST101 isolate from the same hospital encoded OXA-48 and NDM-1, of which NDM was shown to be encoded on an IncFII(K)/FIB(pQIL) replicon. OXA-48 was not encoded on the incFII(K)/FIB(pQIL) replicon and no transformant with OXA-48 was isolated from this sample.
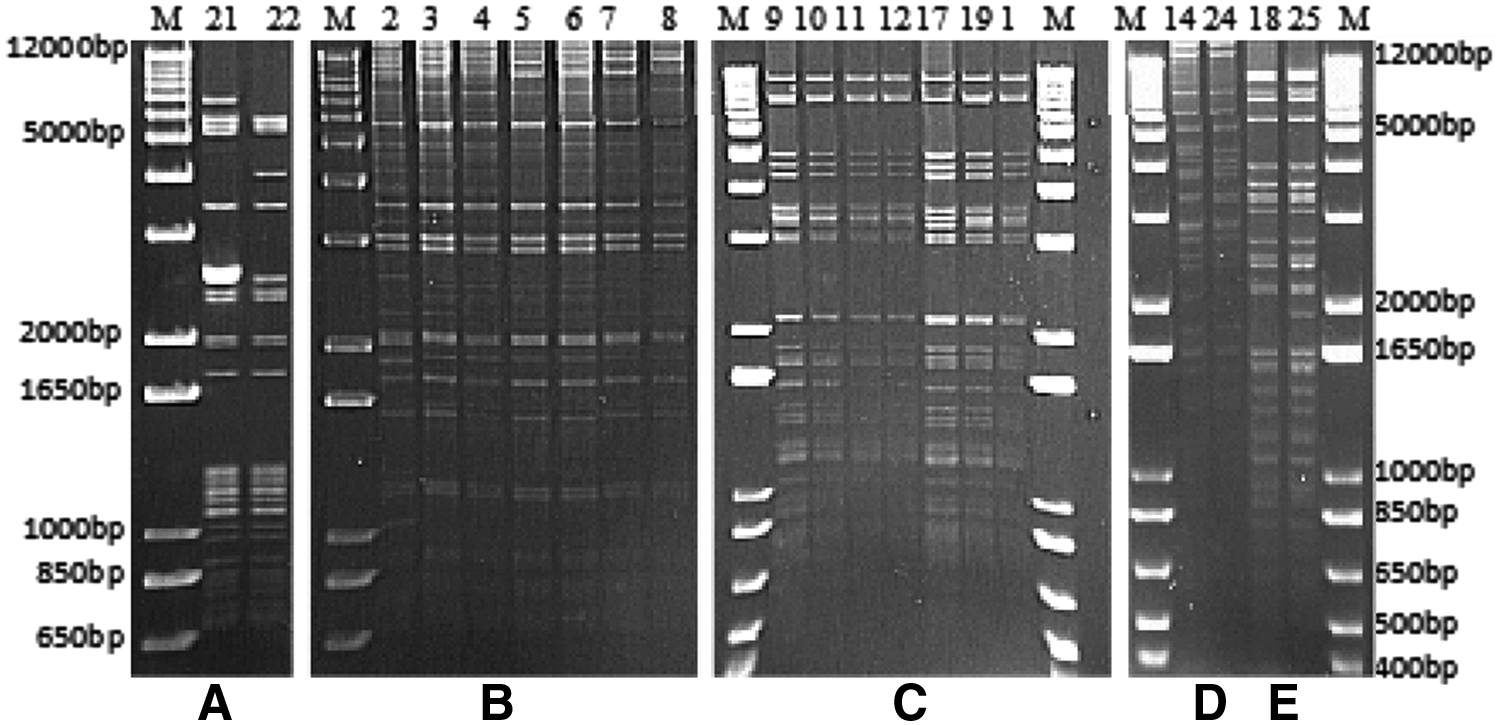
pRFLP of the 20 NDM and OXA-48-like carrying CPE isolates. pRFLP type
The carbapenemase-encoding plasmids from three NDM-1- and one VIM-4-positive E. cloacae complex isolates were nontypable via PBRT. The NDM-encoding plasmids from three isolates were typable by pRFLP as either type D or E. The two isolates with pRFLP type E patterns occurred in different hospitals (Fig. 1, Table 2).
Discussion
Enterobacterial infections are the most frequent nosocomial infections in Jordan.1,11 A recent study by Aqel et al. 9 detected carbapenem resistance in 2.4% of K. pneumoniae in Jordan, while in this study we found CPE to account for 1.0% of Enterobacteriaceae, most often as K. pneumoniae. The breakpoints used in this study were higher than the screening concentrations now recommended by EUCAST for CPE screening, making it possible that some CPE were missed by our initial phenotypic screening. However, the criteria we used were consistent with the CLSI breakpoints used previously by ourselves 9 and others in surrounding countries,22–24 despite these consistencies the rate we observed was lower than from previous reports for carbapenemase-producing K. pneumoniae in Jordan and lower than the 2–20% range observed elsewhere in our region.22–24 Compared with our previous work, this could be explained by the larger sample size of this study. 25 Indeed, the detection of NDM-1 and OXA-48 as the most frequent carbapenemases is in agreement with other studies from the Middle East.12,13,25 Unlike other studies, we did not detect any KPC or IMP producers13,25–27 and the observed dominance of NDM-1followed by OXA-48 enzymes differed from our previous findings as well as the regional epidemiology.9,10 K. pneumoniae encoding both NDM-1 and OXA-48 in the same isolate have been detected recently in neighboring countries such as Turkey; they also appear to be readily spread and are associated with a high fatality rate. 28 The lack of relatedness between the carbapenemase-producing E. cloacae complex isolates, as well as the diversity observed among the carbapenemase-producing K. pneumoniae, indicates that while clonal spread within the hospitals we studied may occur in some instances, the largest part of the CPE burden in Amman, Jordan, is due to diverse bacterial types and may represent plasmid spread. While the international spread of NDM-1 has been confirmed in countries such as Morocco, France, and the United States,12,29 the underexplored extent of plasmid spread raises the possibility of undetected national- and even international-level transmission events introducing and disseminating carbapenem resistance into Jordanian hospitals. 1 The dissemination of NDM-1 across five Jordanian hospitals included in this work indicates the endemicity of NDM-1 and/or possible horizontal transmission between diverse bacterial types. The two pRFLP profiles observed from the PBRT nontypable NDM-encoding plasmids in E. cloacae complex isolates and the four pRFLP profiles from common NDM-associated PBRT types in K. pneumoniae 19 clearly indicate the multiple origins of the plasmids disseminated in such CPE isolates. In contrast, the observation of an NDM-encoding plasmid of the same PBRT and highly related pRFLP type (type C) in E. coli and multiple types of K. pneumoniae suggests a highly mobile plasmid, but the limited discriminatory power of pRFLP prevents firm conclusions about direct transmission events without further detailed investigation. Nevertheless, the observed similarities highlighting the risk of horizontal dissemination of resistance through different species via, for example, plasmids pose a large medical risk in the country and will severely limit treatment choices. Carbapenem resistance among Enterobacteriaceae is a serious clinical problem detected in Jordanian hospitals. Despite the diversity of the isolates and their origins across different clinical departments and specimen types, our results indicated mostly the same resistance profiles to diverse drugs in all three CPE species (K. pneumoniae, E. cloacae complex, and E. coli). However, around 94% of the isolates remained susceptible to tigecycline and colistin indicating that these agents were viable therapeutic options. In summary, the prevalence of CPE found in this study is considered low when compared to that of the region or worldwide. However, the results of the current study represent an early alarm that mandates extra vigilance and more immediate efforts to improve the ability of laboratories to detect, identify, and characterize CPE. It also highlights the necessity for effective infection control measures, active surveillance, and up-to-date management plans to limit the spread of CPE within healthcare settings and also reduce the mortality and morbidity they cause.
Footnotes
Acknowledgments
We thank the AMRHAI staff for their assistance with this project. Amin Aqel's visit to Public Health England, London, was funded by the Daniel Turnberg UK/Middle East Travel Fellowship Scheme, 2015.
Disclosure Statement
J.F., M.J.E., K.L.H., J.T., and N.W. are part of PHE's AMRHAI Reference Unit, which has received financial support for conference attendance, lectures, research projects, or contracted evaluations from numerous sources, including Accelerate Diagnostics, Achaogen, Inc., Allecra Therapeutics, Amplex, AstraZeneca UK Ltd, Basilea Pharmaceutica, Becton Dickinson Diagnostics, BioMérieux, Bio-Rad Laboratories, The BSAC, Cepheid, Check-Points B.V., Cubist Pharmaceuticals, Department of Health, Enigma Diagnostics, Food Standards Agency, GlaxoSmithKline Services Ltd, Henry Stewart Talks, IHMA Ltd, Kalidex Pharmaceuticals, Melinta Therapeutics, Merck Sharpe & Dohme Corp, Meiji Seika Pharma Co, Mobidiag, Momentum Biosciences Ltd, Nordic Pharma Ltd, Norgine Pharmaceuticals, Rempex Pharmaceuticals Ltd, Roche, Rokitan Ltd, Smith & Nephew UK Ltd, Trius Therapeutics, VenatoRx Pharmaceuticals, and Wockhardt. All other authors declare no competing interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.