
Abstract
The aim of this study was to investigate the frequency, antimicrobial sensitivity profile, and genetic characteristics of nosocomial strains of extended-spectrum β-lactamase (ESBL)-producing Klebsiella pneumoniae isolated from inpatients at a teaching hospital in Brazil. The bacterial identification, phenotypic detection of ESBL, and antimicrobial susceptibility profile were performed by the VITEK 2 automated system. Matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) mass spectrometry was used to confirm the identity of the species and genotyping of ESBL-producing K. pneumoniae was performed by pulsed-field gel electrophoresis (PFGE). Thirty-six ESBL-producing K. pneumoniae nosocomial strains isolated from November 2013 to August 2014 were analyzed. High resistance rates were observed for ceftriaxone, ceftazidime, cefepime, gentamicin, and ciprofloxacin. However, all isolates were susceptible to amikacin and meropenem. All strains harbored blaCTX-M-like and blaSHV-like genes. Molecular typing by PFGE showed a diversity of genotypes distributed among 25 clusters, but two isolates collected in different wards had the same genotypic profile and carried the same bla genes, so they were considered clones. The data showed that there was a high frequency of ESBL-producing K. pneumoniae multidrug-resistant among patients in the studied hospital. Furthermore, the detection of blaCTX-M-like genes in all isolates suggests that these enzymes are the major ESBL responsible for the beta-lactam resistance phenotypes among the analyzed strains.
Introduction
Infections caused by Klebsiella pneumoniae have increased for the past few years due to their ability to adapt to the hospital environment. Such microorganisms can also disseminate a variety of enzymes, including extended-spectrum β-lactamases (ESBLs), AmpC cephalosporinases, and carbapenemases.1,2
Most of the infections caused by Gram-negative bacilli are associated with the production of ESBL enzymes, which mediate resistance to oxyimino-β-lactams such as cefotaxime, ceftazidime, and aztreonam. 3 Thus, carbapenems such as imipenem and meropenem have been considered traditionally the drugs of choice for treatment of infections caused by ESBL-producing K. pneumoniae. 4 However, K. pneumoniae carbapenemases (KPC)-producing isolates, a diverse group of β-lactamases that are active against the carbapenems, have limited the therapeutic use of these valuable drugs. 5 In this case, colistin and tigecycline (TIG) are the drugs of choice to treat infections caused by multidrug-resistant (MDR) K. pneumoniae. 2 Moreover, bacteria resistant to antimicrobial treatments are quickly selected, causing persistent infections, which may eventually evolve into almost untreatable conditions. 6
In K. pneumoniae, the most prevalent ESBL include TEM, SHV, and CTX-M.7,8 It is noteworthy that CTX-M β-lactamases become one of the most important families of ESBL enzymes worldwide 9 and are predominant type of ESBLs in Europe 10 and South America, 11 including Brazil.12,13 In addition, KPC-producing clinical isolates have been associated with hospital outbreaks in the United States, Europe, Middle East, Asia, and Central and South America. 14 In Brazil, KPC-producing-K. pneumoniae (only KPC-2 variant) have been detected in different regions, 15 including the northeast.16–18
The study of genetic elements involved in antimicrobial resistance and the knowledge of their prevalence among K. pneumoniae clinical isolates are useful tools to generate epidemiological information to prevent the spread of resistant clones. Likewise, an appropriate therapy choice is crucial for better treatment of multiresistant infections. In such cases, the right antibiotic choice aids in decreasing the morbidity and mortality rates, especially in developing countries, where the indiscriminate use of antimicrobial agents is very frequent. Unfortunately, data regarding antimicrobial resistance and its associated mechanisms are scarce in the northeastern Brazilian State of Ceará. Thus, the aim of this study was to investigate the frequency, antimicrobial sensitivity profile, and genetic characteristics of nosocomial strains of ESBL-producing K. pneumoniae isolated from inpatients treated at a teaching hospital in Ceará, Brazil.
Materials and Methods
Bacterial strains
A total of 72 nosocomial strains of K. pneumoniae (single isolate per patient) were isolated from patients admitted to a Brazilian teaching hospital between November 2013 and August 2014. Of these, 42 K. pneumoniae strains were positive for ESBL production by the VITEK 2 automated system (BioMérieux, Marcy-l'Etoile, France) and selected for this study. Clinical samples were collected from patients admitted to neonatal intensive care unit (n = 11; 26.2%), medical wards (n = 9; 21.4%), adult intensive care unit (n = 6; 14.3%), neurology (n = 4; 9.5%), surgical wards (n = 4; 9.5%), pediatric intensive care unit (n = 4; 9.5%), and other hospital unit (n = 4; 9.5%). The first bacterial identification was carried out using the VITEK 2 system. In addition, mass spectrometry was performed, using the Microflex LT MALDI-TOF (Bruker Daltonics, Germany), for confirmation of the first identification at the species level.
Antimicrobial susceptibility testing
The antimicrobial susceptibility profiles of ESBL-positive isolates were performed by the VITEK 2 automated system (BioMérieux, Marcy-l'Etoile, France). In addition, ertapenem-resistant strains determined by VITEK 2 were also evaluated by the Mueller–Hinton agar dilution method (Oxoid, Basingstoke, England), according to the Clinical and Laboratory Standards Institute (CLSI) recommendations. 19 The minimum inhibitory concentration (MIC) to ertapenem were interpreted according to the breakpoints established by the M100-S25 document. 19 Likewise, TIG nonsusceptible isolates determined by VITEK 2 were evaluated by cation-adjusted Mueller–Hinton broth microdilution (BMD) (Oxoid), according to the CLSI recommendations. 19 However, the MIC to TIG was interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) recommendations. 20 The MIC obtained by the methods of agar dilution and BMD were considered the standard reference in relation to the results obtained by VITEK 2. ATCCs Pseudomonas aeruginosa 27853, Escherichia coli 25922, and Staphylococcus aureus 29213 were tested for quality controls.
DNA extraction and detection of bla genes
Total genomic DNA was extracted using the Easy DNA Kit (Invitrogen, Carlsbad, CA) according to the manufacturer's recommendations. The PCR was used to amplify blaCTX-M, 21 blaSHV, 22 blaTEM, 21 and blaGES 23 genes with primers and protocols previously described. All the isolates were also subjected to PCR for blaKPC detection. 24
Molecular typing by pulsed-field gel electrophoresis
The pulsed-field gel electrophoresis (PFGE) was prepared in agarose blocks and genomic DNA was prepared for restriction fragments analyses as described by Pfaller et al. 25 and digested with the restriction enzyme SpeI (New England, Beverly, MA). 25 Electrophoresis was performed on CHEF-DR III (BioRad, Richmond, CA), according to the following conditions: 0.5× TBE Buffer (0.089 M Tris; 0.089 M boric acid; 0.002 M EDTA), 1% agarose, 13°C, 6 V/cm, for 23 h with switch time ramped from 5 to 60 s. The band patterns were interpreted as previously recommended. 25 BioNumerics software (Applied Maths) was applied for dendrogram analysis using 1.0% Dice's similarity coefficient and the unweighted pair-group method using arithmetic averages. Isolates were considered to belong to the same cluster when the similarity coefficient was ≥80%.
Results
Bacterial strains
Among the 42 isolates, 36 (85.7%) were confirmed as K. pneumoniae by matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS), being included in this study. Six (14.3%) isolates (E. coli [n = 4] and Enterobacter cloacae [n = 2]) first identified as K. pneumoniae by VITEK 2 showed discordant data with the MALDI-TOF results, being then excluded from this study. The ESBL-producing K. pneumoniae strains (n = 36) were isolated from blood (n = 9; 25.0%), surgical wounds (n = 8; 22.0%), urine (n = 5; 14.0%), tracheal aspirate (n = 4; 11.0%), anal swab (n = 3; 8.0%), catheter tip (n = 2; 6.0%), and other specimens (n = 5; 14.0%).
Antimicrobial susceptibility testing
According to VITEK 2 results, most K. pneumoniae isolates were nonsusceptible (intermediate and/or resistant) to broad-spectrum cephalosporins such as ceftriaxone (100.0%), ceftazidime (72.2%), and cefepime (69.4%). High resistance rates were also observed for gentamicin (72.2%) and ciprofloxacin (61.1%). All isolates were susceptible to amikacin and meropenem (Table 1). Four isolates initially resistant to ertapenem (11.1%) and 13 nonsusceptible (intermediate or resistant) to TIG (36.1%) by VITEK 2 were categorized as susceptible by agar dilution and BMD cation-adjusted methods, respectively (Tables 2 and 3).
Susceptibility Profile of 36 Extended-Spectrum β-Lactamase-Positive Klebsiella pneumoniae Isolates According to VITEK 2 Results
I, intermediate; R, resistant; S, susceptible.
Agar Dilution Minimum Inhibitory Concentration Determination for VITEK 2 Ertapenem-Resistant Strains
Breakpoints established according to the Clinical and Laboratory Standards Institute M100-S15 document.
ERT, ertapenem; IMP, imipenem; MER, meropenem; MIC, minimum inhibitory concentration.
Broth Microdilution Minimum Inhibitory Concentration Determination for VITEK 2 Tigecycline Nonsusceptible Strains
Breakpoints established according to the technical standard of the National Health Surveillance Agency (ANVISA) No. 01/2013. 19
Breakpoints established according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST). Version 5.0. 2015.
BMD, broth microdilution; TIG, tigecycline.
Detection of β-lactamase genes and molecular typing by PFGE
All K. pneumoniae nosocomial strains evaluated harbored blaCTX-M-like and blaSHV-like genes. Furthermore, 55.6% (n = 20/36) of the isolates carrying the blaCTX-M-like and blaSHV-like also carried blaTEM-like. No blaKPC or blaGES genes were detected. Molecular typing by PFGE showed a diversity of genotypes distributed among 25 clusters, designated I–XXV (Fig. 1). Among them, nine clusters showed the coefficient of similarity ≥80%. In addition, two isolates (KP01 and KP06) collected in different wards showed the same genotypic profile and carried the same bla genes, so were considered to belong to a single strain.
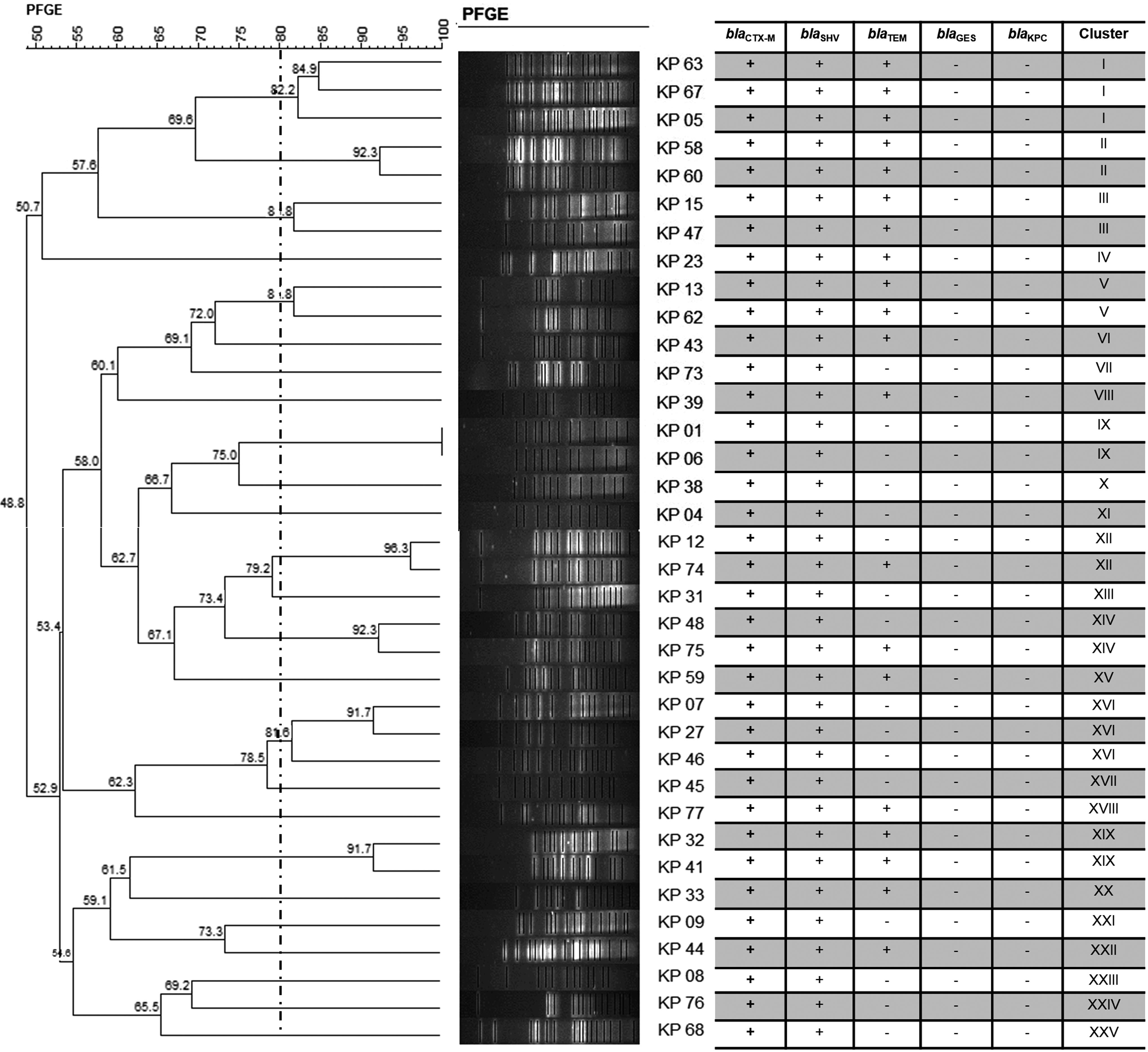
Dendrogram showing genetic relatedness of 36 ESBL-producing Klebsiella pneumoniae (KP) isolates based on pulsed-field gel electrophoresis (PFGE) patterns. Dashed line delineates isolates with Dice coefficient ≥80%.
Discussion
Nosocomial infections caused by ESBL-producing K. pneumoniae strains have been reported in several regions of Brazil.12,18,26 However, there is a lack of information on this topic regarding the population of the State of Ceará, which is composed of 8 million inhabitants. In one of the few studies published, K. pneumoniae was the most frequently found pathogen in patients with infected diabetic foot ulcers, and of the total of 33 K. pneumoniae strains isolated, 7 (21.2%) were identified as ESBL-producing organisms. 27 Other investigation demonstrated that 81.25% of K. pneumoniae strains isolated from blood cultures in the nursery of a hospital located in Fortaleza, Ceará, were diagnosed as ESBL-positive. 28 However, in none of these investigations the bla genes, responsible for the ESBL phenotype, were investigated.
Our findings show that most of the K. pneumoniae isolated from inpatients were resistant to penicillins, cephalosporins, aminoglycosides, and fluoroquinolones. The high rates of resistance to ceftriaxone, ceftazidime, and cefepime are typical of ESBL-producing isolates.12,29 In addition, the detection of blaCTX-M-like genes in all isolates suggests that CTX-M enzymes are the major ESBL responsible for the β-lactam resistance phenotypes in the studied samples. These ESBL enzymes are usually plasmid-mediated but are susceptible to cephamycins such as cefoxitin, and β-lactamase inhibitors such as clavulanate, sulbactam, tazobactam, and carbapenems. 30 CTX-M-producing organisms are a clinical problem worldwide. 9 The results obtained support the recognition of CTX-M as the most prevalent type of ESBL in Brazil, which is in accordance with the data of Europe 10 and South America. 11
In addition, 55.6% of CTX-M and SHV producers also coproduced TEM. The combination of β-lactamases genes observed in the strains of this study may result in therapeutic limitations for the treatment of infections caused by K. pneumoniae in the studied hospital. Moreover, as most of the ESBL-producing strains were resistant to ceftazidime, these results could suggest TEM and/or SHV variants were also ESBL variants because CTX-Ms have very low hydrolytic activity on this antimicrobial.
It is noteworthy that 13 (36.1%, 13/36) isolates classified as nonsusceptible to TIG by VITEK 2 were considered susceptible to TIG when tested with BMD. In recent years, some studies have shown a better performance of BMD than other methods for susceptibility testing to TIG.31,32 Huang et al. 32 showed that from 22.6% (12/53) of ESBL-producing K. pneumoniae isolates that were categorized as resistant to TIG by VITEK 2, only 7.5% (4/53) were confirmed as resistant by BMD method. The authors concluded that VITEK 2 appears to be a suitable method for routine susceptibility testing of TIG only for E. coli isolates, whereas for other Enterobacteriaceae species BMD should be more accurate to determine TIG MICs. 32 Many microbiology laboratories only use VITEK 2 to determine the MIC of TIG, and this method may underestimate the usefulness of this drug in clinical practice. Furthermore, four isolates initially classified as ertapenem resistant by VITEK 2 were also classified as susceptible by the agar dilution method. Therefore, it is conceivable that the results of this study may warn the medical community to the susceptibility profile of ESBL-producing K. pneumoniae determined by VITEK 2 in relation to TIG and ertapenem, collaborating in the choice of appropriate therapy for the treatment of infections caused by this pathogen.
The analysis of genetic similarity of the 36 ESBL-producing K. pneumoniae isolates by PFGE showed a diversity of genotypes distributed among 25 clusters designated I–XXV. Overall, we observed several MDR K. pneumoniae isolates with nonrelated genetic patterns. They may occur due to indiscriminate use of antibiotics, which results in an increase in resistant phenotypes within a group of unrelated isolates, creating an MDR problem in the hospital environment.33,34 Furthermore, the detection of blaCTX-M-like genes in all isolates could be a plasmid spread of CTX-M-encoding genes. This information serves as a warning so that efforts can be directed toward the antimicrobial prescribing policies and they can be reassessed in the studied hospital.
The clonal propagation can be inferred only for the KP01 and KP06 isolates that showed the same banding profile (cluster IX) and had the same bla genes, and so were considered to belong to a single strain. However, these isolates were obtained from patients admitted to different wards. In this case, we believe that the spread of this clone may have occurred due to contact with infected health professionals or after the transfer of patients between hospitals. 34
This study has limitations since it was not possible to determine the CTX-M group carried by each strain, as well as SHV and TEM variants, and the analysis of the plasmid profile was not performed. However, the results obtained in this research can be useful as epidemiological data, and highlight the need for future studies to consider to perform methods that may improve these results and prevent the spread of resistant clones.
Therefore, the detection of blaCTX-M-like genes in all isolates suggests that these enzymes are the major ESBLs responsible for the β-lactam resistance phenotypes in the studied strains and the presence of a clone obtained from patients admitted to different wards reinforces the importance of adopting contact prevention measures in the studied hospital.
Footnotes
Acknowledgments
The authors thank Ana Gales, director of Laboratory Alerta (UNIFESP), for the assistance during this study and technical support for PFGE. Besides that, this study was partly supported by Santa Casa de Misericórdia, Sobral, Ceará, Brazil (Edital DEPE 2014).
Ethical Approval
Ethical approval was obtained from the Research and Ethics Committee of the Vale do Acaraú State University (Opinion 528.783-CEP-UVA).
Disclosure Statement
No competing financial interests exist.