
Abstract
This study was conducted to investigate the phenotypic and genotypic characteristics of vancomycin–resistant Enterococcus faecalis and Enterococcus faecium. Antibiotic resistance and virulence genes in the aforementioned resistant isolates were studied using the epsilometer (E)-test and polymerase chain reaction (PCR). These isolates were subjected to typing by pulsed-field gel electrophoresis (PFGE). Thirty vancomycin-resistant enterococci (VRE; 18.75%) were isolated from a total of 160 various clinical specimens cultured for any bacterial growth. Of these, 11 (36.7%) isolates were identified as E. faecalis and 19 (63.3%) as E. faecium. Minimum inhibitory concentrations (MICs) of vancomycin, teicoplanin, and three alternative therapeutic options (linezolid, daptomycin, and quinupristin/dalfopristin) were determined using the E-test. Multiplex PCR was done for confirming species, identification of the resistant genotypes, and the detection of the virulence genes. Finally, the clonal relationship of all VRE strains was studied by PFGE. All VRE strains showed vancomycin MIC ≥256 μg/mL, and 27 (90%) isolates carried the vanA gene, whereas none of the isolates carried vanB. The most common resistance antibiotic pattern observed was toward rifampicin (n = 30 [100%]). Among all virulence genes studied, gelE (n = 28 [93.33%]) was found as the most prevalent virulent gene. VRE isolates exhibited 90%, 46.67%, 100%, and 66.67% resistance to teicoplanin, linezolid, quinupristin/dalfopristin, and daptomycin, respectively. Molecular typing demonstrated 16 PFGE types of VRE isolates (A–P). Although vanA was carried by most of the isolates, PFGE displayed small clonal dissemination among VR E. faecium and VR E. faecalis species.
Introduction
E
Among vancomycin (VAN)-resistance phenotypes in enterococci, VanA and VanB have the highest clinical importance.
6
vanA and vanB genes encode for ligase, involved in the synthesis of low-affinity precursors, in which the C-terminal
Since the presence of VRE imposes many problems for healthcare systems such as an increase of the length of stay and financial burden, therefore, it is vital to monitor the prevalence, investigate the involved resistance mechanisms, and search any surrogate therapeutic agent. This study aimed to: (1) investigate the phenotypic and genotypic characteristics of VRE isolates, (2) determine the minimum inhibitory concentrations (MICs) of vancomycin, teicoplanin (TEC), linezolid, daptomycin, and quinupristin/dalfopristin (Q/D), (3) investigate the resistance genotypes [vanA, vanB, and aac(6′)Ie-aph(2″)Ia], along with the detection of seven virulence genes (gelE, esp, ace, asa1, cpd, hyl, and cylA) in VRE isolates, and (4) analyze the clonal relationship among VRE strains by pulsed-field gel electrophoresis (PFGE).
Materials and Methods
Identification of the isolates
The work was performed in 4 University Teaching Hospitals of Urmia and Tabriz, northwest of Iran, from September 2014 to July 2015, and 30 VRE isolates were obtained from culture of various clinical specimens. The sources of these isolates were as follows: urine n = 25 (83.33%), blood n = 2 (6.67%), body fluids n = 2 (6.67%), and wound n = 1 (3.33%). The isolates were identified at the species level by conventional methods using Facklam et al.'s recommendations 10 and then subjected to confirmation by PCR as previously described. 11
Susceptibility testing procedures
Antimicrobial susceptibility to ampicillin (AMP, 10 μg), ciprofloxacin (CIP, 5 μg), doxycycline (DXT, 30 μg), erythromycin (ERY, 15 μg), gentamicin (GM, 120 μg), penicillin G (PG, 10 units), rifampicin (RP, 5 μg), streptomycin (S, 300 μg), teicoplanin (30 μg), and vancomycin (30 μg; Mast Group Ltd., Merseyside, UK) was assessed by the Kirby-Bauer disk diffusion method using Mueller-Hinton agar (Merck, Co.). Accordingly, results were analyzed based on the Clinical Laboratory Standards Institute (CLSI) criteria. 12 Susceptibility testing for urine isolates included nitrofurantoin (NI, 300 μg) too.
The presence of VRE was screened by the use of 6 μg/mL vancomycin added to the Brain Heart Infusion (BHI) agar. MICs of vancomycin, teicoplanin, linezolid, daptomycin, and quinupristin/dalfopristin were determined by epsilometer (E)-test (Liofilchem). Results of MICs were analyzed according to CLSI guidelines. 12 Enterococcus faecalis ATCC 29212 was used as quality control vancomycin susceptible strain.
Detection of vancomycin, gentamicin resistance, and virulence genes by PCR
Two vancomycin resistance-associated genes, vanA and vanB, gentamicin resistance-associated gene, aac(6′)Ie-aph(2″)Ia, and seven virulence-associated genes, gelE, esp, ace, asa1, cpd, hyl, and cylA, were detected by the multiplex PCR, using specific primers and PCR conditions as described earlier.11,13,14 The primer sequences and the expected sizes of amplicons are presented in Table 1.
PFGE typing
PFGE was performed according to Murray et al. 15 with some modifications. Briefly, VRE isolates were grown overnight in a BHI broth. Bacterial cells embedded in 2% low–melting point agarose (Sigma) plugs were lysed with lysozyme and proteinase K. Then, chromosomal DNA was digested with SmaI restriction enzyme (Fermentas). Fragmented DNA samples were electrophoresed in 1% pulsed-field certified agarose (Bio-Rad) using a CHEF Mapper system (Bio-Rad) at 14°C for 23 hours, with a pulse time of 5–35 seconds at 6 V/cm2 in the 0.5× Tris-borate-EDTA (TBE) buffer. Gels were stained with 1 μg/mL ethidium bromide and photographed under ultraviolet illumination. Salmonella choleraesuis serotype Braenderup H9812 was used as the molecular size standard. The banding patterns were interpreted by Dice analysis and clustered by the unweighted pair group method with arithmetic averages, using GelCompar II version 4.0 (Applied Maths, Sint-Matenslatem, Belgium). The isolates were categorized into the same PFGE pulsotype group based on over 90% similarity criterion.
Statistical analyses
The values are presented as percentages. Pearson's chi-square test was used to draw the comparison of the frequencies. All statistical analyses were conducted using SPSS v22 software. p-Value of <0.05 was assumed as statistically significant.
Results
A total of 30 (18.75%) VRE isolates were obtained from a total of 160 clinical specimens cultured for the presence of any routine bacteria. Most of them were isolated from intensive care units (ICUs), Nephrology (each n = 8; 26.67%), while four specimens were taken from outpatients (n = 4; 13.33%) who provided nearly the same history of previous hospitalization. By conventional biochemical tests and PCR, 11 (36.7%) isolates were identified as E. faecalis, and 19 (63.3%) isolates were identified as E. faecium.
Antibiotic susceptibility pattern of VRE isolates is presented in Table 2. Irrespective of the species, VRE isolates exhibited resistance toward rifampicin (n = 30; 100%), teicoplanin (n = 27; 90%), streptomycin (n = 20; 66.67%), and a high level gentamicin resistance (HLGR; n = 19; 63.33%).
Code: I, intermediate; R, resistant; S, susceptible; T, Tabriz; U, Urmia.
AMP, ampicillin; CIP, ciprofloxacin; DXT, doxycycline; ERY, erythromycin; GM, gentamicin; MIC, minimum inhibitory concentration; NI, nitrofurantoin; PG, penicillin G; Qui/Dal, quinupristin/dalfopristin; RP, rifampicin; S, streptomycin; TEC, teicoplanin; VAN, vancomycin.
All VRE isolates showed vancomycin MIC ≥256 μg/mL. Twenty-seven isolates (90%) carried the vanA gene, while vanB gene was not detected in any of them. The highest prevalence of vanA gene was observed in E. faecium isolated from Tabriz with a frequency of 44.44% (n = 12; p < 0.01). All HLGR isolates were positive for aac(6′)Ie-aph(2″)Ia gene.
According to the MIC result by E-test, the rate of resistance among VRE isolates to teicoplanin, linezolid, quinupristin/dalfopristin, and daptomycin was 90%, 46.67%, 100%, and 66.67%, respectively.
Molecular detection of virulence genes revealed that gelE (93.3%; Pv = 1), asa1 (76.7%; Pv = 0.031), and cpd (56.7%; Pv = 0.016) were the most frequently detected virulence traits, irrespective of the species. The esp and hyl virulence genes were detected only in VR E. faecium (47.4% and 89.5%, respectively), while the cylA gene was detected only in VR E. faecalis species (27.3%; Pv = 0.001) (Table 3).
VR, vancomycin resistant.
The analysis of molecular typing demonstrated 20 PFGE patterns among the 29 VRE isolates (1 isolate being lost during transport before typing), as shown in Fig. 1. According to a similarity coefficient higher than 90%, VRE isolates were distributed into 16 groups (A–P), and isolates belonging to the same group were considered as closely related (Table 4). Eleven VR E. faecalis and 18 VR E. faecium were distributed into 5 (L–P) and 11 groups (A–K), respectively. PFGE patterns demonstrated five common types, including 14 isolates with 90% of similarity. The remaining 15 isolates (51.7%) were highly diverse, belonging to 15 single types (Fig. 1).
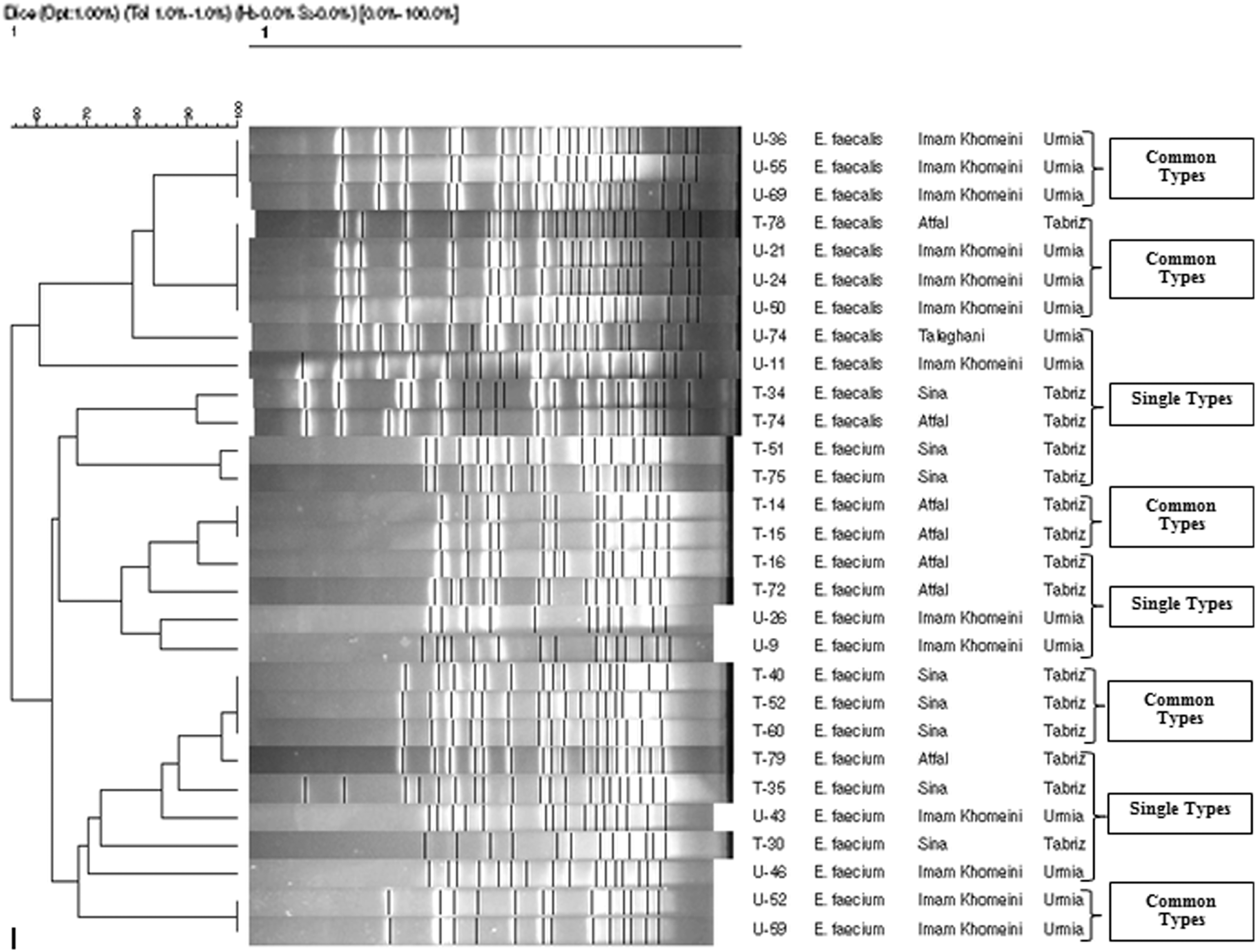
The PFGE analysis of all VRE isolates with their relevant types. PFGE, pulsed-field gel electrophoresis; VRE, vancomycin-resistant enterococci.
ICU, intensive care unit; PFGE, pulsed-field gel electrophoresis.
Discussion
VRE have been increasingly reported worldwide since their first description in 1987. In addition, the epidemiology of these microorganisms varies widely between different geographical areas. 16 Although there are scientific reports regarding the frequency of VRE from different areas of Iran,9,11 to the best of our knowledge, no study has yet been carried out on the molecular typing of VRE in the northwest of Iran.
In the present investigation, majority of VRE were E. faecium (63.3%), and the remaining were E. faecalis (36.7%). In several studies from different countries a similar enhancement in the prevalence of VRE, especially E. faecium, has been noticed earlier.17,18
ICUs have been known to be the reason for the spread of multidrug-resistant bacteria among the hospitalized patients, medical personnel, and within hospital wards. In accordance with Talebi et al. study, 19 our study observed that VRE was isolated more commonly from ICUs (26.7%), compared to other wards in the hospital.
Urinary tract was found to be the most important source of VRE (83.33%), which is consistent with another study specifying it as the major disseminating source of VRE and other organisms. 19
The commonest phenotype seen among VRE strains is VanA, in which a high level inducible resistance to both vancomycin and teicoplanin is observable (MICs ≥64 μg/mL). 6 Among the 30 VRE isolates characterized in this study, 27 (90%) carried the vanA gene, as reported by another study carried out in Tehran, Iran. 18 With regard to the strains without vanA gene, the diversity of plasmids, different types of transposons, and the genetic diversity in Tn1546 through point mutations in orf1, vanS, vanA, vanX, and vanY have been reported among VRE. 20 This could account for the inability to detect the mentioned gene.
The progressive increase in VRE prevalence in Iran is a serious concern, and vancomycin may not serve as the drug of choice for the treatment of multidrug–resistant Gram positive cocci infections in the near future.
In this study, resistance to vancomycin was accompanied by resistance to high level gentamicin (63.33%), ampicillin (66.67%), and ciprofloxacin (86.67%). This finding is in accordance with some other studies.19,21 The detection of high level resistance to gentamicin is the cause of concern, as this organism could limit the combination therapy (a cell wall—active antibiotic like ampicillin or vancomycin plus an aminoglycoside such as streptomycin or gentamicin), which could be essential for severe infections like endocarditis.
Linezolid, quinupristin/dalfopristin, and daptomycin have been proposed as the surrogate drugs for treating vancomycin-resistant bacteria and have been evaluated even for the treatment of serious infections with VRE.22–24
Linezolid was the first oxazolidinone available for clinical use in 2000. It is active against both E. faecium and E. faecalis. 7 However, in the current study, 14 (46.67%) isolates were found resistant to this agent. Outbreaks due to linezolid-resistant enterococci, notwithstanding how rare, have been reported by Ntokou et al. 22
Daptomycin has previously been shown to be successful in treating methicillin–resistant Staphylococcus aureus associated meningitis and other serious VRE infections. 23 However, in the present investigation 20 (66.67%) isolates were found resistant to daptomycin. Quinupristin/Dalfopristin has bactericidal activity against various Gram-positive bacteria, while bacteriostatic against VR E. faecium. It also lacks activity against E. faecalis due to efflux pumps. 24 All VRE isolates (100%) in our study were found to be resistant to quinupristin/dalfopristin.
The results of the current study are consistent with other findings whereby the resistance to linezolid, daptomycin, and quinupristin–dalfopristin has been previously indicated in VRE isolates.25–27
The presence of virulence factors associated with enterococci enhances their pathogenicity. 28 Indeed virulence in this genus has been typically considered a multifactorial process with the involvement of several genes and their products. 29
The aggregation substance encoded by asa1 gene–mediated binding to the host epithelium appeared to mediate bacterial aggregation during conjugation, facilitating plasmid exchange. 30 In this study, 9 (81.8%) out of 11 VR E. faecalis harbored asa1 gene, and all (100%) of them were isolated from urine specimens. These results indicate a significant association between the presence of asa1 and the occurrence of urinary tract infection (UTI) (p < 0.05) by VR E. faecalis. Although the source of most of asa1+ VR E. faecium (n = 11; 78.6%) was also urine, the association was not significant (p > 0.05). Waar et al. reported the high prevalence of asa1 in E. faecalis isolates from liver transplant and septicemic patients and supposed association of asa1 with such infections. 31
Another study on enterococci isolated from food and clinical specimens showed that the asa1 gene was always associated with the presence of pheromone determinants (cpd, cob, ccf, and cad), and the specified gene was present only in E. faecalis. 32 Similarly, the current study found cpd gene in all VR E. faecalis isolates and of them 72.7% were also asa1 positive (p < 0.001). Meanwhile, we could find cpd in 6 (31.6%) VR E. faecium isolates, which is consistent with another study which described the presence of sex pheromone determinant in E. faecium isolates. 11
Gelatinase is a zinc metalloprotease encoded by gelE, with hydrolytic capacity. 33 This study detected gelE gene in all (100%) VR E. faecalis and 89.5% of VR E. faecium. Similarly, Sabia et al. reported the existence of gelE gene in 70% and 71.4% of VR E. faecalis and VR E. faecium strains, respectively. 34 In fact, among virulence genes investigated, the concomitant occurrence of gelE and cpd in VR E. faecalis isolates was found to be significant (p < 0.001).
Adhesion of collagen (Ace) is encoded by ace gene. It is a cell surface protein present in E. faecalis that binds collagen (types I and IV) and laminin and belongs to the microbial surface components recognizing adhesive matrix molecules (MSCRAMM) family. Studies have demonstrated that Ace protein may contribute to the pathogenesis of enterococci in endocarditis. 35 The present study revealed the presence of ace gene in 63.6% of VR E. faecalis and in 15.8% of VR E. faecium, in accordance with another study from Iran where the incidence of the ace gene was identified in clinical VRE isolates. 11 All ace positive isolates were obtained from urine (UTI), while isolates from other sources were negative for this gene. Lebreton et al. suggested that Ace protein could be a valuable drug target against human UTI. 35
The extracellular surface protein (Esp), encoded by the esp gene, is a cell wall associated protein, which serves as an adhesion for the pathogen to colonize host tissue and persists in urinary tract infections. 36 However, in the present study, the esp gene was detected in 9 (47.4%) of VR E. faecium isolates; it was not found in VR E. faecalis isolates. These findings are consistent with other studies,11,13 identifying the high prevalence of the esp gene among VR E. faecium. Moreover, earlier, Chuang-Smith et al. had speculated that Esp could mediate the interaction with primary surfaces and participate in the biofilm formation. 37
cylA did not appear to be a characteristic gene since it was not detected in any of the clinical E. faecium isolates in our study. This assumption has also been supported by the results obtained from other studies.11,13,38
Similar to esp gene, the hyl gene was also detected only in VR E. faecium isolates (89.5%) in the present investigation. Variations in the prevalence of hyl have been documented in VR E. faecium. A study was done in Mexico, and half (50%) of their isolates carried hyl 39 while a higher prevalence rate has been reported (71%) from the United Kingdom. 13 Such a difference could be attributed to the region and population variations. The esp and hyl genes were significantly more common among ampicillin–resistant VR E. faecium isolates than ampicillin-susceptible isolates, which is consistent with the findings of Vael et al. study. 40 Notably, we found that 8 of 17 (47.1%) hyl-positive VR E. faecium strains were also esp positive, suggesting that hyl and esp could function together to enhance the virulence of VR E. faecium. Similar finding has been reported earlier by Yang et al., 38 who described the combined presence of hyl and esp in 94.7% of their strains.
PFGE typing is a cost-effective method providing information about the relatedness of bacterial isolates, extensively used for the surveillance of hospital associated infections. 41
In the current study, PFGE results indicated small clonal dissemination of VR E. faecium and VR E. faecalis species in different wards of the same hospital and even in different hospitals and the two cities (Table 4). The results of the current study are consistent with those of an earlier study, which indicated the clonal dissemination of VRE isolates at different occasions. 2 Furthermore, other studies have also documented the clonal dissemination of VR E. faecium 42 and E. faecalis. 43 The absence of an ongoing alert system for patients infected or colonized with VRE upon hospital readmission in our country might have contributed to this dissemination. Overall, the data obtained from this analysis suggest that there was no genetically important relationship between the two enterococcus species.
To conclude, our findings highlight the incremental emergence of VRE in our clinical setting. In addition, most of these VRE strains frequently carried antimicrobial resistance and virulence genes. The commonest phenotype of glycopeptide resistance distinguished in our study was the VanA phenotype. Data from molecular typing suggest that there was no genetic relationship between strains isolated from two different hospitals in the northwest of Iran. These results highlight the relevance of VRE monitoring constantly in these and other hospitals to detect future possible changes in the prevalence and genotypes of this important multidrug-resistant pathogen, which holds special significance in human health.
Footnotes
Acknowledgments
This article is a report of a database from the PhD thesis of A.J. registered in Tabriz University of Medical Sciences. This work was supported fully by Infectious and Tropical Diseases Research Centre (Grant No. 93.5-7.17), Tabriz University of Medical Sciences (Tabriz, Iran).
Disclosure Statement
No competing financial interests exist.