
Abstract
The prevalence of nontuberculous mycobacteria (NTM) has increased in tuberculosis (TB)-suspected clinical samples. These bacteria are now recognized as important emerging pathogens, which affect both immunocompetent and immunocompromised individuals. The aim of this study was to evaluate the frequency of NTM in clinical samples and to efficacy of genomic loci as targets for detection of NTM species. This cross-sectional study was performed on 8166 clinical samples to determine the presence of NTM species from April 2013 to December 2015. The phenotypic methods were applied for preliminary NTM identification. The PCR-RFLP assay of heat shock protein-65 (hsp-65) gene and multilocus sequence analysis based on 16S–23S internal transcribes spacer (ITS), rpoB, and 16S rRNA genes were applied for species identification. In a total of 520 isolates from TB-suspected cases, 61 samples (11.7%) were identified as NTM. Overall, Mycobacterium (M.) fortuitum (63.9%) was the most frequently encountered species, followed by M. kansasii (9.8%), M. simiae (9.8%), M. abscessus (6.7%), M. gordonae (4.9%), M. flavescens (3.3%), and M. setense (1.6%). Moreover, sequencing of 16S rRNA and rpoB genes could identify all NTM species. In conclusion, we showed that the samples were infected by six NTM species, and M. fortuitum was the most frequent NTM strain. Based on the findings, 16S rRNA and rpoB genes were superior to ITS gene in identification of NTM species.
Introduction
N
In Iran, as a developing country, tuberculosis (TB) remains one of the major public health concerns. By improving the identification techniques, the rate of NTM infection has rapidly increased over the past decades. 3
In some countries, absence of specific diagnostic techniques for NTM detection also hinders the evaluation of NTM diseases. On the other hand, in countries where the incidence of TB is high, a positive smear for NTM may be misinterpreted as TB. In addition, explanations for NTM infection or disease have been inconsistent for many years, thereby complicating the assessment and comparison of epidemiological trends for NTM infection.2,4
The national surveillance reports of NTM disease are not common. Some countries have even failed to conduct any systematic report of the incidence and isolation of NTM species; therefore, assessment of geographical distribution can be challenging. The results of several studies have shown that distribution of NTM species varies from one country to another, thus affecting the local incidence and clinical manifestations of NTM infection.5,6 In addition, a correlation has been proposed between the increased incidence of NTM disease and decreased incidence of TB in adults, although no causality relationship has been confirmed.7,8
Phenotypic methods of NTM detection, such as biochemical tests and analysis of growth characteristics, are cumbersome and time-consuming; also, interpretation of the results can be confusing.9,10 Consequently, several molecular approaches have been designed for NTM detection to overcome the limitations of phenotypic tests. Gene sequence analysis is considered the gold standard for the detection of NTM species. The 16S rRNA gene is often used for identification of Mycobacterium species and is considered a priority in sequence analysis. However, this gene has a highly similar sequence in different types of NTM; therefore, it is not possible to detect closely related species. To compensate for this limitation, the use of other genes, including heat shock protein-65 (hsp-65), 16S–23S rRNA internal transcribed spacer (ITS), and rpoB for reliable detection of NTM, is necessary.10–12
In the recent years, several methods for rapid NTM detection have been developed and evaluated, such as the BacT/Alert 3D unit, QMAP Dual-ID test, Quantamatrix Multiplexed Assay Platform (QMAP) test, and VersaTREK® system (Thermo Fisher Scientific), which need expensive substance and equipment. It is therefore impossible to use these tests in most developing countries. 13
With this background in mind, the primary objective of this study was to assess the frequency of different NTM species from clinical samples and evaluate the efficacy of genomic loci (hsp65, 16S rRNA, ITS, and rpoB) as targets for detection of NTM species.
Materials and Methods
Sample collection
This cross-sectional study was performed from April 2013 to December 2015 on a total of 8166 TB-suspected clinical samples at the Department of Mycobacteriology and Pulmonary Research of Pasteur Institute of Iran (PII). This study was in compliance with the 1975 Declaration of Helsinki and local regulations. It was also approved by the Ethics Committee of PII (IR.PII.REC.1394.54). Written informed consents were obtained from all suspected patients. The suspected samples were processed with N-acetyl-l-cysteine-sodium hydroxide assay.14,15
The standard strains used in this study
The reference strains of Mycobacterium (M.) tuberculosis (CRBIP7.11), M. bovis (CRBIP7.121), M. scrofulaceum (CRBIP7.163), M. avium (CRBIP7.142), M. simiae (CIP104531), M. chelonae (CIP104535), M. kansasii (CRBIP7.98), M. fortuitum (CRBIP17.99), M. gastri (CIP104530), M. flavescens (CIP104533), M. xenopi (CIP104035), M. gordonae (CIP104529), M. aurum (CIP104482), M. intracellulare (CRBIP7.168), M. nonchromogenicum (CIP106811), and M. terrae (CIP104321) used in this study were provided by Pasteur Institute of France.
Phenotypic and biochemical tests
All NTM isolates were tested in terms of growth rate on Löwenstein-Jensen (LJ) medium, growth at temperature of 25°C, 32°C, 37°C, and 42°C, macroscopic and microscopic morphological characteristics, arylsulfatase and urease production, tween-80 hydrolysis, nitrate reduction, tellurite reduction, salt tolerance, and semiquantitative catalase production, according to the Centers for Disease Control procedures. 14
DNA extraction and molecular analysis
Bacterial DNA was extracted using High Pure PCR Template Preparation kit (Roche Diagnostics Deutschland GmbH, Mannheim, Germany). A 441-bp fragment of hsp65 gene was amplified by two specific primers, TB11 and TB12, and then, the PCR products were digested by BstEII and HaeIII restriction enzymes. 16
A 750-bp specific region of rpoB gene was amplified and sequenced using two primers, that is, F-(5′-GGCAAGGTCACCCCGAAGGG-3′) and R-(5′-AGCGGCTGCTGGGTGATCATC-3′), as described by Adékambi and colleagues. 17
The ITS primers, F-(5′-AAGTCGTAACAAGGTARCCG-3′) and R-(5′-TCGCCAAGGCATCCACC-3′), were used to amplify a fragment of ∼230–350 bp in the ITS region. 18 Also, a 1500-bp fragment of 16S rRNA gene was amplified from the isolates using primers, pA (5′-AGAGTTTGATCCTGGCTCAG-3′) and pI (5'-TGCACACAGGCCACAAGGGA-3′), as previously described. 19
In addition, the AccuPrep® PCR purification kit (Bioneer, Seoul, South Korea) was used for purification of PCR products. Subsequently, an ABI Automated Sequencer (Applied Biosystems, Foster City, CA) was used for sequencing the PCR products. The results of PCR sequencing were analyzed using MEGA version 6.0 software. 20
Molecular detection of Mycobacterium tuberculosis complex
The IS6110-based PCR assay was used for differentiation of Mycobacterium tuberculosis complex (MTC) and NTM species in positive cultures. A 123-bp fragment of insertion sequence 6110 (IS6110) gene was amplified from MTC, using the described PCR primers. 21 M. kansasii (CRBIP7.98) and Mycobacterium tuberculosis (CRBIP7.11) were used as the negative and positive controls, respectively.
Accession numbers of nucleotide sequences
The GenBank accession numbers of NTM isolates, submitted in this study, were as follows: MF471847 to MF471906 for rpoB gene, MF472649 to MF472708 for 16S rRNA gene, and MF479200 to MF479258 for ITS gene.
Results
Patient characteristics
A total of 8166 TB-suspected samples were evaluated in this study. Overall, 520 (6.4%) samples were positive for acid-fast bacilli, based on the culture method. Out of 520 positive culture samples, 459 (88.3%) were confirmed as MTC, using biochemical and molecular tests. In addition, 61 (11.7%) samples were identified as NTM, based on the guidelines by the American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA). No mixed infection of Mycobacterium was observed in patients (Fig. 1).

Flowchart of population study and isolation. LJ, Löwenstein-Jensen medium; MTC, Mycobacterium tuberculosis complex; NTM, nontuberculous mycobacteria.
Among 61 NTM samples, 56 (91.8%) and five (8.2%) were from pulmonary and extrapulmonary sites, respectively. The pulmonary samples included 51 (83.6%) sputum and five (8.3%) bronchoalveolar lavage. Among extrapulmonary samples, NTM were identified in two (3.3%) skin, one (1.6%) urine, one (1.6%) pus, and one (1.6%) lymph node samples. In addition, coughing, phlegm, fever, weight loss, and night perspiration were the most common signs and symptoms. The average age of NTM patients was 49.6 ± 16.6 years, and 37 (60.7%) patients were male. Also, six (9.8%) and nine (14.8%) had cystic fibrosis (CF) and human immunodeficiency virus (HIV), respectively (Table 1).
HIV, human immunodeficiency virus; NTM, nontuberculous mycobacteria; AFB, acid-fast bacilli; SD, standard deviation.
NTM species detection by biochemical test
According to the growth rates, NTM strains were classified into two groups. In total, 44 (72.1%) clinical isolates were rapidly growing mycobacteria (RGM), while 17 (27.9%) isolates were slowly growing mycobacteria. Based on the biochemical tests, M. fortuitum (39 isolates) was the most frequent strain, followed by M. kansasii (six isolates) and M. simiae strains (six isolates). Among 61 isolates examined in this study, only 51 (83.6%) strains were detected by biochemical tests and the remaining isolates were unidentifiable (Table 2).
PRA, PCR restriction analysis.
NTM species detection by molecular tests
PCR restriction analysis of hsp65 gene
Based on the PCR restriction analysis (PRA) identification of hsp65, an identical pattern was detected for the isolated microorganisms from every patient. According to the hsp65-PRA results, M. fortuitum (39 isolates) was the most frequently encountered (63.9%), followed by M. simiae (six isolates), M. kansasii (six isolates), M. abscessus (four isolates), and M. gordonae I (three isolates). One (1.6%) isolate showed unknown pattern (Table 2).
Multilocus sequence analysis of 16S rRNA, rpoB, and ITS genes
All NTM isolates were recognized using molecular methods by sequencing ITS, 16S rRNA, and rpoB genes (Fig. 2A–C). Seven different species were recognized. Sequencing of rpoB and 16S rRNA genes could identify all species (Fig. 2A, B), while sequencing of ITS gene could not identify only one species (M. setense) (Fig. 2C). There was a strong association between 16S rRNA and rpoB genes. The clinical isolates included M. fortuitum (63.9%), M. kansasii (9.8%), M. simiae (9.8%), M. abscessus (6.7%), M. gordonae (4.9%), M. flavescens (3.3%), and M. setense (1.6%) (Table 3).
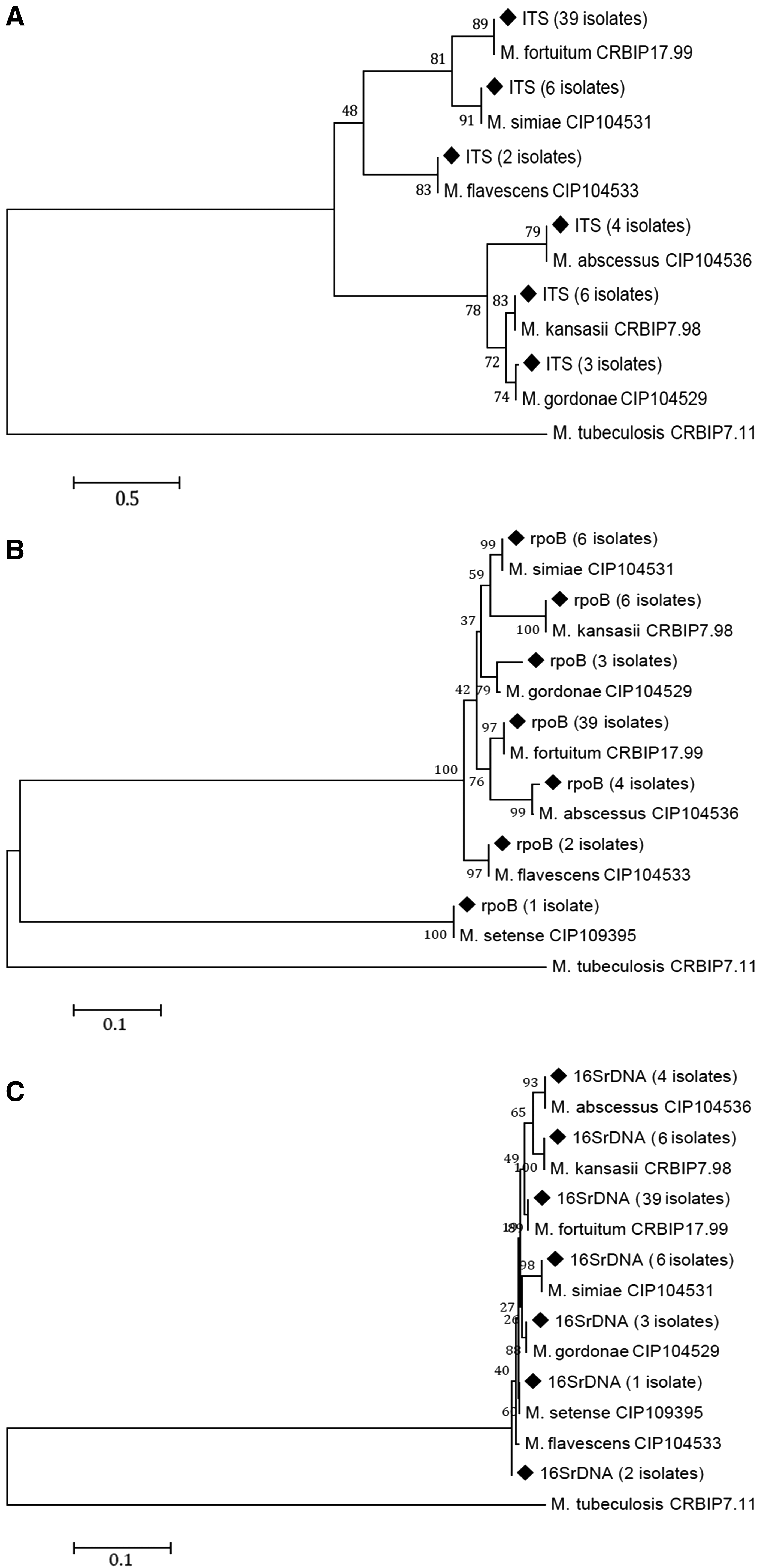
The phylogenetic trees constructed by the ITS
MLSA, multilocus sequence analysis.
Discussion
NTM infection is an emerging public health concern, especially in developing countries. NTM and MTC are found responsible for different pulmonary and extrapulmonary (skin and soft tissue, and disseminated) infections. This study addressed the frequency of different NTM species and their genetic diversity, using ITS, rpoB, and 16S rRNA sequence analysis in pulmonary and extrapulmonary samples from an Iranian population.
We indicated, in Iran, that an unexpected number of patients who sought diagnosis and treatment for M. tuberculosis was infected by NTM, especially M. fortuitum. This result is in agreement with previous studies of an increased frequency of NTM and the difficulty in distinguishing pulmonary M. tuberculosis and NTM based on clinical symptoms.22,23
In Iran, where the incidence of TB has declined over the years, NTM species are being increasingly recognized as human pathogens. This may be clearly explained by the improved identification of NTM infections as clinical phenomena, as well as advances in laboratory methods.10,23,24
Our findings indicated that ITS gene sequencing alone cannot be applied as an efficient method for the detection of NTM species, such as M. setense.
Based on 16S rRNA and rpoB sequences, all the clinical isolates could be identified more accurately. These findings are in disagreement with other studies by Hashemi-Shahraki et al. and Dastranj et al., which revealed poor discrimination of M. kansasii by 16S rRNA gene.25–27 Also, the results of this study showed that although the ITS gene showed valuable sensitivity and specificity, it was limited to the identification of a small number of NTM species. Comparison of these genes indicated that 16S rRNA and rpoB genes had a greater identification potential compared to the ITS gene.
Among 61 NTM isolates from the clinical samples in our study, 63.9% were classified as M. fortuitum. This organism is widely distributed in environmental samples, such as soil and water. It seems that M. fortuitum is transmitted from environmental sources to humans. 3
The clinical manifestations are diverse and include local cutaneous diseases, osteomyelitis, joint infections, lymphadenitis, and disseminated disease. 28 Due to the absence of biochemical characteristics, clinical diagnosis of RGM is challenging. 29 Prevalence rates of M. fortuitum have been reported in different regions around the world, including Turkey (33.9%), the Czech Republic (17.5%), Switzerland (17.5%), Portugal (16.5%), Germany (12.2%), Spain (10.8%), Finland (6.7%), France (6.5%), the United Kingdom (6.0%), Denmark (5.3%), Italy (2.5%), and Belgium (2.1%).2,29 Also, in our previous study, we indicated the high prevalence of M. fortuitum in Iran. According to these findings, M. fortuitum is the most frequent RGM in Iran and Turkey. Therefore, further attention should be directed toward this organism, as RGM species are highly resistant to disinfectants, antibiotics, and antiseptics. 30
Several studies have shown that M. simiae is the most frequent NTM isolate in respiratory specimens.24,31,32 These findings are inconsistent with our study, where M. fortuitum was the most prevalent NTM species in respiratory samples. On the other hand, based on our study, M. simiae was the second most frequent NTM in the clinical samples, and the importance of M. simiae strains was highlighted in this study.
M. simiae may have similar clinical and radiological features to TB, and may be therefore confused with M. tuberculosis. 31 In this study, patients infected by M. simiae had been diagnosed with TB and received anti-TB drugs, without showing any response. As previously reported, it seems that NTMs, such as M. simiae, should be sought rigorously in patients who are unresponsive to anti-TB therapy. 33
M. simiae infection is uncommon among immunocompetent patients, while it is more frequent among immunodeficient patients, such as individuals with respiratory diseases and HIV infection. 34 Four out of six M. simiae-positive patients were HIV positive, three of whom had disseminated disease; this finding is in consistence with previous reports.24,35 The clinical and radiographic features, as well as the applicability of phlegm-based diagnostic methods, may vary among HIV-negative and HIV-positive patients; these factors further complicate the management of patients with HIV and M. simiae coinfection.2,36
In more than 150 confirmed species of NTM, M. avium complex, M. abscessus complex, and M. kansasii are the most frequent human pathogens. 37 Besides M. simiae, M. kansasii was the second most frequent NTM in our clinical samples. Traditionally, M. kansasii has been known as the most virulent NTM species. It is believed that the presence of a single M. kansasii isolate in a sputum sample is clinically significant, especially in HIV-positive patients, 2 although this finding has not been confirmed. 38 Furthermore, a relatively high prevalence of M. kansasii pneumonia has been indicated in highly industrialized regions of Europe and Iran, and pneumonia caused by M. kansasii is probably associated with air pollution in large polluted cities, such as Tehran, Iran.10,39
M. abscessus was the third most frequently recovered NTM pathogen in this study. Several studies have shown that M. abscessus is responsible for most lung diseases caused by RGM. The largest group of patients with this organism consisted of females, nonsmokers, and patients above 60 years; they also had underlying disorders, such as CF and HIV. 2 In consistence with these reports, our study showed that two patients with M. abscessus had HIV coinfection and one patient had CF. Moreover, three out of four patients were female, while all were nonsmokers. Overall, treatment of pulmonary diseases caused by M. abscessus complex is very difficult. In addition, evidence of hospital transmission and prevalence of M. abscessus are increasing; therefore, more attention should be paid to this organism. 40
In this study, we identified M. setense in a 39-year-old woman with HIV infection, who was hospitalized for persistent subcutaneous pus in her right foot. M. setense, as a new and rare Mycobacterium, was isolated from a patient with a posttraumatic lesion of the foot, complicated by osteitis and tenosynovitis. 41 More recently, three infections due to M. setense (a man with a knee joint replacement, an HIV-positive young woman with a subcutaneous abscess, and a renal transplant recipient under immunosuppressive therapy) have been reported in Iran. Also, M. setense, despite its rarity, can infect immunocompromised and healthy subjects. 42
It should be noted that increased sensitivity due to HIV infection, underlying pulmonary diseases, malignancies, relative immunodeficiency, or exposure to occupational dust may lead to NTM infection.22,23 The increasing prevalence of NTM infections in Iran may have several negative effects on public health. On the other hand, most TB laboratories in Iran are not equipped to perform mycobacterial culture or NTM detection studies; as a result, NTM infections are often diagnosed as multidrug-resistant TB. Negligence of NTM infection results in unnecessary anti-TB treatments, unsuitable application of high-cost care and treatment, stigmatization of patients, and important social and economic consequences. 23 Therefore, due to the increasing importance and prevalence of NTM species, rapid and reliable detection is important as an effective management strategy for patients.
In conclusion, we identified six NTM species in this study. M. fortuitum was the most frequent NTM species, and M. setense, as a rare NTM species, was reported for the second time in Iran. Finally, 16S rRNA and rpoB genes were more effective than ITS gene in identification of NTM species; however, multilocus sequence analysis. could be useful in the detection of NTM species in reference laboratories. Future studies are necessary to determine the epidemiology of NTM in Iran, to develop reliable laboratory methods for NTM identification, and to promote the awareness of Iranian physicians for the diagnosis and treatment of NTM species.
Footnotes
Acknowledgments
The authors would like to thank TB staff members from the Department of Mycobacteriology and Pulmonary Research, Pasteur Institute of Iran.
This study was funded by a grant from the Pasteur Institute of Iran, Tehran [no. 866].
Disclosure Statement
No competing financial interests exist.