
Abstract
Aims:
Amoxicillin-clavulanate is extensively used in European hospitals. Whether the hospital use of amoxicillin-clavulanate is associated with nonsusceptibility to third-generation cephalosporins (3GC) in Klebsiella pneumoniae is unknown. Our aim was to assess the relationship between the hospital use of amoxicillin-clavulanate and 3GC nonsusceptibility in K. pneumoniae and Escherichia coli.
Methods:
Yearly data of antibiotic use and 3GC nonsusceptibility in K. pneumoniae and E. coli were obtained from 33 French hospitals between 2011 and 2016. Decreased susceptibility to 3GC and Extended-Spectrum Beta-Lactamase (ESBL) production were modelled from antibiotic use with linear mixed models on years 2011 to 2015, and validated on year 2016.
Results:
Nonsusceptibility to 3GC increased in K. pneumoniae and E. coli. In a multivariable model that included year and use of 3GC and fluoroquinolones as explanatory variables, amoxicillin-clavulanate use was protective against 3GC nonsusceptibility in K. pneumoniae (incidence rate ratio [IRR], 0.992 [0.988–0.997]), and with ESBL production in K. pneumoniae (IRR, 0.989 [0.985–0.992]). The correlation coefficient between observed and predicted numbers of 3GC-nonsusceptible K. pneumoniae in 2016 was 0.95 (95% confidence interval, 0.89–0.98). There was no significant association between amoxicillin-clavulanate use and 3GC nonsusceptibility in E. coli.
Conclusion:
Amoxicillin-clavulanate hospital use was protective against nonsusceptibility to 3GC in K. pneumoniae. Conversely, it was not associated with susceptibility to 3GC in E. coli. To decrease the hospital use of 3GC and fluoroquinolones, and 3GC nonsusceptibility in K. pneumoniae, it may be acceptable to increase the hospital use of amoxicillin-clavulanate. Interventional studies are necessary to confirm this hypothesis.
Introduction
A
While amoxicillin-clavulanate is used extensively in European hospitals, no ecological study has focused on the association between hospital use of amoxicillin-clavulanate and decreased susceptibility to 3GC in Klebsiella pneumoniae. Furthermore, it remains unknown whether replacing 3GC with amoxicillin-clavulanate would decrease 3GC resistance at the hospital level. Our objective was to assess the relationship between the hospital use of amoxicillin-clavulanate and decreased susceptibility to 3GC in K. pneumoniae and E. coli.
Methods
The study was conducted in 33 private and public hospitals of Pays de la Loire, a 32,000 km2 and 3.7 million inhabitant French region. Seven, 14, and 12 were <100-, 100–300-, and >300-bed hospitals, respectively. Each year between 2011 and 2016, resistance and antibiotic use data were transmitted to the OMEDIT Pays de la Loire regional surveillance system of antibiotic use and bacterial resistance using preformatted spreadsheets. These spreadsheets were configured to transform raw antibiotic use into DDD per 1,000 patient-days for each hospital, as recommended by the World Health Organization Collaborating Centre for Drugs Statistics (www.whocc.no). From 2012, the web-based system CONSORES (www.consores.net) was used in place of preformatted spreadsheets for antibiotic use surveillance. Each participating hospital provided the number of nonduplicate E. coli and K. pneumoniae isolates grown from samples for diagnostic purpose from all hospital units (except Emergency Departments and ambulatory care units), and the number of pathogens with decreased susceptibility to 3GC. Isolates were deduplicated according to the guidelines of the Observatoire National de l'Epidémiologie de la Résistance Bactérienne aux Antibiotiques. 19 Bacterial identification and antibiotic susceptibility tests were performed in each hospital using routine methods, including BioMerieux Vitek 2 and matrix-assisted laser desorption ionization time-of-flight mass spectroscopy for identification, and BioMerieux Vitek 2 and BD Phoenix for susceptibility tests. Susceptibility tests were performed and interpreted as recommended by the current French Society for Microbiology guidelines. Isolates were classified as susceptible when minimum inhibitory concentration of ceftriaxone or cefotaxime was 1 mg/L or lower.
Statistical analysis
Descriptive statistics were expressed as median (25th–75th percentiles) and range. Analysis of variance (ANOVA) was used to compare antibiotic use according to bed number classes. The temporal trend of antibiotic use expressed as DDD/1,000 hospital days was assessed using a linear mixed model to allow individual intercept and trend for each hospital. The temporal trend was compared to zero using a Student test. We also modeled the evolution of the yearly use of amoxicillin-clavulanate use by a linear mixed model with a fixed effect for 3GC and fluoroquinolone use, and a random effect for hospital to allow individual intercept for each hospital.
The temporal trend of the number of nonsusceptible strains was assessed using a negative binomial linear mixed model, which included a fixed effect for year and a random effect for hospital and year within hospital, and the number of tested isolates as offset. The association of antibiotic use and resistance was modeled with a negative binomial linear mixed model, which included a fixed effect for year and antibiotic use, and a random effect for hospital and year within hospital. Incidence rate ratios (IRRs) were computed as the exponentiated estimates of negative binomial models.
Models were derived from data of years 2011–2015 and were then validated on data of year 2016 by comparing observed and predicted values. To test our main objective, we used models that included amoxicillin-clavulanate, 3GC, and fluoroquinolones. We also had an unsupervised strategy, with univariate analysis of the association between resistance and use of 12 antibacterial classes (amoxicillin, amoxicillin-clavulanate, piperacillin-tazobactam, 3GC, carbapenems, fluoroquinolones, lincosamides, macrolides-lincosamides-streptogramins, aminoglycosides, imidazole derivatives, tetracyclines, and glycopeptides), followed by a multivariate analysis that included antibiotics associated with resistance in univariate analysis at a p-value <0.20, with a backward selection to minimize the Akaike Information Criteria (AIC). Statistical significance was fixed at a p-value ≤0.05. Statistical analyses were performed using R software version 3.2.3 (December 10, 2015) with the lme4 package (http://CRAN.R-project.org).
Ethical issues
According to the French law, this study was not submitted to an ethics committee, as we collected no patient individual data.
Results
Antibiotic use
Between 2011 and 2016, there was a significant increase in use of piperacillin-tazobactam and 3GC, and a significant decrease of fluoroquinolones (Table 1). Similar trends were observed when antibiotic use was expressed as a percentage of total antibiotic use (Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/mdr). In 2015, amoxicillin-clavulanate, 3GC, and fluoroquinolones accounted for 30.7%, 9.4%, and 9.1% of total antibiotic use, respectively (total antibiotic use, 371.4 DDD/1,000 hospital days). There was a high variability between hospitals in antibiotic use, as shown by the interquartile range and the range of antibiotic use (Supplementary Table S2). We pooled antibiotic use among <100-, 100–300-, and >300-bed hospitals (Supplementary Table S3). ANOVA showed no statistical difference between these three classes, except for tetracyclines (p = 0.02). Furthermore, we found that amoxicillin-clavulanate use was highly associated with fluoroquinolone use (estimate [standard deviation, SD], 0.8 (0.1); p-value <0.0001), but not with 3GC use (estimate [SD], −0.1 [0.5]; p = 0.90). This model should be interpreted as follows, when comparing two hospitals with identical 3GC use on the same year: if their fluoroquinolone use differed by 1 DDD/1,000 hospital days, their amoxicillin-clavulanate would differ by 0.8 DDD/1,000 hospital days.
Yearly antibiotic use was computed as the sum of antibiotic use in each hospital divided by the sum of hospital days of each hospital. Trend estimates are reported with their SD, and were compared with zero using a Student test.
SD, standard deviation.
Resistance to 3GC
The median (first and third quartile) [range] numbers of isolates of K. pneumoniae and E. coli included per hospital andper year were 28 (15–57) [10–538] and 271 (152–601) [12–4,696], respectively. The proportion of 3GC-nonsusceptible K. pneumoniae in the whole cohort increased from 8.3% (6.9–9.8%; number of tested isolates, 1,450) in 2011 to 16.2% (14.4–18.2%; number of tested isolates, 1,494) in 2016 (Fig. 1). This increase was highly significant as shown by the multilevel modeling (IRR of the fixed effect for year, 1.19 [1.12–1.26]). In other words, according to this model, the proportion of 3GC-nonsusceptible K. pneumoniae increased 1.19-fold each year. This increase was confirmed when the analysis was restricted to the hospitals (n = 14) that had susceptibility data of K. pneumoniae for the 6 years of the study period, the proportion of 3GC-nonsusceptible K. pneumoniae increasing from 8.9% (95% confidence interval [CI], 7.4–10.6%; number of tested isolates, 1,240) in 2011 to 16.4% (95% CI, 14.5–18.6%; number of tested isolates, 1,277) in 2016. The proportion of 3GC-nonsusceptible K. pneumoniae of each hospital was computed for the whole study period and showed high variability among hospitals, as median (first and third quartile) was 7.2% (3.9–10.4%), the range being 0.0–28.8%.
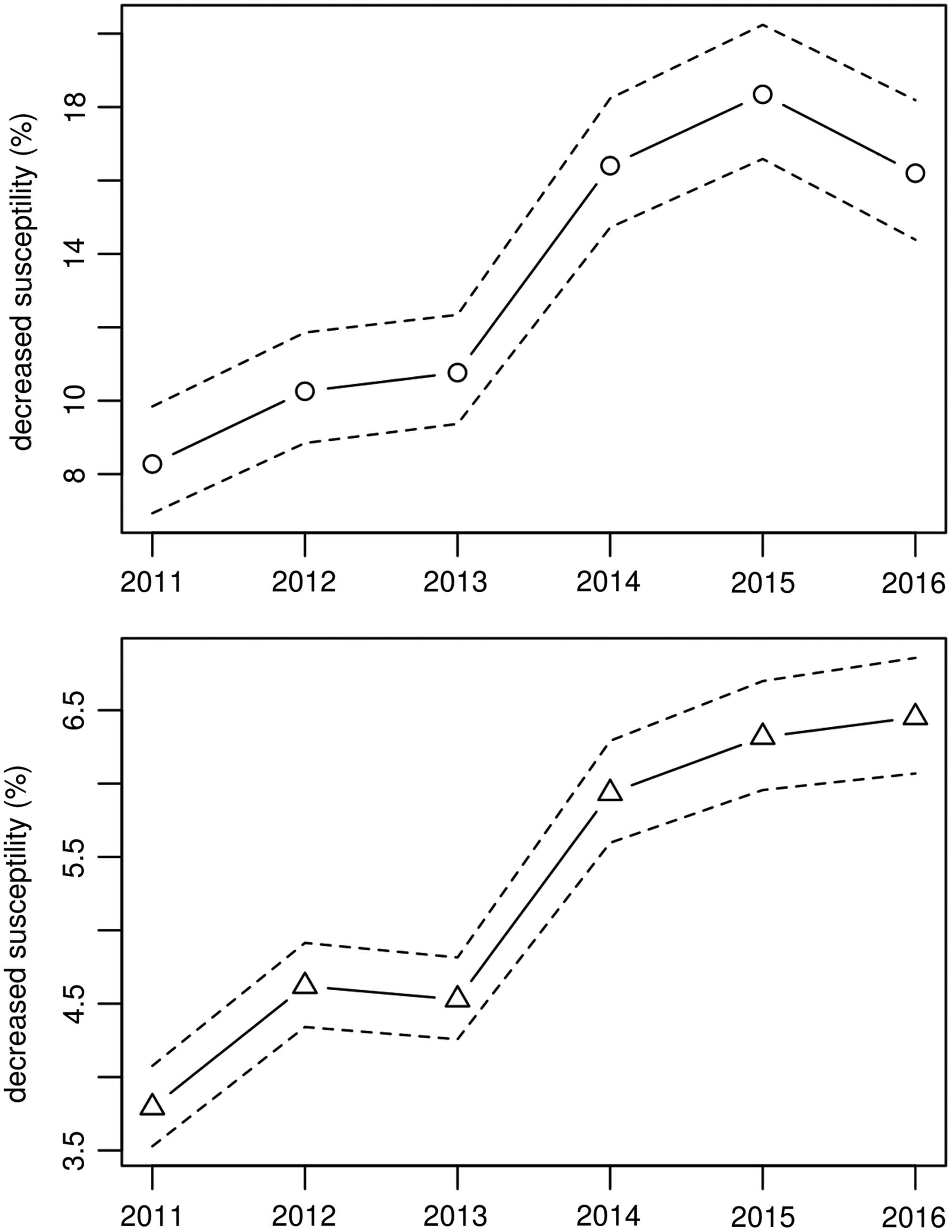
Yearly proportion of third-generation cephalosporin-nonsusceptible Klebsiella pneumoniae and Escherichia coli in 33 hospitals, 2011–2016, Pays de la Loire, France. Full line, proportion. Dashed lines, 95% confidence interval. Circle, K. pneumoniae; triangle, E. coli. Yearly proportions of nonsusceptible isolates were computed as the sum of nonsusceptible isolates in all hospitals divided by the sum of tested isolates.
The proportion of 3GC-nonsusceptible E. coli increased between 2011 and 2016, from 3.8% (3.5–4.1%; number of tested isolates, 19,061) to 6.4% (6.1–6.9%; number of tested isolates, 15,190) in the whole cohort (Fig. 1). This increase was highly significant as shown by the multilevel modeling (IRR of the fixed effect for year, 1.11 [1.07–1.15]), meaning that the proportion of 3GC-nonsusceptible E. coli increased 1.11-fold each year. The increasing proportion of resistant bacteria was confirmed when the analysis was restricted to hospitals (n = 24) that had susceptibility data of E. coli for the 6 years of the study period, from 3.7% (95% CI, 3.5– 4.1%; number of tested isolates, 16,189) in 2011 to 6.4% (95% CI, 6.0–6.8%; number of tested isolates, 14,137) in 2016. The proportion of 3GC-nonsusceptible E. coli was computed for the whole study period and showed some variability among hospitals, as median (first and third quartile) was 4.9% (3.8–5.6%), the range being 2.5–13.1%.
Between 2011 and 2016, the proportion of extended-spectrum beta-lactamase (ESBL)-producing isolates increased from 6.8% (95% CI, 5.4–8.5%; number of tested isolates, 1,079) to 12.9% (95% CI, 11.0–15.1%; number of tested isolates, 1,068) for K. pneumoniae, and from 2.9% (95% CI, 2.6–3.2%; number of tested isolates, 14,466) to 4.4% (95% CI, 4.0–4.8%; number of tested isolates, 11,073) for E. coli (Supplementary Fig. S1).
Relationship between antibiotic use and 3GC nonsusceptibility
After adjusting on year, amoxicillin-clavulanate use tended to be associated with susceptibility to 3GC in K. pneumoniae (Table 2, p = 0.15). This association was highly significant (IRR [95% CI], 0.992 (0.988–0.997), p-value <0.001) when the use of 3GC and fluoroquinolones was added to the model (Table 2). This IRR should be interpreted as follows, when comparing two hospitals with identical 3GC and fluoroquinolone use on the same year: if amoxicillin-clavulanate use in hospital A exceeded by 1 DDD/1,000 hospital days the amoxicillin-clavulanate use in hospital B, the proportion of 3GC-nonsusceptible K. pneumoniae in hospital A would be 0.992-fold the proportion in hospital B. Similar results were observed when modeling ESBL-mediated resistance in K. pneumoniae (Supplementary Table S4). Models including antibiotic use of the preceding and current years had higher AICs than models that only included the current year's antibiotic use, and showed similar results for the association between amoxicillin-clavulanate use and decreased susceptibility to 3GC or ESBL production in K. pneumoniae.
IRRs (95% CI) of fixed effects of each antibacterial class. All models included the year among explanatory variables. IRR should be interpreted as follows when comparing two hospitals with identical 3GC and fluoroquinolone use in the same year: if amoxicillin-clavulanate use in hospital A exceeded by 1 DDD/1,000 hospital days the amoxicillin-clavulanate use in hospital B, the proportion of 3GC-nonsusceptible K. pneumoniae in hospital A would be 0.992-fold the proportion in hospital B.
3GC, third-generation cephalosporins; CI, confidence interval; DDD, defined daily doses; IRR, incidence rate ratio.
Furthermore, we tested the association between other antibacterial classes and decreased susceptibility to 3GC in K. pneumoniae. In univariate analysis, in addition to amoxicillin-clavulanate, fluoroquinolones, and 3GC, amoxicillin, piperacillin-tazobactam, carbapenems, and glycopeptides were associated with nonsusceptible K. pneumoniae with a p-value <0.20. After backward selection, the multivariate model retained only three antibacterial classes, namely amoxicillin-clavulanate, fluoroquinolones, and 3GC. Similarly, seven antibacterial classes (amoxicillin, 3GC, carbapenems, macrolides-lincosamides-streptogramins, aminoglycosides, fluoroquinolones, and glycopeptides) were associated with ESBL-producing K. pneumoniae at p-value <0.20 in univariate analysis. Only 3GC (IRR [95% CI], 1.052 [1.030–1.074], p-value <0.0001) and fluoroquinolones (IRR [95% CI], 1.015 [0.998–1.031], p = 0.08) were retained in the final multivariate model.
After adjusting on year and use of 3GC and fluoroquinolones, amoxicillin-clavulanate use tended to be associated with susceptibility to 3GC in E. coli (Table 3). Similar results were observed when modeling ESBL-mediated resistance in E. coli (Supplementary Table S5). As observed for K. pneumoniae, models including antibiotic use of the preceding and current years had higher AICs than models that only took account of current year's antibiotic use, and showed similar results for the association between amoxicillin-clavulanate use and decreased susceptibility to 3GC or ESBL production in E. coli. We also tested the association between other antibacterial classes and decreased susceptibility to 3GC in E. coli. In univariate analysis, piperacillin-tazobactam, 3GC, carbapenems, macrolides-lincosamides-streptogramins, aminoglycosides, and fluoroquinolones were associated with 3GC-nonsusceptible E. coli at p-value <0.20. After backward selection, the multivariate model with the lowest AIC had only three antibacterial classes, namely carbapenems (IRR [95% CI], 1.028 [1.001–1.051], p = 0.02), macrolides-lincosamides-streptogramins (IRR [95% CI], 0.980 [0.967–0.993], p-value <0.01), and 3GC (IRR [95% CI], 1.006 [1.000–1.013], p = 0.055). Similarly, six antibacterial classes (3GC, carbapenems, lincosamides, aminoglycosides, fluoroquinolones, and glycopeptides) were associated with ESBL-producing E. coli at p-value <0.20 in univariate analysis. Only 3GC (IRR [95% CI], 1.011 [1.004–1.018], p-value <0.01) and fluoroquinolones (IRR [95% CI], 1.006 [0.999–1.013], p = 0.12) were retained in the final multivariate model.
IRRs (95% CI) of fixed effects of each antibacterial class. All models included the year among explanatory variables. IRR should be interpreted as follows when comparing two hospitals with identical amoxicillin-clavulanate and fluoroquinolone use in the same year: if 3GC use in hospital A exceeded by 1 DDD/1,000 hospital days the 3GC use in hospital B, the proportion of 3GC-nonsusceptible E. coli in hospital A would be 1.008-fold the proportion in hospital B.
Subgroup analyses
Similarly, we found that the use of amoxicillin-clavulanate was protective against nonsusceptibility to 3GC in K. pneumoniae when the analysis was restricted to (1) hospital years with at least 50 tested isolates, (2) hospitals with available data for each year between 2011 and 2015, (3) hospitals with 100–300 beds, (4) hospitals with at least 300 beds, and (5) hospitals that had a proportion of nonsusceptible K. pneumoniae in the third quartile of the cohort (Supplementary Fig. S2).
Predicted resistance in 2016
Models including amoxicillin-clavulanate, 3GC, and fluoroquinolones as explanatory variables were used to predict the number of nonsusceptible isolates in 2016 (Fig. 2). The models showed a very good predictive value, as Pearson correlation coefficients (95% CI) between observed and predicted numbers of 3GC-nonsusceptible isolates for K. pneumoniae and E. coli in 2016 were 0.95 (0.89–0.98) and 0.93 (0.86–0.97), respectively.
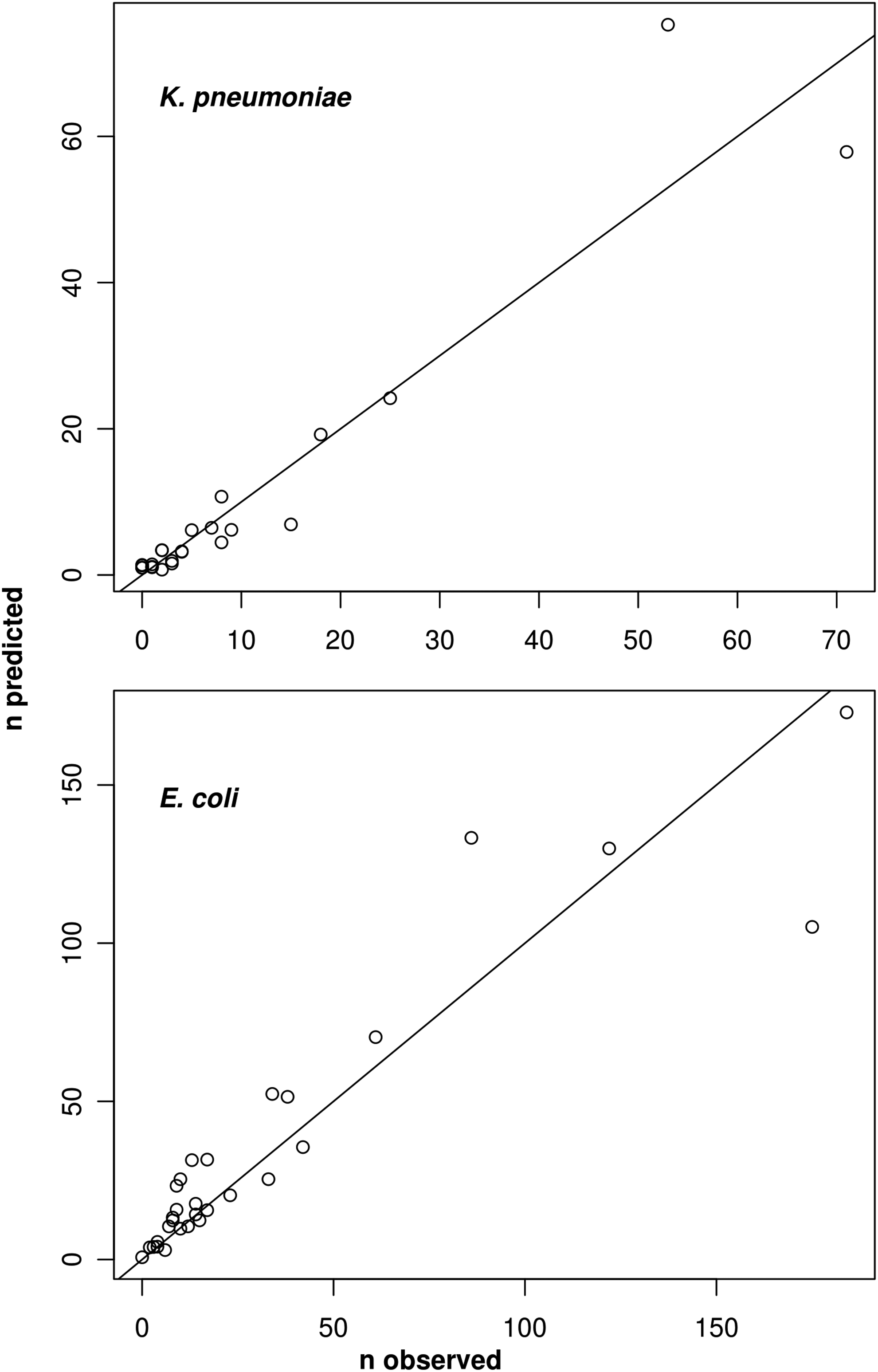
Predicted numbers of third-generation cephalosporin decreased susceptibility for 2016. Note: Each point represents a hospital in 2016. The line represents n observed = n predicted.
Discussion
No study had previously assessed the relationship between the hospital use of amoxicillin-clavulanate and 3GC nonsusceptibility in K. pneumoniae at the hospital level. In this multicentric study involving 33 hospitals, a higher amoxicillin-clavulanate use hospital-wide was associated with a lower proportion of 3GC nonsusceptibility in K. pneumoniae. Conversely, we found no significant association between amoxicillin-clavulanate hospital use and decreased susceptibility to 3GC in E. coli, as previously reported.13,20 These results corroborate the hypothesis that the declining cephalosporin nonsusceptibility among Enterobacteriaceae, especially frank for Klebsiella spp., was linked with replacement of cephalosporins and quinolones by penicillin/β-lactamase inhibitor combinations in UK hospitals. 21
Few studies have assessed the relationship between exposure to amoxicillin-clavulanate and decreased susceptibility to 3GC in Enterobacteriaceae at the individual level, and they had conflicting results.5,9,22,23 Only one study reported separate results for Klebsiella spp. and found no association between exposure to amoxicillin-clavulanate and ESBL-mediated resistance. 5 Another study found that exposure to beta-lactamase inhibitor (mainly amoxicillin-clavulanate) was a protective factor against ESBL-producing K. pneumoniae. 24
The use of piperacillin-tazobactam was not associated with decreased susceptibility to 3GC or ESBL production in our study, as previously reported in a multicentric ecological study. 13 Of note, two ecological studies—both monocentric and conducted in university hospitals—found either a positive association between piperacillin-tazobactam use and cefepime resistance in E. coli or a negative association between use of ticarcillin or piperacillin with or without enzyme inhibitor (in fact, mainly piperacillin-tazobactam) and ESBL-producing Enterobacteriaceae.2,25 The infrequent use of piperacillin-tazobactam in this cohort's hospitals (<2% of total antibiotic use) may make our study insufficiently powered to detect a relationship between piperacillin-tazobactam use and bacterial resistance.
Our results need to be confirmed by other observational studies and experimental and mechanistic investigations. Among the reasons why use of amoxicillin-clavulanate would not increase or even decrease nonsusceptibility to 3GC in K. pneumoniae at the hospital level is the persisting activity of penicillin/β-lactamase inhibitor combinations against ESBL-producing Enterobacteriaceae. Thus, in an experimental model of fecal carriage of a piperacillin-tazobactam-susceptible K. pneumoniae strain, piperacillin-tazobactam promoted carriage if mice were inoculated before or after antibacterial treatment, but inhibited carriage if mice were inoculated during treatment.26,27 Hence, amoxicillin-clavulanate may favor more weakly than 3GC the growth of enteric 3GC-resistant isolates. Furthermore, hypothetical differences between amoxicillin-clavulanate and 3GC in disruption of the intestinal microbiota may explain differences in intensity, duration, and transmissibility of fecal carriage of 3GC-nonsusceptible organisms.
Our study had four main limitations. First, the observational design only demonstrates association and not causal relationship between antibiotic use and bacterial resistance. A causal relationship between amoxicillin-clavulanate use and 3GC resistance should be tested at the hospital level through experimental studies aiming to increase the hospital use of amoxicillin-clavulanate, and decrease those of 3GC and fluoroquinolones. In our observational study, amoxicillin-clavulanate might be less used because of highly prevalent 3GC-nonsusceptible Enterobacteriaceae. However, this interpretation is questionable in this study's hospitals, where amoxicillin-clavulanate is mainly used for community-acquired infections (e.g., community-acquired lower respiratory tract infections where 3GC-nonsusceptible Enterobacteriaceae are exceptionally isolated), while 3GC-nonsusceptible Enterobacteriaceae are mainly associated with heathcare-associated infections. Moreover, we found no significantly decreased use of amoxicillin-clavulanate during the study period, whereas the proportion of 3GC-nonsusceptible K. pneumoniae almost doubled. Finally, by including the hospital as a random effect, we allowed the model to take account of various hospital characteristics, including prescription habits, antibiotic resistance prevalence, proportion of hospital-acquired isolates, and outbreaks of 3GC-nonsusceptible K. pneumoniae. Cross-sectional studies provide the opportunity to easily assess the relationship between antibiotic use and resistance, in various settings and periods that may differ in antibiotic use and level of bacterial resistance. In opposition with monocentric studies based on time-series analyses, which are usually conducted in tertiary referral hospitals, our study was conducted in a cohort including <100-, 100–300-, and >300-bed hospitals, thus being representative of French hospitals.
Second, resistance data encompassed all isolates, including those cultured in the beginning of the hospital stay, associated with community-acquired infections, among which susceptibility should not be influenced by the hospital antibiotic use. Restricting the analysis to bacteria isolated from the 3rd hospital day would address this limitation. 25 However, this design requires patient individual data that were not collected by our multicentric surveillance system.
Third, some DDD fixed by the WHO collaborative center may not represent usual dosing in French hospitals. In particular, the WHO collaborative center-defined DDD of amoxicillin and oral amoxicillin-clavulanate is 1 g, whereas usual daily doses in French hospitals are 3 g. Furthermore, the WHO DDD of ceftriaxone is 2 g, whereas the usual daily dose is 1 g in French hospitals. These differences may lead to underestimate the association of 3GC nonsusceptibility with 3GC use and overestimate its relationship with amoxicillin-clavulanate use. We chose not to modify the DDD, to allow for comparison with hospital networks in other countries.
Fourth, this study was only conducted at the institution level, and we collected no data to describe patients who were hospitalized during the study period. This study should be complemented with adequately powered patient-level studies. Ecological group-level and patient-level studies provide different results on the association between a given antibacterial class and a given bacterial resistance, as ecological studies also take account for interhuman transmissibility of resistant bacteria. 28
The WHO has classified aminopenicillins, including amoxicillin-clavulanate, as high priority critically important antimicrobials, and 3GC and fluoroquinolones as highest priority critically important antimicrobials. 29 In this study, we found that amoxicillin-clavulanate hospital use was protective against nonsusceptibility to 3GC in K. pneumoniae. Conversely, it was not associated with susceptibility to 3GC in E. coli. These results suggest that for combating decreased susceptibility to 3GC in K. pneumoniae at the hospital level, the hospital use of 3GC and fluoroquinolones should be decreased, and to this end, it may be acceptable (or even useful) to increase the hospital use of amoxicillin-clavulanate. In particular, amoxicillin-clavulanate may be promoted instead of 3GC in community-acquired lower respiratory tract infections.30–34 Ecological, hospital-level interventional studies are necessary to confirm this hypothesis.
Footnotes
Acknowledgments
The authors warmly thank pharmacists and microbiologists of the OMEDIT network for providing antibiotic use and bacterial resistance data. M.-A.V. thanks the DefiMaths Program and Fédération de Recherche Mathématiques des Pays de Loire for financial support.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.