
Abstract
Aims:
Although the cases of macrolide-resistant Mycoplasma pneumoniae (MRMP) have been increasing substantially among children, there are very few studies that have focused on MRMP in adults. This study aimed to investigate the prevalence and clinical features of community-acquired pneumonia (CAP) caused by MRMP from adults in Jeju Island, Korea.
Methods:
We retrospectively recruited adult patients with CAP in whom M. pneumoniae infections had been confirmed for a 7-year period. Macrolide resistance was determined by identifying a mutation in the 23S rRNA gene using PCR.
Results:
In total, 70 subjects were included. Their mean age was 46.1 years and 36 (51.4%) were women. Only two isolates (2.9%) carried macrolide resistance mutations in the 23S rRNA gene, and all the mutations were A2063G transitions. No significant differences were observed in age, comorbidities, symptoms, duration of fever, and length of hospital stay between the MRMP and macrolide-sensitive Mycoplasma pneumoniae groups. The number of involved pulmonary lobes was greater in the MRMP group (3.50 vs. 1.44, p = 0.008).
Conclusion:
The prevalence of CAP caused by MRMP was relatively low in adults in Jeju Island. Patients with MRMP pneumonia tended to have multilobar pneumonic infiltrates.
Introduction
M
M. pneumoniae is resistant to antimicrobials targeting the cell wall, including β-lactams. M. pneumoniae is susceptible to macrolides, tetracyclines, and fluoroquinolones, and macrolides are the first-line treatment for M. pneumoniae respiratory infections because of their low minimum inhibitory concentrations against bacteria and their safety and low toxicity. 1 There are several reports that the cases of macrolide-resistant Mycoplasma pneumoniae (MRMP) have been increasing substantially among children, especially in Japan (50–90%) and China (>80%).5,6 Korea is geographically located between these two countries, and few studies have also shown increased prevalence of MRMP in children from Korea.7–10 However, to the best of our knowledge, there have been no studies focusing on MRMP in adult patients with CAP. Instead, few studies investigated MRMP pneumonia in both adolescents and adults.11,12 In Korea, only one study demonstrated the prevalence of MRMP in adult and pediatric patients with CAP during an epidemic in 2011, which was significantly lower in adults than in children. 13
This study aimed to investigate the prevalence and clinical features of CAP caused by MRMP from adults in Jeju, the largest island off the southern coast of Korea. These results may provide useful information to guide the treatment of CAP cause by M. pneumoniae in Korea.
Materials and Methods
Study population and sample processing
We recruited adult patients (≥18 years) with CAP in whom M. pneumoniae infections were confirmed by PCR from their respiratory specimens at Jeju National University Hospital on Jeju Island in Korea between April 2010 and December 2016. A diagnosis of CAP was made based on the following criteria: (1) symptoms of an acute lower respiratory tract illness; (2) new focal chest signs on examination; (3) at least one systemic feature (either a symptom complex of sweating, fevers, shivers, aches, and pains and/or temperature of 38°C or more); (4) no other explanation for the illness, treated as CAP with antibiotics. 14
Respiratory specimens (expectorated sputum from 69 patients and transtracheal aspirate from 1 patient) were collected when the patients were hospitalized or visited the emergency department. We used the DNA for diagnosis on admission and stored it at −80°C for further study. M. pneumoniae infections were confirmed by PCR as follows. DNA extraction from the respiratory specimens was performed using the Chemagen® DNA Extraction Kit (Perkin Elmer, Inc., Baesweiler, Germany) according to the manufacturer's instructions. Extracted DNA was amplified on the Veriti® 96-Well Thermocycler (Applied Biosystems, Waltham, MA) using the PneumoBacter ACE Detection Kit (Seegene, Inc., Seoul, Korea), which can detect six bacterial pathogens, including M. pneumoniae. We selected the samples in which only M. pneumoniae was detected and confirmed the P1 adhesin amplification by PCR.
Demographic information, such as underlying diseases, clinical manifestations, laboratory findings, radiological features, and CURB-65 pneumonia severity scores, was collected retrospectively from medical records. Treatment response and outcomes, such as time to defervescence, days of hospitalization, classes of antimicrobials used, and days of antimicrobial use, were also collected.
Amplification of macrolide resistance genes
The frozen M. pneumoniae DNA was used to examine the presence of macrolide resistance genes. Domain V of the 23S rRNA gene was amplified by PCR using specific primers (forward, 5′-CGCAAGCGAAGCTTTTAACT; reverse, 5′-ATTCCACCTTTCGCATCAAC) (10). PCR was performed in a total volume of 20 μL containing 0.2 μL of genomic DNA and 2 μL of 10 × buffer in a PCR PreMix Tube (Accu-Power; Bioneer Inc., Alameda, CA). The reaction mixture was subjected to denaturation, annealing, and elongation for 5 minutes at 90°C, 30 seconds at 90°C, 40 seconds at 50°C, followed by an extension step of 5 minutes at 90°C for 35 PCR cycles. When the PCR product was uncertain, nested PCR was performed using a second set of primers (forward, 5′-TAACTATAACGGTCCTAAGG; reverse, 5′-ATTCCACCTTTCGCATCAAC). The amplified products were analyzed by electrophoresis on a 1.5% agarose gel. The sizes of the PCR products were 306-bp and 263-bp, including positions 2063 and 2064.
Statistical analyses
All statistical analyses were performed using the statistical software package PASW Statistics v18.0.0 (IBM Co., Armonk, NY). Patient characteristics and treatment outcomes were compared between the MRMP and macrolide-susceptible Mycoplasma pneumoniae (MSMP) patient groups. Categorical variables were compared using the chi-square test or Fisher's exact test, and continuous variables were analyzed using the Mann–Whitney U test. A value of p ≤ 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Jeju National University Hospital Institutional Review Board with an exemption for acquiring informed consent (No. 2017-17). There are no potential conflicts of interest relevant to this article.
Results
Patient characteristics
In total, 70 adult patients with M. pneumoniae pneumonia were included in this study. Their mean age was 46.1 ± 19.2 years (range, 18.5–82.5 years), and 34 patients (48.6%) were men. Forty-one patients (58.6%) were previously healthy, and the others had more than one comorbidity. The prevalence of M. pneumoniae pneumonia in adults was the highest in 2010 and 2011 during the study period, and a slightly increased prevalence was also found in 2016 (Fig. 1).
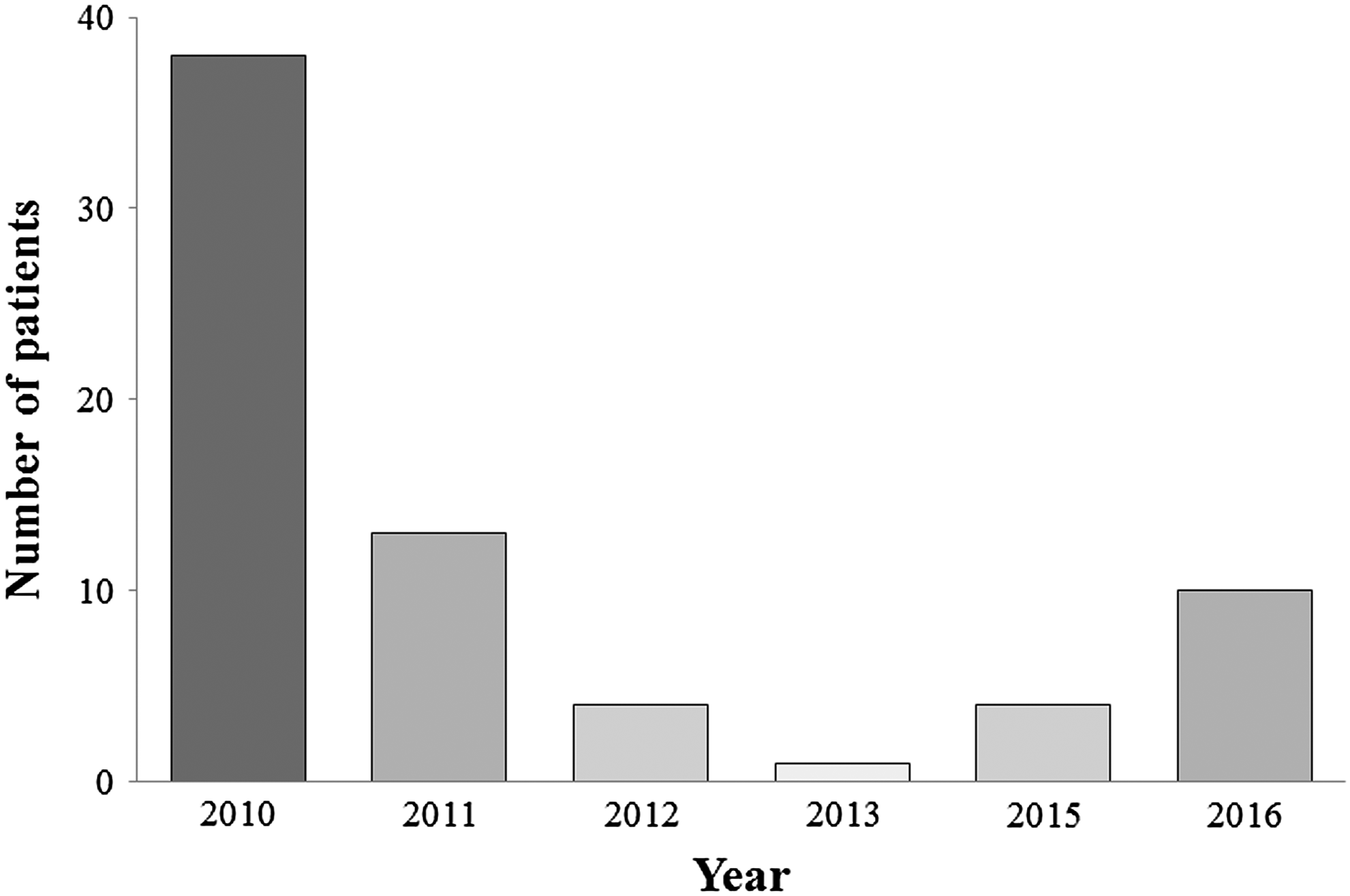
Annual distribution of Mycoplasma pneumoniae pneumonia during the study period.
Prevalence of MRMP
Of the 70 M. pneumoniae-positive respiratory specimens, only 2 (2.9%) had macrolide resistance. All MRMP showed the A2063G point mutation in domain V of the 23S rRNA gene. No other mutation in the 23S rRNA was detected. One case of macrolide resistance was found in 2011, and the other case was in 2016.
Clinical characteristics of MRMP and MSMP patient groups
The demographic data, symptoms, and laboratory findings of adult patients with MRMP and MSMP pneumonia are summarized in Table 1. There were no significant differences in age, gender, and the number of comorbidities between the two groups. Laboratory findings and CURB-65 score also did not show any significant differences between the two groups. However, the number of involved pulmonary lobes was greater in the MRMP group (3.50 vs. 1.44, p = 0.008). Pleural effusion was detected in eight patients (11.4%) of the MSMP group but was not detected in the MRMP group.
Baseline Characteristics of Macrolide-Resistant Mycoplasma pneumoniae and Macrolide-Sensitive Mycoplasma pneumoniae Groups
Values are presented as mean ± SD, or n (%).
ALT, alanine transaminase; AST, aspartate transaminase; CRP, C-reactive protein; MRMP, macrolide-resistant Mycoplasma pneumoniae; MSMP, macrolide-susceptible Mycoplasma pneumoniae; SD, standard deviation; WBC, white blood cells.
Comparison of treatment response in MRMP versus MSMP pneumonia
Antibiotics that were used to treat M. pneumoniae pneumonia and the patient response to the treatment were compared between MRMP and MSMP patient groups (Table 2). There were no significant differences in the duration of fever, days of hospitalization, and days of antimicrobial use between the two groups. All patients with MRMP were treated with the β-lactam plus macrolide combination, and they finally recovered without treatment failure. Three deaths occurred during hospitalization in the MSMP group, which were due to exacerbation of chronic obstructive lung disease, superimposed nosocomial infection, and heart failure.
Values are presented as mean ± SD, or number (%).
FQ, fluoroquinolone.
Discussion
This study aimed to investigate the prevalence and clinical features of CAP caused by MRMP from adults in Jeju Island, Korea. In total, 70 patients with M. pneumoniae pneumonia were identified during the study period, and only 2 of them were found to harbor MRMP. It was also demonstrated that the number of involved lobes was greater in the MRMP group.
M. pneumoniae is known to be the most common causative agent of atypical pneumonia worldwide. The mainstays of therapy are macrolides, doxycycline, or fluoroquinolones, and physicians generally prefer a short-course treatment with azithromycin. However, macrolide resistance has been increasing in frequency among children from various regions, particularly in Asia rather than in Western countries.6,15–18 In addition, there are some evidences that the prevalence of MRMP pneumonia is considerable even in the adult population.11,12,19,20 In a Japanese report, 41% of M. pneumoniae strains showed macrolide resistance in adolescent and adult patients with CAP. 11 Moreover, the resistance rate of M. pneumoniae from adult patients with respiratory infection was as high as 49–80% in China.12,19,20
To the best of our knowledge, this is the first study concerning MRMP in adult patients with CAP in Korea. The rate of macrolide resistance for 6 years was 2.9% in this study. In a previous Korean study, which was conducted during a short epidemic in 2011, the rate of macrolide resistance was 13.3% among adolescent and adult patients with CAP (≥16 years old). 13 In the most recent study from Jeju Island, the prevalence of MRMP was 10.9% among children with lower respiratory tract infection. 21 This was markedly lower than the prevalence among children with CAP in the previous Korean study (61.3%). 13 Therefore, the frequency of macrolide-resistant isolates was lower in Jeju Island than in the Korean peninsula and other surrounding countries, among children as well as adults.
The reason for the relatively low prevalence of MRMP in Jeju Island was difficult to explain. Geographical isolation might be partly responsible for these differences in prevalence. In fact, the increasing pattern of MRMP was common in Asia. However, several recent reports have presented a gradual decrease of resistance rates in Japan.22,23 The high prevalence of MRMP is by no means a universal status in the whole of Asia, and macrolide-resistant rates could be subject to change. Previous administration of macrolides might be closely related to the regional prevalence of MRMP, 15 and so, it would be meaningful to collect data on the regional antibiotic use in Korea in the near future.
In patients with MRMP pneumonia in this study, pulmonary infiltrates were found in three or more lobes on their chest images. Although this finding could be incidental, a similar report suggested that radiological findings were more serious in the MRMP group. 24 There were also some reports that time to resolution of fever and duration of therapy were significantly longer for patients who were infected with macrolide-resistant strains.9,12,13 Therefore, some experts have suggested alternative antibiotics for when patients remain febrile at least 48–72 hours after macrolide treatment in children with MRMP pneumonia. 25 However, no significant differences were found in the duration of fever and days of antimicrobial use between the MSMP and MRMP groups in this study. In addition, the condition of all patients with MRMP improved with the β-lactam plus macrolide combination treatment, and no treatment failure was observed. We cannot explain the precise reason, but these treatment responses might be because M. pneumoniae infections are usually mild and self-limiting. One possible hypothesis was that drug-resistant strains of M. pneumoniae suffer from less efficient protein synthesis and can be eradicated from the respiratory tract before propagating to sufficient amounts to develop pneumonia at many instances in adults. 26
This study has several limitations. First, the number of study subjects was relatively small, and among them only two patients had MRMP pneumonia. Therefore, the number of subjects was not adequate to analyze the difference between the two groups. Second, the clinical data of the patients were collected retrospectively only from medical records. Third, this study is limited to patients who were hospitalized or visited the emergency department, suggesting the inclusion of more severe cases. Therefore, the results cannot be generalized to the outpatients with M. pneumoniae pneumonia.
In conclusion, the prevalence of CAP caused by MRMP was relatively low in adult patients in Jeju Island. Although the sample size was inadequate for statistical analysis, patients with MRMP pneumonia tended to have multilobar pneumonic infiltrates. There were no other clinical characteristics that could differentiate between patients with MRMP pneumonia and those with MSMP pneumonia. Further studies with a higher number of patients are warranted to clarify these results.
Footnotes
Acknowledgment
This work was supported by a research grant from Jeju National University Hospital in 2017.
Disclosure Statement
The authors have no conflicts of interest to declare.