
Abstract
Chryseobacterium indologenes is an emerging nosocomial pathogen that produces IND-type chromosomal metallo-beta-lactamase. The phenotype and molecular aspects of two multidrug resistant C. indologenes strains and the analysis of the tertiary structure of the IND enzyme were studied. Identification of species and susceptibility tests were performed using the Vitek-2 compact. Chromosomal and plasmid DNA were extracted using PureLink™ Genomic DNA Mini Kit and PureLink Quick Plasmid Miniprep Kit, and the sequencing was performed using ABI 3130 genetic analyzer. Two strains were isolated and are registered as P-23 and P-113. Of the two, P-113 was sensitive to ciprofloxacin and cefepime only, whereas the P-23 showed reduced sensitivity to ceftazidime, ciprofloxacin, and tigecycline. The genetic analysis of both isolates identified the presence of the blaIND-like gene, with similarity to IND-3 and IND-8 alleles. The IND-3 identified in the P-133 sample presented a single mutation at position T355G, which corresponds to a nonsynonymous substitution of the amino acid at position 119 (Ser→Ala). The phylogenetic analysis of INDs showed lineages that are circulating in Asian and European countries. These results emphasize the need for effective preventive actions to avoid the dissemination of this type of pathogen in the hospital environment.
Introduction
C
Eight different sublineages of resident enzymes have been identified in the Flavobacteriaceae family, such as BlaB from Elizabethkingia meningoseptica, IND from C. indologenes, JOHN from Flavobacterium johnsoniae, CGB from Chryseobacterium gleum, EBR from Empedobacter brevis, TUS from Myroides odoratus, and MUS from Myroides odoratimimus.3,5 The most common Flavobacterium isolated from clinical specimens is C. indologenes, associated with different types of infections. 3 C. indologenes are commonly encountered on lavatories, faucets in hospitals, and in chlorinated water systems,4–7 creating potential reservoirs for infections. 8 The clinical isolates of C. indologenes have been associated with severe infections in urinary tracts, pneumonia,6,7 sepsis, meningitis, endocarditis, cellulitis, abscess formation, and ocular infections,8–10 with high mortality rates, mainly in immunocompromised patients and newborns.8–10 Genetic variants of IND have been identified in various countries such as South Korea, Japan, Italy, France,1,3,6,7,9–12 Taiwan, Kuwait, 9 Turkey, Greece, 13 United States, and Mexico.9,14 However, these reports are restricted to clinical aspects of nosocomial infections. In Brazil, reports about this pathogen are restricted to cases of nosocomial infections. In this communication, the molecular characteristics of two multidrug resistant C. indologenes that presented a novel mutation, along with its phylogenetic studies, are described.
Materials and Methods
Collection of samples
The blood samples were collected from two female inpatients, aged 64 and 82 years old, respectively, hospitalized in a public health hospital and sent to Hematology and Hemotherapy Foundation (HEMOAM-Manaus-AM), a reference center in the northern region of the country that serves patients with or without hematological diseases.
Cultivation, identification, and antibiotic susceptibility test
The C. indologenes (P-23 and P-113 isolates) were identified during 10,090 bacteriological tests, performed between 2014 and 2015 by the Clinical Bacteriology Laboratory of HEMOAM. The identification, susceptibility test, and minimum inhibitory concentration values were performed by Vitek-2 compact automatic microbial identification system (bioMérieux, Brazil), according to the manufacturer's recommendations and Clinical Laboratory Standard Institute (CLSI) reference manual. 15
Molecular characterization
For genetic characterization of the antimicrobial resistance, the genomic and plasmidial DNA was extracted directly from colonies resuspended in 200 μL of Lysis Buffer from the PureLink™ Genomic DNA Mini Kit and PureLink Quick Plasmid Miniprep Kit (Invitrogen, Carlsbad, CA). The polymerase chain reaction (PCR) for the molecular characterization of the strains of the β-lactamase genes blaOXA, blaSHV, blaCTX-M-1; blaCTX-M-2; blaCTX-M-8; blaCTX-M-9; blaVIM; blaGES; blaIND-like; and blaIND-2 was performed according to the protocols described previously.16–20 For detection of the carbapenemase blaKPC and the metallo-beta-lactamase blaNDM genes, two pairs of primers were designed: blaKPC-FW-5′-ATGTCACTGTATCGCCGTC-3′; blaKPC-RV-5′-TTACTGCC CGTTGACGCC-3′; and (blaNDM-FW-5′-GCCCAATATTATGCACCCGG-3′; blaNDM-RV-5′-CGCAGCTTGTCGGCCAT-3′). The PCR product of the blaIND gene was sequenced using sense and antisense primers and the BigDye Terminator v3.1 Cycle Sequencing Kit (Thermo Fisher Scientific) in the Automatic ABI PRISM 3130xl Genetic Analyzer (Applied Biosystems, Foster City, CA). The Geneious v.11 and MUSCLE (MEGA software) were used for the sequence analysis. The nucleotide sequences obtained were compared with other sequences of Chryseobacterium sp. downloaded from NCBI genome database, using BLASTN alignment tool.
Primary structure and phylogenetics analysis
The in silico analysis of the IND primary structures was achieved using the I-TASSER server (zhanglab.ccmb.med.umich.edu), to infer about the tertiary structure of the enzymes, based on the sequence-structure-function paradigm. 21 The molecular characterization of the strains Bla B1 was obtained from phylogenetic inference using metallo-beta-lactamase B1 (Bla B1) sequences of Chryseobacterium sp., from the GenBank. The phylogenetic tree was made using the Bayesian analysis with the general time reversible model 22 in the software Mr. Bayes 3.2.6 23 and tested through a nonstatistical parametric of the replications Bootstrap method, 24 with a minimum percentage of 50% and 1,000 replications. The established parameters were as follows: 1—mutation rates equal to 0.16 (AC), 0.25 (AG), 0.2 (AT), 0.08 (CG), 0.2 (CT), and 0.11 (GT); 2—stationary sites rate equal to 0.38 (A), 0.14 (C), 0.2 (G), and 0.28 (T); and 3—assuming monophyly for C. indologenes taxa. The sequences of the P-23 (IND-8) and P-133 (IND-3) were deposited in the GenBank with accession number KY488544 and KY575027, respectively. The other Bla B1 sequences of Chryseobacterium sp. were obtained from the GenBank database.
Results
The susceptibility test of the two C. indologenes showed MICs >64 μg/mL for amikacin, ceftriaxone, and cefuroxime; >32 μg/mL for ampicillin; >16 μg/mL for colistin, imipenem, and meropenem, and >128 μg/mL for piperacillin/tazobactam. P-133 was sensitive to ciprofloxacin and P-23 to cefepime. However, P-23 showed reduced sensitivity to ceftazidime, ciprofloxacin, and tigecycline (Table 1). No PCR amplicons were observed for the genes blaOXA, blaSHV, blaCTX-M-1; blaCTX-M-2; blaCTX-M-8; blaCTX-M-9; blaVIM; blaGES; blaKPC; and blaNDM, when tested by PCR.
Antimicrobial Susceptibility Test of the Chryseobacterium indologenes Isolates
The sequence analysis of the two isolates allowed the detection of the BlaB1 gene, with similarity of 99.1% with the IND-3 allele (P-133) and 98.6% with the IND-8 allele (P-23). Even though most mutations were silent in both sequences (P-23 and P-133), only the P133 sequence showed a single mutation at position T355G, which corresponds to a nonsynonymous substitution of the amino acid at position 119 (Ser→Ala) (Figs. 1 and 2), compared with the reference sequence NG_049232.1 (IND-3 allele).

Alignment between amino acid sequences of the samples M11189.1, M63556.1, NG_049232.1, KY575027, NG_049237.1, and KY488544, showing the mutant site 119 and the zinc binding sites described by Bebrone. 25
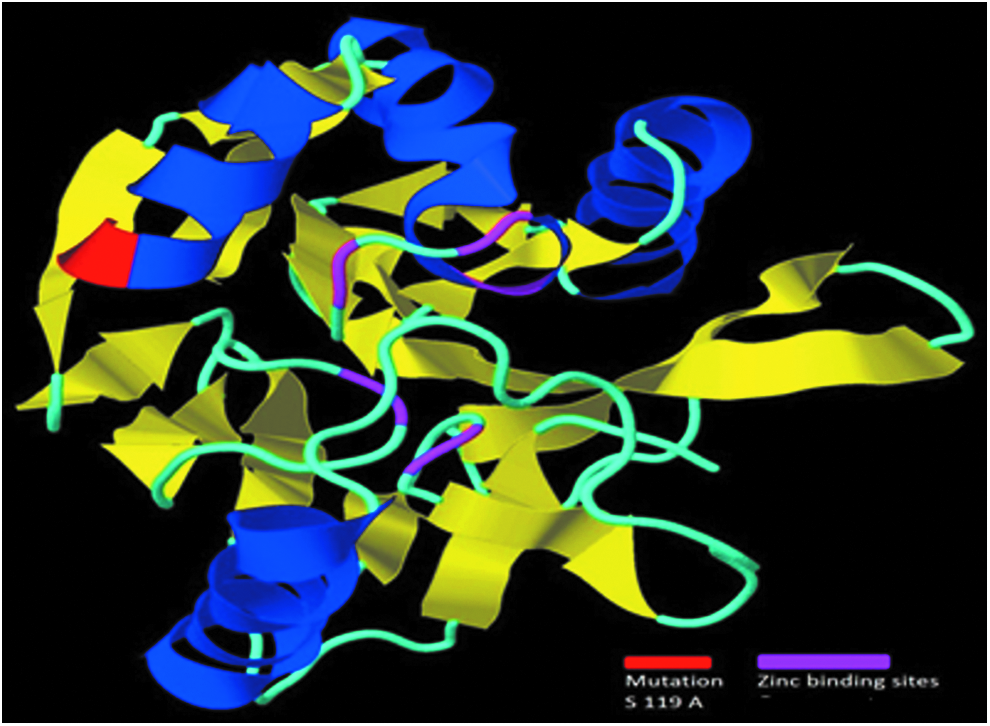
The mutant site 119 (Ser→Ala) and the zinc binding sites described by Bebrone. 25
The multiple alignment of M11189.1, M63556.1, NG_049232.1, KY575027, NG_049237.1, and KY488544 amino acid sequences showed that both zinc binding sites (Metallo-beta-lactamase), His116-His118-His196 and Asp120-Cys221-His263, described by Bebrone 25 were conserved between the sequences, as determined by comparison with domains deposited in the Protein Data Bank, verified by the I-TASSER server (Figs. 1 and 2). The divergences between positions result from multiple alignment. The three-dimensional models, generated from the primary structures of the amino acid reference sequence NG_049232.1 and the KY575027, obtained by the I-TASSER server, presented c-value scores equal to −0.48 and −0.49, respectively (larger than the average −1.5 for this parameter).21,26 Both models also presented an arrangement αββα, composed of two central β-sheets with five α-helices around, corroborating with the structures mentioned by Bebrone and Palzkill (Fig. 2).25,27
In the phylogeny cladogram (Fig. 3), it was observed that the Bla B1 gene present in C. indologenes forms a monophyletic group, compared with other BlaB1 of the Chryseobacterium genus. In this cladogram, the KY575027 sequence forms a monophyletic group with IND-3, and KY488544 forms a monophyletic group with IND-8, IND-10, and IND-16.
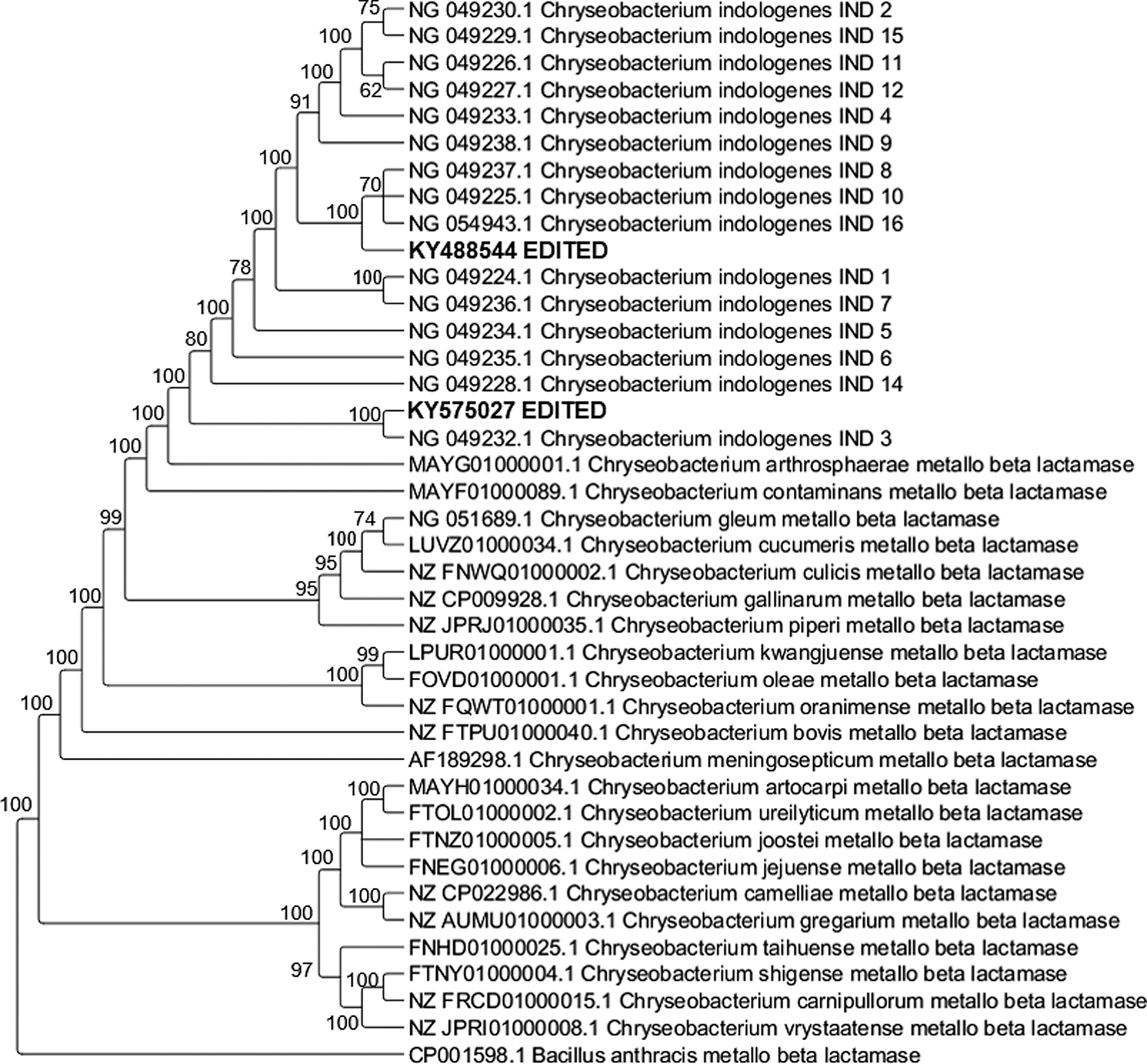
Molecular phylogenetic analysis by Bayesian method.
Discussion
C. indologenes is an emergent pathogen responsible for different nosocomial infections. 28 Studies indicate that infections caused by C. indologenes are more frequent in the elderly over 65 years, in immunosuppressed patients, and in newborns.1,3,4,29–31 The two patients included in this study are indeed older than 65. Regarding the susceptibility test, the absence of criteria for break-point levels of antibiotic as per CLSI reference manual, 14 specifically for this specie, as well as the different methods applied in different laboratories, complicated the correct interpretation of the results and the choice of antibiotics for the treatment of these patients. Another important point that requires attention is that this genus is naturally resistant to aminoglycosides, extended-spectrum cephalosporins, aztreonam, imipenem, meropenem, chloramphenicol, and erythromycin.29,32,33 These antibiotics are commonly recommended for empirical treatment of infections caused by Gram-negative bacteria. 29 According to the SENTRY Antimicrobial Surveillance Program, 9 ciprofloxacin, levofloxacin, sulf./trimethoprim, piperacillin/tazobactam, ceftazidime, and cefepime are the most active antibiotics against C. indologenes. In this study, the P-133 isolate was sensitive only to ciprofloxacin, whereas P-23 was sensitive only to cefepime with reduced sensitivity to ceftazidime, ciprofloxacin, and tigecycline. A similar resistance pattern has been described by other authors from different countries,1,29,30,34 although a different pattern, characterized by high susceptibility to several classes of antibiotics, has also been described4,6; in addition, it contrasts with data published by SENTRY. 9
The analysis of the three-dimensional structure of the BlaB1 demonstrates that, despite the occurrence of a nonsynonymous mutation, the three-dimensional structure of the enzyme underwent few modifications, not affecting, in principle, the activity of this protein. The c-score values obtained by the three-dimensional modeling of NG_049232.1 and KY575027 demonstrated high reliability for both models. In addition, both structures were highly aligned with the three-dimensional structure of IND-7, obtained by X-ray crystallography in the study by Yamaguchi et al. 35 and deposited in the Protein Data Bank with the 3L6N code, obtaining normal z-score values equal to 3.4 (good alignments show values higher than 2.0) with respect to 3L6N. 35 The phylogenetic analysis indicates that Chryseobacterium arthrosphaerae forms a monophyletic group with the C. indologenes group. Inside this group, it was observed that the KY575027 (P-133) emerged from a lineage of IND-3, while IND-8, IND-10, and IND-16 emerged from KY488544 (P-23), which has not been previously reported in Brazil. The high values of bootstrap sustain the reliability of this phylogeny. Since there are no reports of this mutation in other INDs, involving the expression of this variant, further studies are necessary to confirm this hypothesis. These new multidrug resistant strains should be acknowledged by hospital and clinical staffs, emphasizing the need for effective measures aimed to prevent the spread of this pathogen and the risks of infections, as well as criteria to evaluate the susceptibility of these bacteria to antibiotics to guide proper therapeutic decisions. The rapid identification of this pathogen in clinical laboratories is also necessary for appropriate empiric therapy for the patients by the clinical staffs.
Footnotes
Acknowledgments
This work has been funded by the Fundação de Amparo à Pesquisa do Estado do Amazonas-FAPEAM, Programa de Apoio à Pesquisa UNIVERSAL AMAZONAS; Fundação de Hematologia e Hemoterapia do Amazonas-HEMOAM.
Disclosure Statement
No competing financial interests exist.