
Abstract
Aims:
Following reports from various doctors regarding increased treatment failure in Helicobacter pylori infection among the Arab population, we decided to make a prospective comparison between the resistance rates of H. pylori in the Arab and Jewish populations in northern Israel.
Results:
Among the Arab population, higher resistance rates were found for clarithromycin and levofloxacin (LEV), as well as a higher rate of multidrug resistance. Rifampin and LEV were found to have higher resistance rates in the village, whereas LEV had a higher resistance rate among women.
Conclusions:
Helicobacter pylori in the Arab population compared with the Jewish population in northern Israel is more resistant to treatment. We assume that these results are caused by overexposure combined with unwise use of antibiotics. A correlation was also found between the type of residence and resistance rates to various antibiotics. Further research is needed to determine the resistance mechanism that may explain these results. Due to the high resistance rate and treatment failure, it is appropriate to consider replacing the standard treatment of H. pylori in these populations.
Introduction
A
Various physicians have noticed that the Arab population is characterized with higher treatment failure rates than the Jewish population and should receive additional antibiotic treatment to eradicate the bacteria. Based on these observations, we decided to compare H. pylori antibiotic resistance between adult Arab and Jewish populations who live in northern Israel. Only limited data regarding differences in antibiotic resistance rates between ethnic groups exist in the literature. For example, one Chinese study found that a certain minority in China has an increased resistance to CLA. 9 A study conducted in Thailand found high prevalence of resistance to MET in mountain people. 10 In the Netherlands, it was also found that ethnicity should be taken into consideration when studying antibiotic resistance. 11 To our best knowledge, this phenomenon has not yet been described in Israel and/or in Arab compared with Jewish populations. In addition, we compared different areas of residence (city, village, and other) and their correlation with antibiotic resistance.
The results of this study will not only give us a better understanding of the overall resistance status in these populations but may also change the standard treatment and provide suitable treatment for each population, while understanding the mechanism of resistance formation and possibly preventing the future spread of resistance.
Materials and Methods
Study population
Two hundred eighteen patients between the ages of 18 and 88 years, residing in northern Israel, who had undergone endoscopy due to abdominal pain or discomfort, from January 2016 to November 2016, were included in the study. The specimens used for this study were gastric biopsy samples collected from 103 Jewish and 115 Arab patients. Since we wanted to compare resistance rates of H. pylori between Arab and Jewish populations, we collected samples from two hospitals: the Jewish patients were admitted to the Poriya Medical Center and the Arab patients were admitted to the Holy Family Hospital in Nazareth. None of the patients received antibiotic treatment during the month preceding the gastroscopy procedure. All patients were treated with CLA, AMO, and PPIs according to the standard treatment protocol for H. pylori infection.
All patients were Israeli residents and had not recently migrated to Israel. We divided the participants into three groups according to their type of residence: city, village, and other. In Israel, a city is usually defined by having over 20,000 inhabitants. A village is defined by fewer inhabitants and less population density. Other was defined by way of negation—any area of residence that is not a city or a village.
The study was approved by the institutional review board, and informed consent was obtained from all study participants.
Bacterial culture
All biopsy specimens were placed in sterile Eppendorf tubes containing 1 mL sterile physiological solution (0.9% NaCl) and were sent to the Clinical Microbiology Laboratory in the Poriya Medical Center. Biopsies were minced manually with a sterile scalpel and seeded on Modified BD Helicobacter Agar (BD Diagnostics, Sparks, MD) and blood agar (Hylabs, Rehovot, Israel). The plates were incubated for 7 days at 37°C in a micro-aerobic atmosphere produced by a gas generating system adapted for Campylobacter (Campy-Gen™; Gamidor Diagnostics). If no bacterial growth was seen after 7 days, an additional 3 days of incubation were added. H. pylori was identified based on Gram-staining followed by oxidase, catalase, and urease tests. Final identification was performed using matrix-assisted laser desorption ionization–time of flight mass spectrometry (Bruker Daltonics, Bremen, Germany).
Determination of minimum inhibitory concentration
Colonies from primary plates were suspended in 0.46% NaCl solution until a 3.0 McFarland turbidity was generated. These suspensions were seeded on Etest (bioMérieux, Durham, NC). Müller–Hinton agar with 10% horse blood (Hylabs) and Etest strips (bioMérieux) of AMO, TET, CLA, MET, LEV, and RIF were added. These antibiotics are part of the standard treatment protocols for the first-line treatment and following treatment failure. 8
The plates were incubated for 72 h at 35°C in micro-aerobic atmosphere condition. Minimum inhibitory concentration 90 (MIC90) was determined as the antibiotic concentration that inhibited 90% of the bacterial growth (inhibited a visible growth of a microorganism).
Interpretation of susceptibility tests results were performed in accordance with the British Society for Antimicrobial Chemotherapy 2015. 11 For MIC quality control, H. pylori ATCC 43504 strain was used.
Statistical analysis
Correlation between a categorical variable (Jewish/Arab or city/village/other) and another categorical variable (sensitive/resistant) was analyzed using chi-square test to examine statistical dependence between variables.
The nonparametric Wilcoxon–Mann–Whitney rank sum test for independent samples was applied for analyzing the differences in distribution of continuous parameters (MIC) between categorical variables.
All tests were two-tailed. Statistical significance was determined with p < 0.05. The statistical analysis was performed using SPSS 17 software (SPSS, Inc., Chicago, IL).
Results
Two hundred eighteen patients were enrolled in the study (mean age 42 years); 103 Jewish patients (mean age 40 years) and 115 Arab patients (mean age 43 years); 67 were male (39 Jewish, 28 Arab patients) and 151 were female (64 Jewish, 87 Arab patients).
Of 218 subjects, 18 (8.25%) isolates were resistant to AMO (mean MIC 0.12 mg/L), 44% to CLA (mean MIC 3.69 mg/L), 4.6% to TET (mean MIC 2.5 mg/L), 3.2% to RIF (mean MIC 2.29 mg/L), 7.8% to LEV (mean MIC 2.33 mg/L), and 23.9% to MET (mean MIC 12.77 mg/L) (Table 1).
Distribution of Antibiotic-Resistant Isolates in Arabs Compared with Jews
Bold, statistically significant (p < 0.05).
AMO, amoxicillin; CLA, clarithromycin; TET, tetracycline; RIF, rifampicin; MET, metronidazole; LEV, levofloxacin.
When analyzing the differences in resistance rates between Arab and Jewish populations, only CLA and LEV resistance rates were statistically different. Among the Arab population, 62 (53.9%) isolates were resistant to CLA (mean MIC 4.2 mg/L) compared to 34 (33%) isolates in the Jewish population (mean MIC 2.75 mg/L) (p = 0.0019) (Fig. 1). In addition, eight (7%) Arab-derived isolates were resistant to LEV (mean MIC 2.37 mg/L) compared with one (0.97%) Jewish-originated isolate (mean MIC 2 mg/L) (p = 0.018).
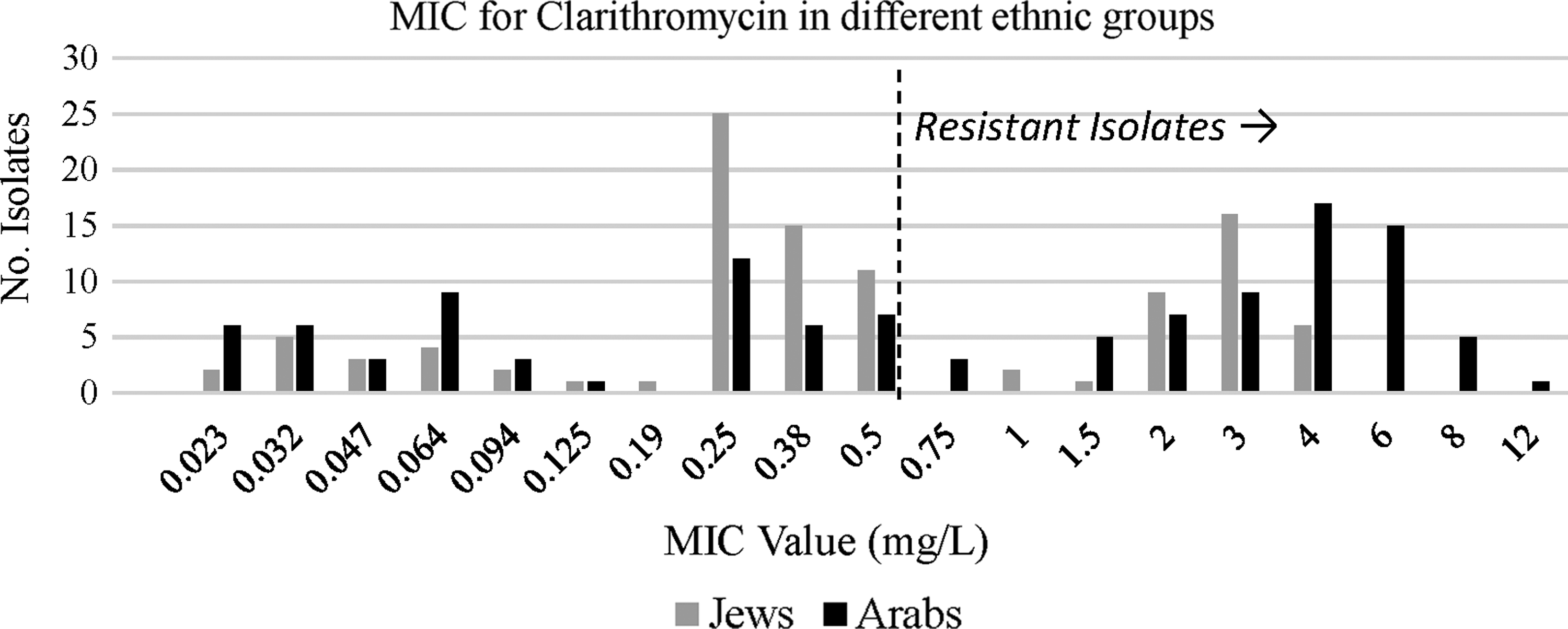
MIC distribution for clarithromycin among Jewish and Arab patients. MIC, minimum inhibitory concentration.
We further looked for multidrug-resistant (MDR) isolates (Table 1). We found a total of 49 isolates with a double drug resistance (22.5%); we noticed more Arab-derived isolates (29.56% of Arab population) than those of Jews (14.56% of Jewish population). CLA and MET double resistance was the most common combination overall and among Arab population with 11.47% and 18.26%, respectively. Only 3.88% of the Jewish population showed this kind of resistance (p = 0.0009). CLA and AMO resistance was the most common combination among Jews (5.83%), but a similar number was found among Arabs (5.22%). A triple drug resistance was found only in the Arab population with 6.96% of isolates.
Next, we wanted to test whether there are differences in resistance rates with correlation to gender. We found a statistically significant difference between males and females in LEV resistance rate (Table 2); although no isolate from the male group was LEV resistant, 100% of female isolates were LEV resistant (p = 0.0413). When we looked for differences between males and females among each population, only AMO resistance rate was statistically different and only among the Arab population (data not shown); although 5 (17.85%) of 28 isolates from the male Arab group were AMO resistant, 5 (5.74%) of 87 isolates from the female group were resistant (p = 0.0479).
Distribution of Antibiotic Resistance by Gender and Area of Residence
Bold, statistically significant (p < 0.05).
The correlation of different types of resistance with antibiotics resistance was also tested (Table 2). Among RIF-resistant isolates, one originated from patients living in a city (14.3%), three in a village (42.86%), and three in other (42.86%) (p = 0.0463). Among LEV-resistant isolates, three came from patients who live in a city (33%), four in a village (44%), and two in other (22%) (p = 0.018).
The mean MIC was calculated for each type of residence: in the city population (n = 94), in the village population (n = 29), and in the other population (n = 95) for each type of antibiotic. As shown in Fig. 2, the mean MIC for AMO was 0.15 mg/L in city, 0.26 mg/L in village, and 0.1 mg/L in other (p = 0.0487). The mean MIC for RIF was 0.13 mg/L in city, 0.36 mg/L in village, and 0.15 mg/L in other (p = 0.0428). The mean MIC for LEV was 0.14 mg/L in city, 0.39 mg/L in village, and 0.06 mg/L in other (p = 0.0176).

Mean MIC for amoxicillin, rifampicin, and levofloxacin among patients living in city, village, and other settlement.
Discussion
Helicobacter pylori is the most common chronic bacterial infection in humans and a major cause of gastrointestinal symptoms for many patients. 10 Its high infection rate and its increasing resistance to antibiotics pose a therapeutic challenge. 12 The most likely means of transmission are oral/oral and fecal/oral.13,14 As several doctors in northern Israel have noticed that more Arab patients returned for a second treatment after initial treatment has failed, we decided to conduct this research. Factors associated with treatment failure include poor patient compliance and resistance of the patient's H. pylori strain to prescribed antibiotics. In the current study, we found that isolates from Arabs were more resistant to both CLA and LEV and had more resistance to several antibiotics simultaneously (MDR). High resistance rates in the Arab population may be caused by different cultural behavior and poorer knowledge regarding antibiotics and their mechanism of action, leading to antibiotic overuse or misuse compared with the Jewish population.15–17 A specific mutation leading to CLA resistance is well known, and it may explain the higher resistance rate in the Arab population, but further research is needed in this specific population. 18 Another assumption is that the Arab population does not complete the full antibiotic course of treatment, thus not fully eradicating H. pylori—although this hypothesis also needs further research. Additionally, the extent of crowding in the Arab villages is higher than that in the city, with an emphasis on the number of family members living inside the same house. Such density, which is characteristic of Arab society, can contribute to the easier transfer of resistant strains of H. pylori, thereby increasing the rates of resistance in the whole population. Future research should examine the phylogenies of the resistant bacteria and confirm whether they came from the same clone that has spread, a fact that will reinforce this hypothesis.
The male–female resistance differences may be explained by the different use of antibiotics by each gender. For example, urinary tract infections (UTIs) are much more common in females, and therefore, this population is more prone to antibiotic resistance for antibiotics that are used to treat this kind of infection. LEV is a good example of such an antibiotic and may explain our results, which indicate a higher resistance rate in females. The higher resistance for AMO among Arab men can be explained by behavior overuse and not by medical indication since this resistance in men does not exist in the Jewish sector and there are no special medical indications that may cause the overuse of this antibiotic among men (like the UTI example in women).
Bacterial resistance in different areas of residence is not well described in this geographical area. This study found that resistance to RIF in the city was lower than that in the village and in other forms of residence. H. pylori was found to be very resistant to LEV in the village, but more sensitive in the city and in other. One explanation for these results is the denser living form of the village that may contribute to the oral/oral and oral/fecal transmission of resistant bacteria. A second explanation is the different antibiotic consumption habits in each residential area. For example, a massive use of LEV in the village may lead to high resistance. One of the current research's limitations is that no data concerning treatment compliance was collected; further research may provide answers to our assumptions.
It is important to note that there is no constitutional definition in Israel for cities and villages. The term village usually refers to a small Arab residential area, and sometimes a village resembles other, more advanced, forms of residence.
In light of our results and other work, 19 further studies are needed to confirm our assumptions or to find other explanations for these variations in antibiotic resistance among populations and types of residence. These studies should focus on compliance with antibiotic treatment, which antibiotic has been taken in recent years, and the unnecessary use of antibiotics as a treatment for diseases that do not require antibiotic treatment. Physicians should consider replacement of the first-line treatment according to the specific resistance of the population and the patient's area of residence.
Ethics Approval and Consent to Participate
The study was approved by the Helsinki Committee of Baruch Padeh Medical Center, Poriya, and Holy Family Hospital. Informed consent was obtained from all study participants. The article was written as part of the requirements of the School of Medicine in the Galilee.
Footnotes
Disclosure Statement
No competing financial interests exist.