
Abstract
Spread of multidrug-resistant pathogenic bacteria became one of the greatest threats in healthcare worldwide. It is generally accepted that both inter- and intrahospital transmissions of these bacteria contribute significantly to this problem. The purpose of the current study was the evaluation of the inter- and intrahospital spread of multidrug resistant Gram-negative pathogenic bacteria in Lithuania. Clinical isolates of Acinetobacter sp., Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa were subjected for the screening for extended spectrum β-lactamase, carbapenemase, as well as plasmid-mediated AmpC β-lactamase genes. BOX-PCR genotyping was used for the genotyping of these isolates. Our results show that all four pathogens are involved in the intra- and/or interhospital dissemination between the Lithuanian healthcare institutions. The level of transmissions differed between pathogens, and the worst situation was detected for Acinetobacter sp. followed by E. coli. In almost all cases, transmissible strains had at least one gene conferring β-lactam resistance, thereby contributing to the dissemination of the resistance determinants in and between Lithuanian hospitals. Our study clearly demonstrated that immediate actions, more effective strategy, and surveillance are needed to confine and prevent further spread of multidrug resistant Gram-negative pathogenic bacteria in Lithuanian healthcare institutions.
Introduction
The emergence and spread of drug-resistant pathogenic bacteria became one of the greatest threats in healthcare worldwide. It is generally accepted that the spread of these bacteria is associated with the referral of patients between hospitals and other healthcare institutions within the same country.1,2 Modern centralized healthcare systems promote this process. 3 In contrast, interinstitutional transmission also contributes significantly to the spread of antimicrobial resistance. 3 The local and national surveillance is considered to be an important component of the strategy to prevent the spread of drug-resistant bacteria. 4
It should be noted that different strains of a single pathogenic species can be distributed differently in community and healthcare institutions; they can also differ in their level of virulence, as well as susceptibility to antimicrobials. Therefore, it is very important to discriminate these strains to determine the ways of their transmission and to design highly efficient surveillance systems both at the hospital, as well as at the national level. 4 The development of genotyping methods has provided new tools for better surveillance. 5 One of the most highly discriminatory strain-specific methods is a repetitive element PCR (rep-PCR) that amplifies regions of DNA flanked by the repetitive elements, leading to multiple amplicons of different sizes.5,6
In this study, we used one of the rep-PCR methods—BOX-PCR—for the genotyping of clinical isolates of Acinetobacter sp., Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa from the different Lithuanian hospitals to evaluate the intra- and interhospital spread of these drug-resistant pathogenic bacteria. To the best of our knowledge, this study is the first evaluation of such transmissions in Lithuania.
Materials and Methods
Bacterial isolates
E. coli and K. pneumoniae resistant to third generation cephalosporins, as well as Acinetobacter sp. and P. aeruginosa resistant to carbapenems, were isolated from blood samples in 14 clinical microbiological laboratories (A, B, C, D, E, F, G, I, J, L, M, N, O, and R), which provide services to 56 healthcare institutions in the different regions of Lithuania. Each clinical microbiological laboratory provides services to a few particular healthcare institutions, except the laboratories J and L that provide services to a single hospital each. The overlapping service of the laboratories is unavailable and impossible.
Phenotypic evaluation of β-lactam susceptibility
We investigated 109 E. coli and 179 K. pneumoniae isolates resistant to third generation cephalosporins, as well as 20 isolates of Acinetobacter sp. and 11 isolates of P. aeruginosa resistant to carbapenems. The susceptibility of bacteria was analyzed by a disk diffusion method (BioMaxima, Poland) and a gradient method (E test; bioMerieux, France). The phenotypic evaluation of cefotaxime, ceftriaxone, ceftazidime, meropenem, and imipenem–cilastatin susceptibility was conducted according to the European Committee on Antimicrobial Susceptibility testing guidelines 2016. 7
Screening for antibiotic resistance genes
All Gram-negative clinical isolates were subjected for the screening for antibiotic resistance genes. Screening for extended spectrum β-lactamase (ESBL) genes (blaCTX-M, blaOXA-1, blaSHV, and blaTEM,), carbapenemase genes (blaGIM, blaIMP, blaKPC, blaNDM, blaOXA-48-like, blaSIM, blaSPM, and blaVIM), as well as plasmid-mediated AmpC β-lactamase genes (blaCMY and blaDHA), was performed according to the previously published protocols.8–10 Primers used for this screening are listed in Table 1.
Primers Used for Screening for Antibiotic Resistance Genes
BOX-PCR genotyping of isolates
BOX-PCR genotyping was performed according to Dombek et al. 11 with some minor modifications. Briefly, the isolates, which were phenotypically resistant to at least one β-lactam antibiotic, were cultivated at 30°C for 12 hours using Tryptic Soy agar, resuspended in sterile water, frozen, and maintained at −80°C until use. BOX-PCR was performed in 50 μL of reaction mixture containing DreamTaq Green PCR Master Mix (2 × ) (Thermo Fisher Scientific), 0.5 μM BOXA1R primer (5′-CTA CGG CAA GGC GAC GCT GAC G-3′), and 23 μL of bacterial cell suspension. BOX-PCR conditions were as described by Versalovic et al. 12 Products of amplification were analyzed by electrophoresis through 1% agarose gel.
Data analysis
Electrophoretic profiles of Acinetobacter sp. and P. aeruginosa were analyzed manually and interpreted according to the following guidelines published previously 13 : bacterial isolates that are indistinguishable by typing methods should be considered to represent a single strain, while bacterial isolates that can be distinguished from one another by typing methods should be considered to represent the different strains. Electrophoretic profiles of E. coli and K. pneumoniae were analyzed using the TREECON software v.1.3b. 14 BOX-PCR products of E. coli and K. pneumoniae were scored in a size range from 250 to 2,000 bp. The presence or absence of an individual DNA fragment in the BOX-PCR products was scored as “1” or “0,” respectively. Very weak, unclear, and nonreproducible bands were excluded from scoring. Based on this, the matrix of binary data was constructed. The genetic distance between isolates was calculated according to the method of Nei and Li. 15 The relationship between the samples based on genetic distances was assessed by the unweighted-pair group method with arithmetic means grouping method. The bootstrap analysis was conducted using 1,000 resamplings.
Results
Characterization of β-lactam susceptibility and genotyping of P. aeruginosa
Carbapenem-resistant clinical isolates of P. aeruginosa were screened for β-lactam antibiotic resistance genes. It was determined that only one isolate (5M) was positive for carbapenemase gene blaVIM (Fig. 1). Metallo-β-lactamase gene blaVIM commonly occurs in P. aeruginosa.16,17 Other genes coding for other β-lactamases were not detected in P. aeruginosa clinical isolates.
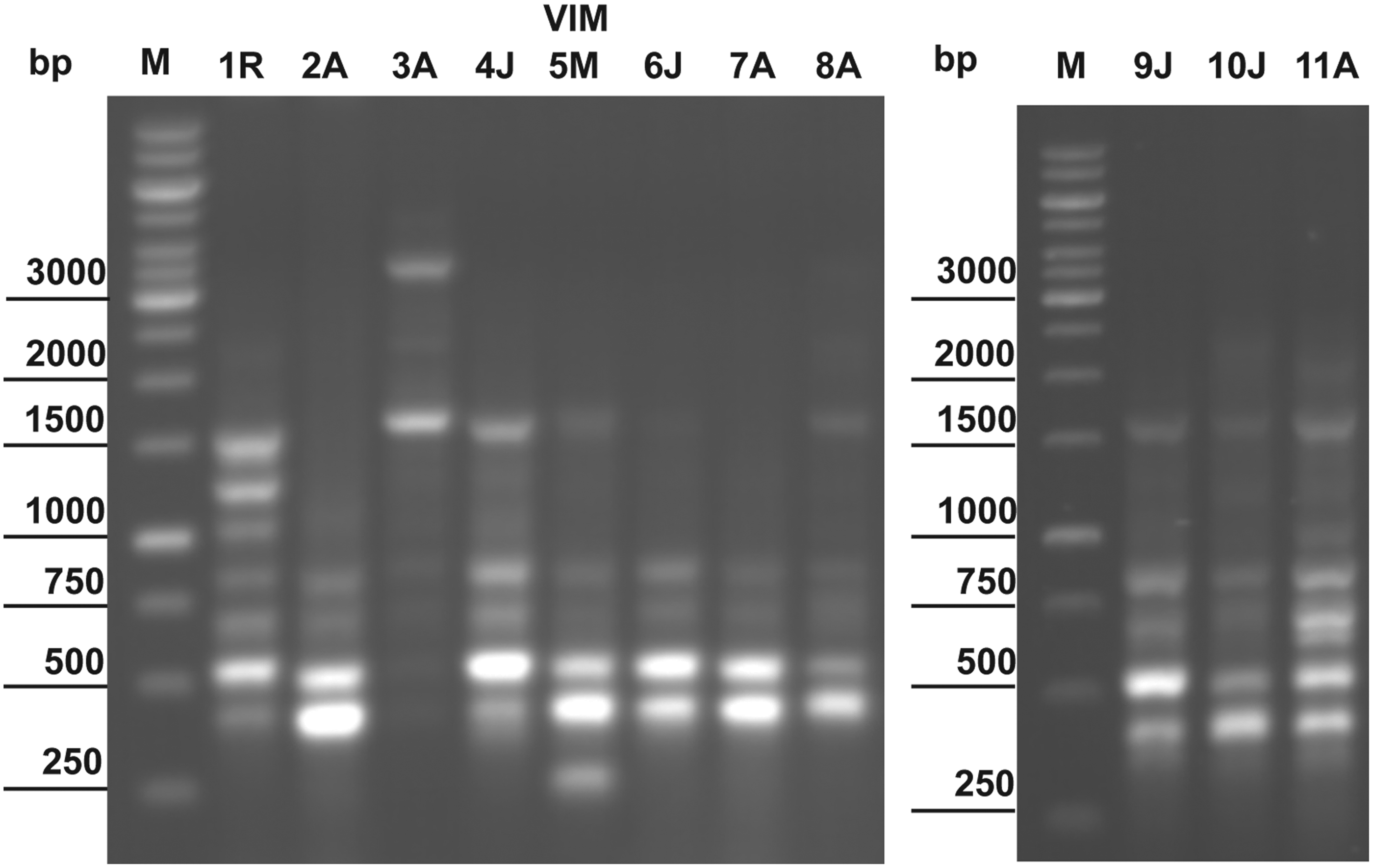
BOX-PCR genotyping of clinical Pseudomonas aeruginosa isolates. VIM—the isolate that was positive for carbapenemase gene blaVIM; A, J, M, and R—different clinical microbiological laboratories of Lithuania. M—Thermo Scientific GeneRuler 1 kb DNA Ladder.
BOX-PCR genotyping allowed to identify a single P. aeruginosa strain that was represented by two isolates: the isolates 6J and 7A came from the different clinical microbiological laboratories, but were identical in the genotyping experiments (Table 2 and Fig. 1). As the different microbiological laboratories provide services to the different healthcare institutions, interhospital transfer of this strain (two isolates) was supposed. Although in some cases with only minor differences, BOX-PCR profiles of the remaining isolates could be distinguished from each other. It was concluded that each of the latter isolates represents a separate nontransmissible strain.
Clinical Bacterial Isolates That Were Supposed to Be Involved in the Inter- and Intrahospital Spread
Isolates that were supposed to represent a single strain are shown in parentheses.
Characterization of β-lactam susceptibility and genotyping of Acinetobacter sp.
It was determined that all 20 tested isolates of Acinetobacter sp. had at least one gene conferring resistance to β-lactam antibiotics. Seven isolates were positive for metallo-β-lactamase blaNDM and carbapenemase blaOXA-48-like genes (Fig. 2). One isolate—the isolate 5F—had carbapenemase gene blaVIM.
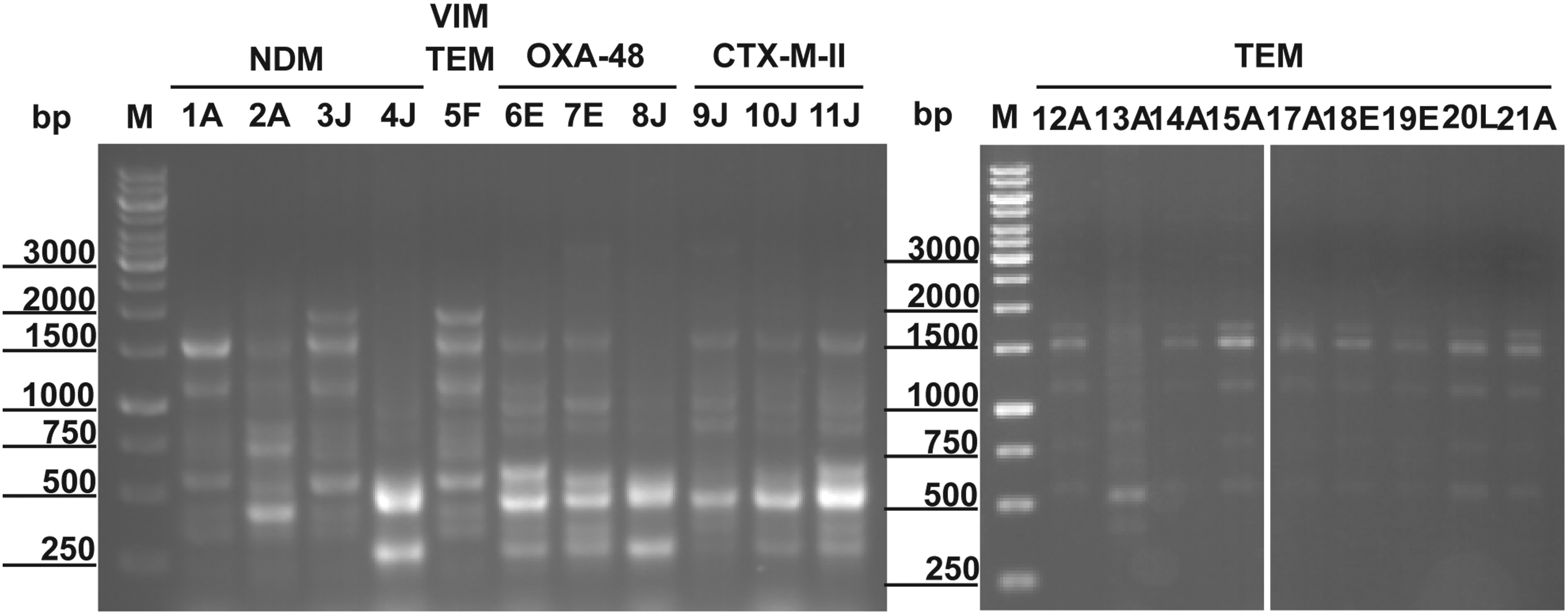
BOX-PCR genotyping of clinical Acinetobacter sp. isolates. CTX-M-II and TEM—isolates that were positive for ESBL genes blaCTX-M-II and blaTEM, respectively; NDM, OXA-48, and VIM—isolates that were positive for carbapenemase genes blaNDM, blaOXA-48-like, and blaVIM, respectively. A, E, F, J, and L—different clinical microbiological laboratories of Lithuania. M—Thermo Scientific GeneRuler 1 kb DNA Ladder. ESBL, extended spectrum β-lactamase.
BOX-PCR genotyping of Acinetobacter sp. isolates revealed more complicated picture of the probable inter- and intrahospital spread compared with P. aeruginosa. Five electrophoretic profiles, each represented by a few genotypically identical isolates from both the same, as well as the different clinical microbiological laboratories, were identified (Fig. 2 and Table 2). Three electrophoretic patterns were represented by the pairs of isolates from the different laboratories/hospitals—3J and 5F, 6E and 11J, as well as 17A and 19E. These isolates were supposed to be involved in the interhospital transfer. The fourth profile was represented by the isolates from the different patients from the same laboratory—4J and 8J. It was already mentioned that the clinical microbiological laboratory J provides services to only a single hospital; therefore, intrahospital transfer of this strain (two isolates) was supposed. And the fifth pattern was represented by six isolates from both the same, as well as the different clinical microbiological laboratories of Lithuania (Table 2). Although the isolates with the latter electrophoretic pattern are clearly involved in the interhospital transfer, the putative intrahospital transfer of the isolates 12A, 14A, 15A, and 21A should be examined more closely in the future because the clinical laboratory A provides services to a few different hospitals. Consequently, these isolates could come to this laboratory from the different healthcare institutions, and, in this case, they could be involved in the interhospital but not intrahospital transfer. The remaining six isolates had unique electrophoretic BOX-PCR profiles representing six nontransmissible strains. It should be noted that isolates from the pairs 3J-5F, 6E-11J, and 4J-8J differed in their bla genes (Fig. 2).
Characterization of β-lactam susceptibility and genotyping of E. coli
In total, 109 E. coli isolates from Lithuanian hospitals were examined in this study. Low phenotypical susceptibility to β-lactam antibiotics was recorded for these isolates, and this information was in accordance with the results for screening for the genes conferring resistance to these antibiotics—almost all (106/109) isolates had 1–7 genes coding for ESBL (94.5% of all tested isolates) and/or AmpC β-lactamase (59.6% of all tested isolates) genes (Table 3). The most frequent resistance gene in E. coli clinical isolates was found to be blaCTX-M-I (67.9% of all isolates) followed by blaCTX-M-II (62.4% of all isolates), blaCMY-II (59.3% of all isolates), blaOXA-1 (46.8% of all isolates), blaTEM (33.9% of all isolates), blaSHV (29.4% of all isolates), and blaCTX-M-IV (15.6% of all isolates) genes. β-Lactamase gene blaDHA was identified in a single isolate. The most frequent combination of the resistance genes was blaCTX-M-I blaCTX-M-II blaOXA-1 blaCMY-II (22.0% of all tested isolates) followed by blaCTX-M-I blaCTX-M-II blaOXA-1 (12.8% of all tested isolates) (Table 3).
Number of Escherichia coli and Klebsiella pneumoniae Isolates with the Different Combinations of the Resistance Genes
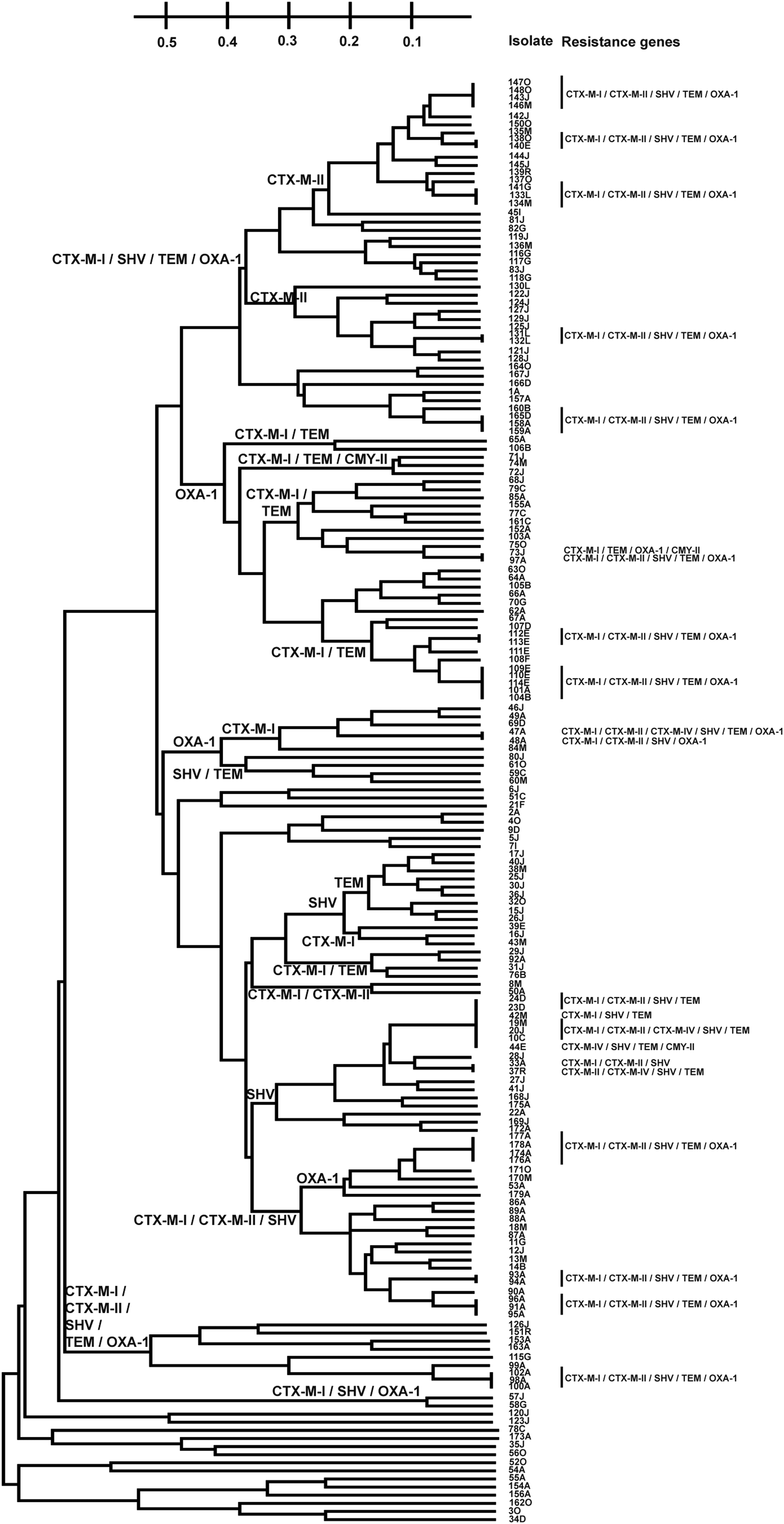
BOX-PCR genotyping revealed 11 clusters of 2-11 isolates with the identical electrophoretic profiles, which were supposed to represent 11 different strains (Fig. 3). Seven clusters/strains included E. coli isolates from the different clinical microbiological laboratories/hospitals (Table 2); consequently, these strains were supposed to be involved in the interhospital transmissions. The isolates from the other four clusters/strains were identified in the samples from the different patients from both the same, as well as the different microbiological laboratories (Table 2). Although interhospital transfer of the latter strains could be supposed, both inter- and intrahospital transmissions could be confirmed only for the cluster/strain represented by the isolates 39D, 37J, 38J, and 42M. For the other three clusters, the isolates from the different hospitals could come to a single clinical microbiological laboratory, and therefore, these strains could be involved in the inter- but not intrahospital transmissions.

UPGMA dendrogram showing the relatedness of Escherichia coli clinical isolates as determined by BOX-PCR genotyping. The resistance genes are shown in detail only for those isolates that were supposed to be involved in the inter- and intrahospital spread. CTX-M-I, CTX-M-II, CTX-M-IV, SHV, TEM, OXA-1, and CMY-II at the nodes of the dendrogram indicate the clusters of the isolates that were all positive for ESBL genes blaCTX-M-I, blaCTX-M-II, blaCTX-M-IV, blaSHV, blaTEM, blaOXA-1, and AmpC β-lactamase gene blaCMY-II, respectively. The scale represents the distance between the isolates. UPGMA, unweighted-pair group method with arithmetic means.
The isolates in some BOX-PCR clusters/strains were identical not only in their electrophoretic patterns but also in terms of their β-lactam resistance genes, while the others differed. Most isolates in the clusters/strains had 2-5 resistance genes, the only exceptions being the isolates 26A, 43O, and 105J with a single resistance gene. The most frequent resistance gene in the clusters/strains was blaCTX-M-I (10/11 clusters) followed by blaCMY-II (9/11 clusters), blaCTX-M-II (8/11 clusters), blaOXA-1 (7/11 clusters), blaTEM (6/11 clusters), blaSHV (5/11 clusters), and blaCTX-M-IV (4/11 clusters) (Fig. 3).
BOX-PCR profiles of 61 clinical isolates (56.0% of all tested isolates) of E. coli were unique and did not fall into the clusters with the probable inter- and intrahospital spread.
Characterization of β-lactam susceptibility and genotyping of K. pneumoniae
In total, 179 clinical isolates of K. pneumoniae were tested in the present study. From one to six ESBL genes were identified in 96.6% of all tested isolates. The most frequent gene in these isolates was found to be blaCTX-M-I (91.1% of all tested isolates) followed by blaTEM (86.6% of all tested isolates), blaSHV (85.5% of all tested isolates), blaCTX-M-II (78.2% of all tested isolates), blaOXA-1 (75.4% of all tested isolates), and blaCTX-M-IV (10.1% of all tested isolates) genes. AmpC β-lactamase gene blaCMY-II was found in 13.9% of all tested isolates, while the genes of carbapenemases were rare in the tested K. pneumoniae—blaKPC and blaNDM genes were identified in only one and two strains, respectively. It should be noted here that the presence of AmpC β-lactamase with ESBL enzymes allows to destroy the carbapenems without any activity of carbapenemases making Gram-negative bacteria resistant to these antibiotics. 17 The most frequent combination of the resistance genes in K. pneumoniae was blaCTX-M-I blaCTX-M-II blaSHV blaTEM blaOXA-1 (53.1% of all tested isolates) followed by blaCTX-M-I blaTEM blaOXA-1 blaCMY-II (8.4% of all tested isolates), blaCTX-M-I blaCTX-M-II blaSHV blaTEM (6.1% of all tested isolates), and blaCTX-M-I blaCTX-M-II blaCTX-M-IV blaSHV blaTEM (6.1% of all tested isolates) (Table 3).
Results of BOX-PCR genotyping showed 15 clusters of 2-7 isolates with the identical electrophoretic profiles representing 15 different strains of K. pneumoniae (Fig. 4). Most clusters/strains (7/15) were represented by the isolates from the different patients from the same microbiological laboratory, but the intrahospital transfer can be clearly stated only for the isolates 131L and 132L—the clinical laboratory L provides services to only a single hospital as was mentioned earlier. Four clusters/strains included the isolates from the different clinical microbiological laboratories that were clearly involved in the interhospital spread (Table 2). The remaining four clusters were composed of the isolates from both the same and the different clinical microbiological laboratories—these strains were supposed to be involved in the interhospital and, probably, in the intrahospital transmissions (Table 2). The profiles of antimicrobial resistance in the clusters/strains were quite uniform—the isolates with the different genes were detected only in 4 out of 15 clusters/strains. All isolates in the remaining 11 clusters/strains had the same combination of the resistance genes—blaCTX-M-I blaCTX-M-II blaSHV blaTEM blaOXA-1 (Fig. 4).
UPGMA dendrogram showing the relatedness of Klebsiella pneumoniae clinical isolates as determined by BOX-PCR genotyping. The resistance genes are shown in detail for those isolates that were supposed to be involved in the inter- and intrahospital spread. CTX-M-I, CTX-M-II, SHV, TEM, OXA-1, and CMY-II at the nodes of the dendrogram indicate the clusters of the isolates that were all positive for ESBL genes blaCTX-M-I, blaCTX-M-II, blaSHV, blaTEM, blaOXA-1, and AmpC β-lactamase gene blaCMY-II, respectively. The scale represents the distance between the isolates.
It should be noted that out of 179 tested clinical isolates of K. pneumoniae, only 46 isolates (25.7% of all tested isolates) fell into the clusters; the remaining electrophoretic profiles were unique and were supposed to represent different nontransmissible strains.
Discussion
Genotyping (pulsed field gel electrophoresis, rep-PCR) of the clinical isolates and identification of the identical genotyping profiles have been shown to be a very effective strategy to determine inter- and intrahospital spread of these isolates.10,18–20 Although some other more discriminative techniques are available (whole-genome sequencing, for example), rep-PCR [BOX-, ERIC-, (GTG)5-, REP-PCR] methods are commonly used because of their simplicity, speed, efficiency, reproducibility, low cost, and feasibility to process large numbers of isolates. BOX-PCR has been previously shown to be highly discriminative for molecular typing of Acinetobacter sp., 21 E. coli,6,11 K. pneumoniae, 20 and P. aeruginosa. 19 Therefore, namely BOX-PCR has been chosen for the genotyping of Gram-negative clinical isolates from the Lithuanian clinical microbiological laboratories. The main purpose of this study was the evaluation of the inter- and intrahospital spread of these Gram-negative pathogenic bacteria in Lithuania. Because of the risk caused by the transmission of antibiotic-resistant bacteria, only the drug-resistant isolates were examined.
The isolates with the identical BOX-PCR electrophoretic profiles were identified for all tested Gram-negative pathogens suggesting that all four pathogens are involved in the intra- and/or interhospital dissemination between the Lithuanian healthcare institutions. But the level of such transmissions varied from species to species. The absolute leader was Acinetobacter sp.—even 70.0% of all tested isolates of these pathogenic bacteria were supposed to be involved in the inter- and intrahospital spread. Bacteria of the genus Acinetobacter are the major cause of the nosocomial infections worldwide, and the spread of these bacteria was reported to occur not only on the national but also on the international scale.22,23 Therefore, the results on the dissemination of these bacteria in and between Lithuanian healthcare institutions were in accordance with the data for other countries—France, Portugal, England, United States, etc. 22 Our results showed that both intra- (at least in the case of the isolates 4J and 8J) and interhospital transmissions contribute to the spread of Acinetobacter sp. in Lithuanian healthcare institutions, and this is a matter of great concern, the rather that all tested isolates of Acinetobacter sp. were phenotypically resistant to carbapenems and had at least one gene conferring resistance to β-lactams. Very high percentage of the supposed transmissions shows that the immediate actions are needed to stop and prevent the spread of these dangerous bacteria in Lithuanian hospitals.
In contrast to Acinetobacter sp., only 18.2% and 25.7% of the tested P. aeruginosa and K. pneumoniae isolates, respectively, could be involved in the inter- and/or intrahospital transmissions. P. aeruginosa can cause both community-acquired and nosocomial infections. 16 Horizontal acquisition of the resistance genes results in the development of the multidrug-resistant strains of this species that are not susceptible to the different antibiotics, including carbapenems. The problem is that mechanisms and ways of the spread of this important pathogen are still unknown. 24 The differences between BOX-PCR profiles of the isolates from the Lithuanian hospitals showed that most of the isolates were either community acquired or the nosocomial strains were not transmitted in and between the healthcare institutions—the interhospital transmission was documented only for two P. aeruginosa isolates.
Inter- and intrahospital spread of drug-resistant K. pneumoniae, as well as the outbreaks caused by such transmissions, was described worldwide.10,20,25,26 Our results show that both intra- and interhospital spread of K. pneumoniae occurs in Lithuanian hospitals. The most important feature of the transmissible K. pneumoniae strains was the resistance profile—even 11 out of 15 transmissible strains had a combination of 5 different ESBL genes—blaCTX-M-I blaCTX-M-II blaSHV blaTEM blaOXA-1. This is in contrast with a single if any resistance gene in the transmitted strains of Acinetobacter sp. and P. aeruginosa. So despite a quite low percentage of the dissemination in and between Lithuanian hospitals, further surveillance of the spread of K. pneumoniae is a matter of great concern because of the high-risk dissemination of the multiple-resistance determinants.
During the last 20 years, a sharp increase in the prevalence of ESBL producing bacteria was determined, and E. coli but not K. pneumoniae became the prevalent carrier. 27 However, the data for the inter- and intrahospital transmissions of the drug-resistant E. coli differ from study to study and from country to country.18,27 In our study, the healthcare associated transmissions were determined to occur in Lithuanian hospitals, and the level of this spread (44.0% of all tested isolates) was determined to be higher for E. coli than for K. pneumoniae. Resistance gene profiles of the transmissible strains were more variable for E. coli than those for K. pneumoniae and included not only ESBL but also AmpC β-lactamase genes. Our results showed that more effective strategy and surveillance are needed to confine and prevent the healthcare associated transmissions of the drug-resistant E. coli strains.
It should be reminded that analysis of the probable inter- and intrahospital transmissions in Lithuanian hospitals was performed using only blood samples; other specimens (urine, tracheobronchial aspirates, wound swabs, etc.) were not examined. It means that the real scale of the healthcare associated transmissions of Gram-negative pathogens can be even larger. In contrast, the possibility that some strains probably involved in the inter- and/or intrahospital spread are, in fact, community-acquired and community-circulating strains, cannot be completely ruled out. In this case, the percentage of the transmissible strains could be slightly overestimated. To minimize this possibility, blood samples have been chosen for analysis.
Our experiments also show that some isolates with the identical BOX-PCR profiles carried different resistance genes, and these results are of great concern. Similar results were also reported by the other authors. For example, Koczura et al. 21 also found some isolates of Acinetobacter calcoaceticus-baumannii complex with the identical BOX-PCR patterns but with the different resistance profiles. Such discrepancies between the results of genotyping and screening for the resistance genes can be explained by localization of some antimicrobial resistance determinants on the different mobile elements. 21 For example, blaCMY, blaCTX-M, blaNDM, blaOXA, blaSHV, and blaTEM genes have been located on plasmids; blaCTX-M and blaTEM genes can also be transferred by bacteriophages.23,28,29 Although there have been no studies showing the horizontal transfer of VIM determinants in A. baumannii, blaVIM-carrying plasmids were described in E. coli, K. pneumoniae, and some other representatives of Enterobacteriaceae.23,28 These plasmids can readily disseminate between the isolates and persist, for example, in human microbiome 30 without any effect on the strain-specific BOX-PCR profile.
In conclusion, our study showed both inter- and intrahospital spread of the drug-resistant Gram-negative bacteria in Lithuanian hospitals. The level of transmissions differed between pathogens, and the worst situation was detected for Acinetobacter sp. followed by E. coli. In almost all cases, transmissible strains had at least one gene conferring β-lactam resistance, thereby contributing to the dissemination of the resistance determinants in and between Lithuanian hospitals.
Footnotes
Disclosure Statement
No competing financial interests exist.