
Abstract
This study investigated the prevalence and antibiotic resistance of Ureaplasma spp. and Mycoplasma hominis isolated from asymptomatic individuals in Korea. Endocervical swabs from women and urine from men, from a total of 5,781 asymptomatic individuals, were analyzed using a Mycoplasma IST2 Kit. Of the 4,825 specimens tested from females, 486 (10.1%) were positive culture. In these positive specimens, 437 (9.1%) were positive only for Ureaplasma spp., 17 (0.4%) were positive only for M. hominis, and 32 (0.7%) were positive for both Ureaplasma spp. and M. hominis. In males, of the 956 tested specimens, only 4 (0.42%) were positive for Ureaplasma spp. and no M. hominis colonization was identified. In antimicrobial susceptibility tests, more than 93.2% of both M. hominis and Ureaplasma spp. was susceptible to tetracycline, doxycycline, josamycin, and pristinamycin. However, M. hominis isolates were found to be highly resistant to erythromycin, azithromycin, and clarithromycin (82.4%, 70.6%, and 76.5%, respectively). Ofloxacin and ciprofloxacin, which have recently exhibited increasing resistance rates, showed rates of 17.7% and 35.3%, respectively, in M. hominis, and 50.6% and 27.4%, respectively, in Ureaplasma spp. In conclusion, accurate antimicrobial susceptibility tests of the genital mycoplasmas should be conducted for each case to select the appropriate antibiotics. Fluoroquinolone-based drugs should be avoided in the initial treatment of urogenital mycoplasmas because of the increasing rate of resistance to quinolones, although the susceptibility to tetracycline remains high in Korea.
Introduction
M
Because of the lack of a cell wall, mycoplasmas are not affected by many common antibiotics that target cell wall synthesis such as beta-lactam antibiotics (penicillin and cephalosporins). 1 Mycoplasmas are susceptible to agents that interfere with protein synthesis, such as tetracycline, macrolides, aminoglycosides, and chloramphenicol, and to the fluoroquinolones that act by inhibiting topoisomerases.9–11 Mycoplasma infections are usually treated with tetracycline, except in pregnant women, neonates, and children, in whom erythromycin is recommended.12,13
In recent years, due to the overuse of antibiotics and the tetM gene, the incidence of tetracycline resistance in mycoplasma infections has been increasing.14–16 tetM is a ribosomal protection protein that is involved in tetracycline resistance. 17 Therefore, clindamycin, fluoroquinolones, or other macrolides are usually used to treat infections that do not respond to tetracycline or erythromycin. 12 However, resistance to these drugs has also been reported, 18 and mycoplasmas can develop resistance to antibiotics to which they are usually considered to be susceptible. 10 The extent of resistance varies geographically and depends on the use of different antibiotics and the history of previous antimicrobial exposure of different populations. 19
Therefore, it is important to identify the local antibiotic susceptibility of mycoplasmas to provide guidance for the rational use of antibiotics in the clinic and determine the most appropriate agents for empirical therapy. The aim of this study was to investigate the prevalence and antibiotic resistance of Ureaplasma spp. and M. hominis isolated from asymptomatic individuals in Korea.
Materials and Methods
Clinical specimens
Endocervical swabs from women and urine from men were obtained from individuals for urogenital mycoplasma analysis. A total of 5,781 individuals (4,825 females and 956 males) were analyzed from January 2011 to December 2015. All the individuals were outpatients attending St. Vincent's Hospital in Korea for healthcare screening. They did not have any symptoms of genital tract infections (urethral or vaginal discharge, dysuria, urethral irritation, itching, genital lesions, and abdominal pain). Approximately 500 μL of urine or 100 μL of endocervical and vaginal swab specimens was collected by physicians or well-trained nurses. The collected samples were immediately refrigerated, and all the tests were performed within 24 hours of collection. This study was approved by the Institutional Review Board of the Catholic University of Korea (VC16RISI0029).
Urogenital mycoplasma culture and antibiotic susceptibility testing
A Mycoplasma IST2 kit (bioMerieux, Marcy-l'Etoile, France) was used for the detection, enumeration, identification, and antibiotic susceptibility testing of Ureaplasma spp. and M. hominis. Clinical specimens were inoculated in liquid transport medium R1 that contains selective agents to inhibit the growth of contaminating flora present in the sample. The samples in the R1 transport medium were centrifuged for 10 seconds and used to rehydrate the lyophilized selective growth medium R2. This medium was then dispensed into 22 test wells of 55 μL each, and two drops of mineral oil were overlaid on each compartment to prevent desiccation. The strips were incubated at 37°C for 48 hours and observed for color changes. Positive results were a change in color of the culture medium from yellow to red as a result of alkalization and an estimate of the density of each organism ≥104 colony-forming unit.
There were two concentration assay wells for each of nine antibiotics (doxycycline, josamycin, ofloxacin, erythromycin, tetracycline, ciprofloxacin, azithromycin, clarithromycin, and pristinamycin). The development or absence of red color of the strip provided an index of the resistance or susceptibility to each antimicrobial agent. No discoloration to red in either of the wells implied the sensitivity of the Mycoplasma, whereas discoloration to red in both wells signified resistance. Mycoplasma was considered moderately susceptible to the antibiotic tested if the low-concentration assay wells turned red. 20 The breakpoints (mg/L) were as follows: doxycycline S ≤4, R ≥8; josamycin S ≤2 R ≥8; ofloxacin S ≤1, R ≥4; erythromycin S ≤1, R ≥4; tetracycline S ≤4, R ≥8; ciprofloxacin S ≤1, R ≥2; azithromycin S ≤0.12, R ≥4; clarithromycin S ≤1, R ≥4; and pristinamycin R ≥2.
Results
Prevalence of urogenital mycoplasma of the urogenital tract
The positive rates of urogenital mycoplasma in male and female individuals are shown in Table 1. In females, of the 4,825 tested specimens, 486 (10.07%) were positive for urogenital mycoplasma. In these positive specimens, 437 (9.06%) were positive only for Ureaplasma spp., 17 (0.35%) were positive only for M. hominis, and 32 (0.66%) were positive for both Ureaplasma spp. and M. hominis. In males, of the 956 tested specimens, only 4 (0.42%) were positive for Ureaplasma spp. and no M. hominis colonization was identified. By stratified age groups, the highest positive rates of urogenital mycoplasmas in females were detected in the 30–40 years age group (M. hominis: 41.2%, Ureaplasma spp.: 32.3%, and both Ureaplasma spp. and M. hominis: 12.5%), and lower levels were found in women older than 50 years (Table 2; Fig. 1).
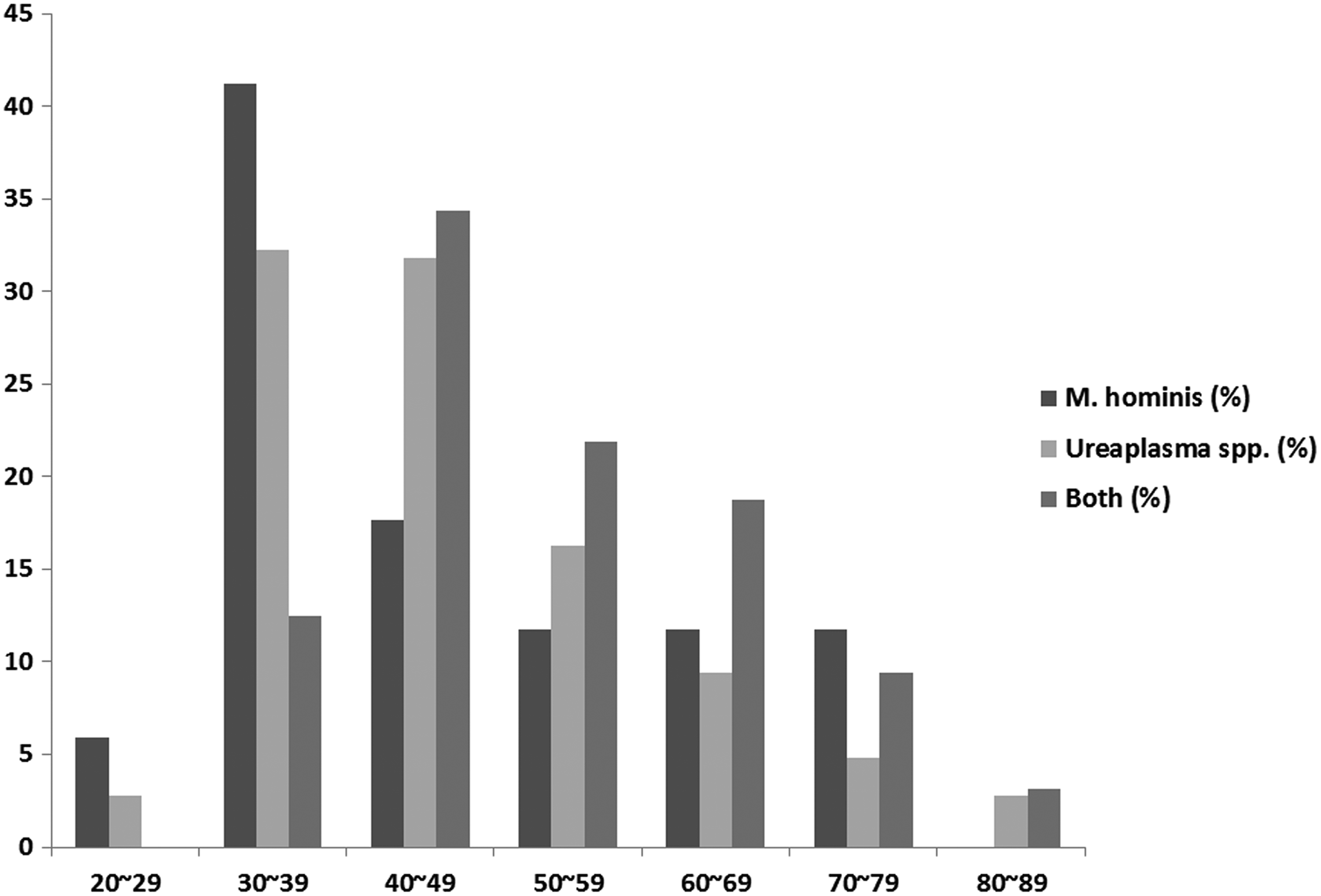
Distribution of Mycoplasma hominis and Ureaplasma spp. in different age groups of women. Both—both Ureaplasma spp. and M. hominis.
Both—both Ureaplasma spp. and M. hominis.
Antibiotic susceptibility of urogenital mycoplasmas in vitro
The antimicrobial susceptibilities of M. hominis and Ureaplasma spp. are shown in Table 3 and Fig. 2. Most of the Ureaplasma spp. isolates were susceptible to tetracycline, doxycycline, pristinamycin, and josamycin (93.2%, 95.46%, 97.28%, and 95.24%, respectively). Most of the Ureaplasma spp. isolates were susceptible to clarithromycin, azithromycin, and erythromycin (82.31%, 87.3%, and 82.77%, respectively). Ofloxacin proved to be inactive in approximately half of the isolates (50.57%), and ciprofloxacin was almost ineffective in Ureaplasma spp. isolates (27.44%). Similarly, M. hominis isolates were susceptible to josamycin, pristinamycin, doxycycline, and tetracycline (100%, 100%, 100%, and 94.12%, respectively). However, M. hominis isolates exhibited high resistance to erythromycin, azithromycin, and clarithromycin (82.35%, 70.59%, and 76.47%, respectively). Ofloxacin and ciprofloxacin, which have recently shown increasing resistance rates, showed rates of 17.65% and 35.29%, respectively.
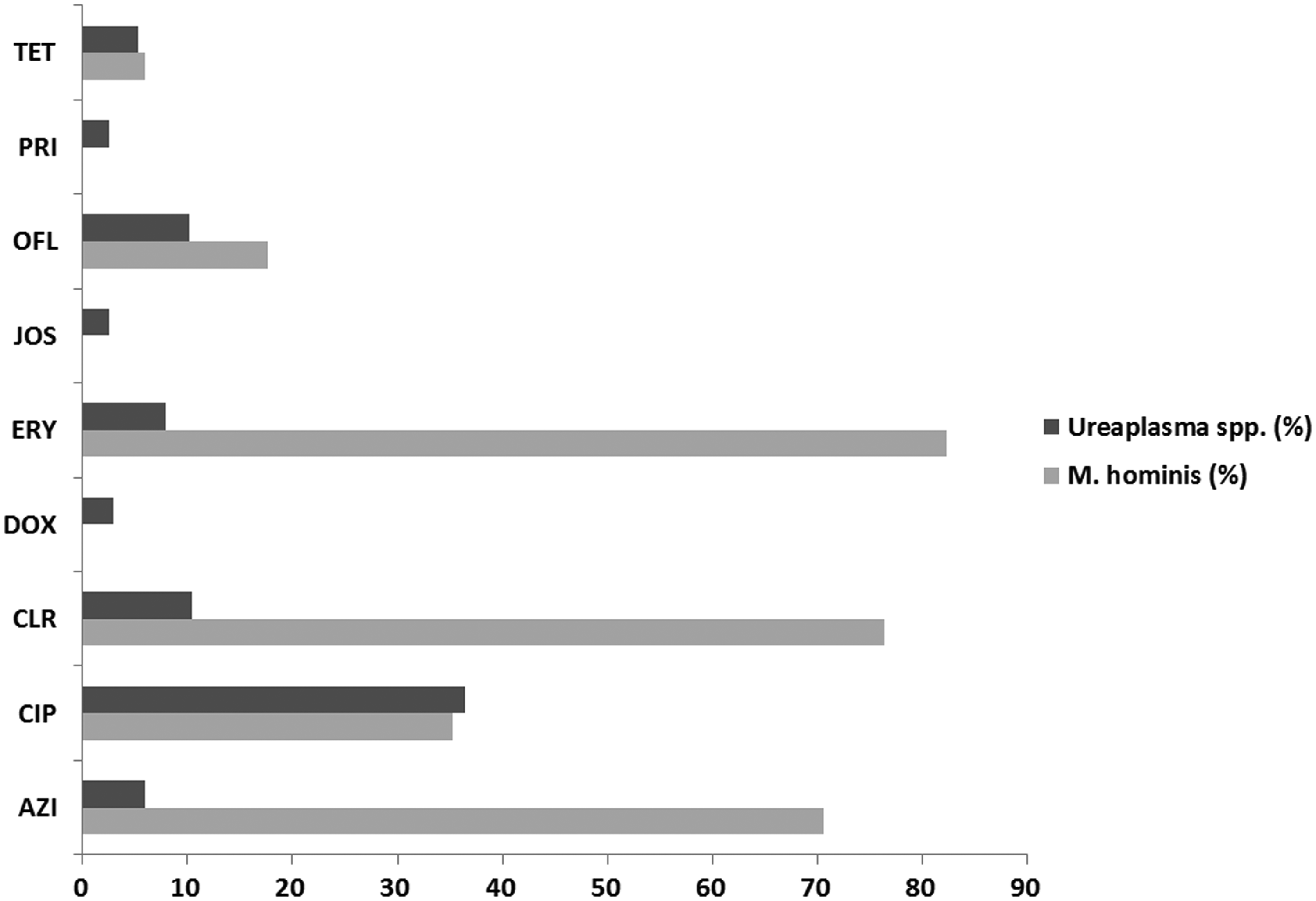
Antibiotic resistance rates of M. hominis and Ureaplasma spp. AZI, azithromycin; CIP, ciprofloxacin; CLR, clarithromycin; DOX, doxycycline; ERY, erythromycin; JOS, josamycin; OFX, ofloxacin; PRI, pristinamycin; TET, tetracycline.
AZI, azithromycin; CIP, ciprofloxacin; CLR, clarithromycin; DOX, doxycycline; ERY, erythromycin; JOS, josamycin; OFX, ofloxacin; PRI, pristinamycin; TET, tetracycline; S, susceptible; I, intermediate; R, resistant.
Discussion
In this study, the rate of urogenital mycoplasmas in asymptomatic individuals was 486 (10.07%) from 2011 to 2015. Of these, 437 (9.06%) were positive for Ureaplasma spp., 17 (0.35%) were positive for M. hominis, and 32 (0.66%) were positive for both. This is a low percentage compared with those found in previous studies in asymptomatic individuals in Korea. Kim et al. reported that the prevalence rates of U. urealyticum and M. hominis were 22.1% (157/709) and 11.6% (82/709), respectively. 21 They used the same type of specimens as our study: first-voided urine specimens were collected from men, and specimens from women were obtained through endocervical swabs by gynecologists.
Despite the similarity of the specimens, there are several reasons for the differences in prevalence between the two studies. First, they used PCR amplification performed with the Seeplex® STD6 ACE detection kit (Seegene, Seoul, Korea), not the Mycoplasma IST2 kit (bioMerieux). In contrast, Kweon et al. reported that the prevalence rates of U. urealyticum, U. parvum, and M. hominis were 9.0% (48/532), 30.8% (164/532), and 5.5% (29/532), respectively, using both kits, but they collected only urine specimens in asymptomatic females. 22 Second, the levels of estrogen in the body and sexual activity are known to be related to the rates of Ureaplasma spp. in women. 23 Therefore, there is a possibility of differences in the age composition of the study participants between the studies. The distribution of the two urogenital mycoplasmas in asymptomatic women was consistent with the results of previous studies from other countries. However, the total positive rates in our study were lower than those of studies from Canada, Australia, and Japan.24–26
Colonization of urogenital mycoplasmas increases in women with increasing sexual contact and the number of sexual partners after puberty.27,28 Previous studies reported that risky sexual behavior and being middle aged were risk factors in women for the development of urogenital mycoplasma infections.8,29 The prevalence of Ureaplasma spp. and M. hominis was highest in those aged 18–40 years and were lower in patients older than 50 years in many reports.20,30,31 Our study also found that a certain relationship existed between mycoplasma infections and the ages of individuals. The highest positive rate of urogenital mycoplasmas was detected in the 30–40 years age group (M. hominis: 41.2%, Ureaplasma spp.: 32.3%, and both Ureaplasma spp. and M. hominis: 12.5%), and it was lowest in women older than 50 years.
M. hominis is known to be resistant to C14- and C15-membered macrolides (erythromycin, azithromycin, and clarithromycin), but susceptible to a C16-membered macrolide (josamycin) and lincosamides (clindamycin and lincomycin). 32 In our study, all M. hominis isolates were susceptible to josamycin, pristinamycin, and doxycycline and were highly resistant to erythromycin, azithromycin, and clarithromycin (82.35%, 70.59%, and 76.47%, respectively) in both sexes, as found in previous studies. 33 In addition, ofloxacin and ciprofloxacin, which have recently exhibited increasing resistance rates, showed rates of 17.65% and 35.29%, respectively. Similar or higher rates of resistance to ciprofloxacin in M. hominis were reported in other countries and even reached 60%.2,15,31 By contrast, our study showed 94.12% susceptibility for tetracycline, but the results of recent studies suggest higher rates of tetracycline resistance, up to 100%.14–16 This discrepancy is believed to be due to the lack of tetracycline use in Korea.
In contrast to M. hominis, Ureaplasma spp. is known to be susceptible to macrolides, but resistant to lincosamides. 1 In our study, Ureaplasma spp. was susceptible to erythromycin, azithromycin, josamycin, doxycycline, and pristinamycin (82.77%, 87.3%, 95.24%, 95.46%, and 97.28%, respectively), as found in previous studies.2,15,31 However, the resistance rate to ofloxacin was 10.20%, and that to ciprofloxacin was 36.51%. This is a lower resistance rate than those of other countries such as Greece (18.02% and 77.48%, respectively) and Serbia (48.6% and 83.8%, respectively).2,15 However, in Korea, Lee et al. analyzed the genital mycoplasmas obtained from 1,035 pregnant women from 2009 to 2014 and reported high resistance rates to ofloxacin and ciprofloxacin of 11.2% and 61.2%, respectively. 34 The increasing rate of resistance to fluoroquinolones can be partly explained by the frequent use of this class of drugs for treating respiratory tract infections such as pneumonia and other urogenital infections. Therefore, fluoroquinolone-based drugs should be avoided in the initial treatment of urogenital mycoplasmas to prevent further increases in resistance to quinolones.
This study has several limitations. First, this study was conducted only for asymptomatic individuals. Thus, further studies are needed about the general public or the symptomatic group. Second, Ureaplasma spp. can be separated by PCR into two species, such as U. urealyticum and U. parvum. U. parvum, which is usually colonized as commensals, can be mistaken for U. urealyticum. Thus, discriminating U. urealyticum and U. parvum is important for treating sexually transmitted infections properly. However, we could not detect U. parvum because the commercial kit used in our study could not detect it. Therefore, it is necessary to conduct PCR to discriminate U. parvum in future research. Third, there are discrepancies among the breakpoints in the Mycoplasma IST2, the Clinical and Laboratory Standards Institute (CLSI) guidelines, and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines.19,35 Thus, resistance rates to ofloxacin are probably underreported using Mycoplasma IST2 when compared to the EUCAST guidelines (R ≥4 vs. R >0.5). On the other hand, resistance rates to erythromycin might be overreported when compared to the CLSI guidelines (R ≥4 vs. R ≥16).
Conclusions
Accurate antimicrobial susceptibility tests are essential for appropriate antibiotic selection in all cases of genital mycoplasmas because Ureaplasma spp. and M. hominis have different antimicrobial susceptibility patterns. The susceptibility of tetracycline remains high in Korea. However, fluoroquinolone-based antimicrobials should be avoided in the initial treatment of urogenital mycoplasmas because of the increasing rates of resistance to quinolones. Thus, the changes in the antibiotic resistance of genital mycoplasmas should be monitored regularly in every country to provide the best treatment in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.