
Abstract
New Delhi metallo-β-lactamase (NDM)-producing bacteria have been identified at a worrying rate in Brazil since 2013. Owing to the need to understand the extent of their spread, this study reports the dissemination of blaNDM in different species of Gram-negative bacilli in different regions and states of Brazil. A total of 81 isolates from nine states were studied, including 11 species. All isolates carried blaNDM-1 variant and were considered multidrug resistant. Colistin and amikacin were the agents with higher activity compared with the other drugs tested. The findings indicate that the NDM-1 enzyme is already widespread in the country.
Introduction
New Delhi metallo-β-lactamase (NDM)-producing bacteria are resistant to all β-lactams, except aztreonam and may harbor mechanisms of resistance to other antimicrobials. 1 NDM was first detected in 2008 in a Klebsiella pneumoniae isolated from a Swedish patient formerly hospitalized in India. 2 Since then, NDM-producing Enterobacteriaceae, Acinetobacter sp., and Pseudomonas aeruginosa have been detected in several countries. 1 Until now, 24 variants of this enzyme have been identified with variable carbapenemase activity. 3
In Brazil, NDM-1 was first identified in a Providencia rettgeri isolated in a hospital from Rio Grande do Sul in 2013. 4 A retrospective study in the same hospital revealed that NDM has been present in the country since 2012. 5 Since then, NDM has been reported sporadically in different states of Brazil such as Rio de Janeiro,6–8 Paraná, 9 Rio Grande do Sul,10–12 Santa Catarina, 13 Distrito Federal, 14 São Paulo,15,16 and Bahia, 17 and in several bacterial species, including Enterobacter cloacae, Enterobacter hormaechei, P. rettgeri, Escherichia coli, K. pneumoniae, Acinetobacter pitti, Klebsiella oxytoca, Citrobacter freundii, Acinetobacter bereziniae, Proteus mirabilis, and Acinetobacter baumannii. 18
Owing to the increasing reports of NDM-producing bacteria in Brazil18,19 and the need to understand the extent of their dissemination, this study reports the distribution of NDM in several bacterial species in different states of Brazil.
Materials and Methods
Bacterial isolates and identification
The Laboratório de Pesquisa em Infecção Hospitalar–LAPIH (Oswaldo Cruz Institute, Rio de Janeiro) frequently receives clinical bacterial isolates from Brazilian Central Laboratories of Public Health and hospitals to evaluate the determinants of drug resistance by PCR. A total of 81 NDM-producing Enterobacteriaceae and Acinetobacter sp. isolates received from nine states of Brazil (Rio de Janeiro, Espírito Santo, Santa Catarina, Rio Grande do Sul, Paraná, Bahia, Sergipe, Maranhão, and Goiás) were included in this study.
The isolates were collected between October 2012 and October 2015 from different clinical specimens. The species identification was previously made by each health care facility and then confirmed by standard biochemical methods in LAPIH. A. bereziniae was identified by rpoB sequencing 13 and A. baumannii identified by rpoB sequencing and PCR for blaOXA-51 gene 9 since phenotypic methods are inefficient to discern species of Acinetobacter. 20
PCR amplification genes and sequence analysis
The blaNDM gene was detected by PCR with the thermal cycles: 94°C for 5 min; 30 cycles of 94°C for 45 s, 58°C for 30 s, and 72°C for 30 s; 72°C for 5 min. Primers used were NDM-Seq-F (5′-CGAAGCTGAGCACCGCATTA-3′) and NDM-Seq-R (5′-TCAGCGCAGCTTGTCGGC- 3′) (this study), which amplified the whole blaNDM gene. Primers were analyzed with several parameters such as self-dimer, hairpin, and CG% using Geneious 8.0 (Biomatters Ltd., New Zealand). BLAST analysis also revealed neither interaction between primer pairs nor unspecific binding to other genes. E. coli (American Type Culture Collection) ATCC 25922 and a whole-genome shotgun sequencing isolate of a clinical NDM-positive K. pneumoniae (CCBH13327) 7 were used as the negative and positive control, respectively. The amplicon was purified with Wizard SV Gel and PCR Clean-Up System (Promega), quantified with Qubit® (Thermo Fischer Scientific™) and sequenced with DNA 3730xl Analyzer (Applied Biosystems, EUA). DNA sequence identity was confirmed using Nucleotide Basic Local Alignment Search Tool (BLASTn) against nucleotide sequence database. Nucleotide sequences were also aligned with 24 blaNDM variants using Geneious 8.0 (Biomatters Ltd.). The genetic environment of the blaNDM gene was assessed by PCR mapping, as described elsewhere. 21 The mcr-1 and blaCTX-M extended-spectrum β-lactamase (ESBL) genes were detected as previously described.22,23
Antimicrobial susceptibility test and carbapenemase production
The susceptibility of the isolates to ertapenem, meropenem, doripenem, piperacillin-tazobactam, cefepime, cefotaxime, cefoxitin, ciprofloxacin, aztreonam, gentamicin, amikacin, minocycline, and sulfamethoxazole/trimethoprim were evaluated with agar diffusion method following Clinical and Laboratory Standards Institute (CLSI) guidelines. 24 Cefoxitin was not tested for E. cloacae and C. freundii isolates, and the same occurred with aztreonam and ertapenem for A. baumannii isolates, since these species have intrinsic resistance to those antibiotics. 24 Carbapenemase production was detected using Blue Carba test 25 and carbapenem inactivation method (CIM). 26
Broth microdilution antimicrobial susceptibility testing
Of the 81 isolates, 75 were analyzed for broth micro-dilution antimicrobial (BMD) susceptibility testing. Isolates of intrinsically colistin-resistant species (n = 6) (Morganella morganii, P. mirabilis, Providencia stuartii, and P. rettgeri) were not evaluated. Sulfate salt of colistin (Sigma, St. Louis, MO) was dissolved in cation-adjusted Mueller Hinton Broth (Oxoid, Basingstoke, England) and BMD performed in accordance with CLSI/EUCAST reference method. 27 Dilutions to the minimum inhibitory concentration (MIC) range of 0.125–256 mg/L were performed in untreated 96-well polystyrene microplates. E. coli ATCC 25922 was used as the drug-susceptible control strain, whereas intrinsically P. mirabilis ATCC 12453 served as the colistin-resistant control strain. EUCAST breakpoints were used for interpretation of colistin MIC results (susceptible ≤2 mg/L and resistant >2 mg/L).
Results
From 81 isolates, 1.2% (n = 1) was collected in 2012, 3.7% (n = 3) were collected in 2013, followed by 33.4% (n = 27) in 2014, and 61.7% (n = 50) in 2015. The isolates were collected from rectal swab (n = 35), urine (n = 19), blood (n = 14), catheter tip (n = 4), cerebrospinal fluid (n = 2), surgical wound (n = 2), tracheal secretion (n = 2), ascitic fluid (n = 1), nasal swab (n = 1), and other secretion (n = 1) (Table 1). Of these bacteria 43.2% were isolated from rectal swab, followed by 23.4% isolates recovered from urine samples.
Origin, Specimen of Isolation and Resistance Profile of the Bacterial Isolates Evaluated in This Study
BA, Bahia; ES, Espírito Santo; GO, Goiás; MA, Maranhão; PR, Paraná; RJ, Rio de Janeiro; RS, Rio Grande do Sul; SC, Santa Catarina; SE, Sergipe.
AMK, amikacin; ATM, aztreonam; CIP, ciprofloxacin; COL, colistin; CTX, cefotaxime; DOR, doripenem; ETP, ertapenem; FEP, cefepime; FOX, cefoxitin; GEN, gentamicin; MEM, meropenem; MH, minocycline; SXT, sulfamethoxazole/trimethoprim; TZP, piperacillin/tazobactam.
Resistance was detected by broth microdilution antimicrobial susceptibility testing. Resistant isolates with range from 4 to 32 mg/L.
Others include catheter tip, cerebrospinal fluid, surgical wound, tracheal secretion, ascitic fluid, nasal swab, and other secretion samples.
NA, not applicable.
The isolates were identified as K. pneumoniae (n = 39), E. cloacae (n = 17), K. oxytoca (n = 9), E. coli (n = 5), C. freundii (n = 3), P. stuartii (n = 2), P. rettgeri (n = 2), P. mirabilis (n = 1), M. morganii (n = 1), A. bereziniae (n = 1), and A. baumannii (n = 1). The isolates were collected from nine states representing four macroregions in Brazil as shown in Fig. 1.
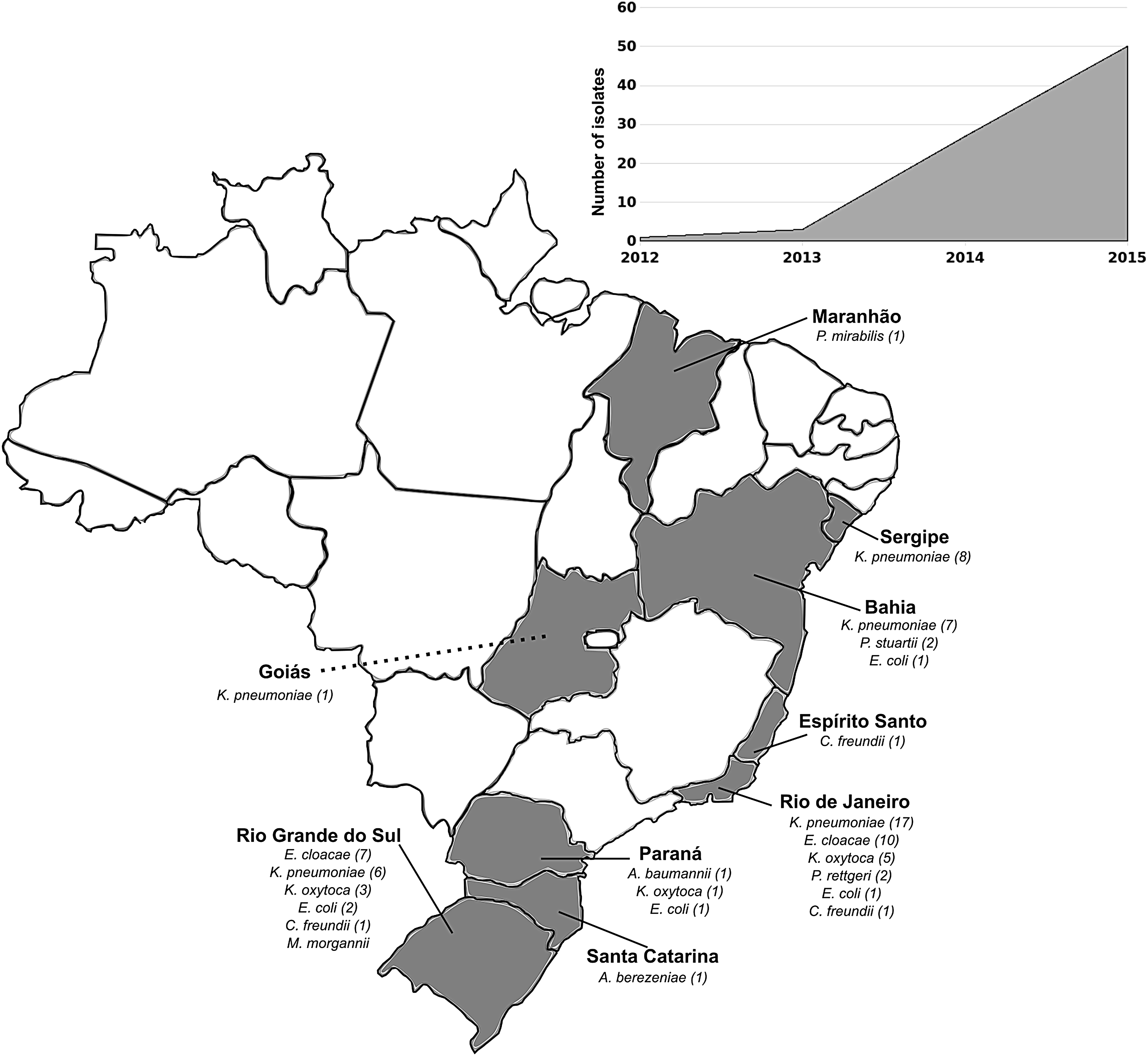
Distribution of NDM-producing bacterial species in different states of Brazil. NDM, New Delhi metallo-β-lactamase.
Both primers showed a high sensibility and specificity. No false or negative amplification was found. A specific 795 bp amplicon was observed in all isolates. Nucleotide sequence analysis showed that all isolates harbored the blaNDM-1 gene variant and carried the conserved structure associated with a truncated insertion sequence ISAba125 upstream the blaNDM and a bleomycin resistance gene (bleMBL) downstream, except for one K. pneumoniae from Rio de Janeiro that holds the whole ISAba125 element. All isolates were identified as carbapenemase producers by Blue Carba test, whereas 98.8% showed carbapenemase activity in CIM. All 81 isolates were found to be PCR-negative for mcr-1 gene. In addition, all isolates were EBSL-encoding gene blaCTX-M positive.
Overall, isolates were highly nonsusceptible to tested drugs.Of the isolates 71.6% (n = 58) were nonsusceptible to any of the β-lactams tested (98.7% cefotaxime; 97.5% ertapenem, meropenem, and doripenem; piperacillin/tazobactam; 96.7% cefoxitin; 95.1% cefepime; and 75% aztreonam). Of the isolates 42% (n = 34) were nonsusceptible to both aminoglycosides tested (77.8% gentamicin and 42% amikacin). Of the isolates 86.4% were nonsusceptible to trimethoprim/sulfamethoxazole, 85.2% to ciprofloxacin, and only 50.6% to minocycline (Table 1). Colistin reference MICs for the 75 Gram-negative bacteria showed a range of 0.25–32 mg/L. Overall, 24% (n = 18) isolates were resistant to colistin (ranging from 4 to 32 mg/L), being K. pneumoniae (n = 12) the most frequent bacterium, followed by E. cloacae (n = 3), K. oxytoca (n = 2) and A. bereziniae (n = 1). From 81 isolates, 3.7% (n = 3; one K. pneumoniae and two E. cloacae) showed no antibiotic treatment options among all drugs available in this study.
Discussion
All isolates carried the blaNDM-1 gene variant, which is highlighted due to its higher incidence and spread in cases of clinical infection.1,28 The absence of a previous detection of other variants in Brazil9–13 and the findings of this study suggest the predominance of the blaNDM-1 variant in the country, similar to other countries of Latin America. 19
Campos et al. suggested that the transposon Tn3000, which carries a conserved structure associated with a whole or a truncated ISAba125 upstream blaNDM and downstream bleMBL, plays an important role in blaNDM spread, since they have been detected in distinct plasmids from different countries, including Brazil. 6 In this study, the truncated ISAba125 element was found in most isolates. This genetic structure was also previously described in NDM-producing E. coli and E. hormaechei from Rio de Janeiro. 6 Only one K. pneumoniae isolate holds the whole ISAba125 element, similar to a K. pneumoniae strain isolated in India. 21
K. pneumoniae was the most frequent bacterial species in this study and has been reported as one of the most frequent NDM producers. 1 It was demonstrated that the spread of NDM-producing K. pneumoniae seems to be not associated with clonal expansion in Brazil, 29 differently from the greatly worldwide spread of K. pneumoniae KPC-carbapenemase-producing K. pneumoniae. 30
Regarding the carbapenemase production, CIM was not able to detect only one NDM-producing E. cloacae; despite this, both Blue Carba test and CIM exhibited high sensitivity and specificity, as reported,31,32 suggesting that both tests can be useful and important tools for NDM detection.
In this study, we found isolates belonging to 11 species producing NDM and all of them were considered multidrug resistant (MDR), according to Magiorakos et al. criteria. 33 Most studies report that the dissemination of NDM is associated with different bacterial species with diverse resistance patterns and plasmids, which facilitates the occurrence of MDR clones and decreases therapeutic options.1,19,34
All isolates were EBSL-encoding gene blaCTX-M positive. The coexistence of blaCTX-M and blaNDM has already been reported. 35 EBSL-producing bacteria have spread worldwide as causative agents of infection in humans, including in Brazil. 18 Furthermore, 24% of our isolates were colistin resistant. This finding raises a major concern since colistin/polymyxin have been the last-line antibiotics used to treat MDR Gram-negative bacteria and its efficacy is being compromised by the higher detection of the mobile colistin resistance gene, mcr-1. 36 Despite human infections caused by mcr-1-producing bacteria have already been reported in Brazil,37,38 all isolates in this study were mcr-1 negative.
This study shows the presence of NDM producers in health care facilities, which is a growingly important medical issue that compromises the efficacy of treatment. Furthermore, reports of NDM in recreational waters 39 and soil 40 are factors that corroborate to this spread.
Our data show that from 2012 to 2015 there was a significant increase of NDM-producing Gram-negative bacteria. The alarming presence of NDM-1 in several states of Brazil indicates that this enzyme is already widespread in the country. Only isolates received by our laboratory were used in this study, so the prevalence of NDM in Brazil can be much higher than disclosed. Moreover, all isolates were considered MDR being a fact of great concern. The fact that 44% isolates were recovered from rectal swabs is also worrying and justifies the necessity of surveillance. Furthermore, this study reports for the first time the detection of an NDM-producing P. stuartii in Brazil and the presence of NDM in Goiás, Sergipe, Maranhão, and Espírito Santo.
Footnotes
Acknowledgments
This project was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico, Fundação Carlos Chagas de Amparo a Pesquisa, and Instituto Oswaldo Cruz.
Disclosure Statement
No competing financial interests exist.