
Abstract
Background:
Septicemia in children in mainland China has recently become a public health concern.
Methods:
A meta-analysis was performed on studies investigating the prevalence of cephalosporin-resistant Escherichia coli isolated from children with septicemia in mainland China from 2007 to 2017 following a search of relevant databases.
Results:
A total of 43 articles reporting 11 cephalosporins were included in the review. The results of the meta-analysis revealed that for the first-generation cephalosporins, the pooled summarized prevalence of resistance to cefazolin was 74.96% (95% confidence interval [CI]: 64.79–83.91) and cephalothin resistance was 62.28% (95% CI: 36.45–100). Regarding the second-generation cephalosporins, cefoxitin-resistant E. coli comprised 23.85% (95% CI: 10.60–40.40) and cefuroxime resistance was 60.32% (95% CI: 51.25–68.73). For the third-generation cephalosporins, the pooled summarized prevalence of resistance was 51.34% for cefotaxime (95% CI: 40.08–62.54), 40.43% for ceftazidime (95% CI: 31.07–50.15), 45.51% for cefoperazone (95% CI: 20.41–70.61), 12.10% for cefoperazone/sulbactam (95% CI: 6.55–18.76), 62.99% for ceftriaxone (95% CI: 55.00–70.98), and 0% for cefotetan. Among the fourth-generation cephalosporins, resistance to cefepime was 34.08% (95% CI: 25.91–43.31).
Conclusions:
Most third-generation cephalosporins (e.g., cefotaxime and ceftriaxone) retained high resistance rates throughout the 11-year study period without significant changes. The new fourth-generation cephalosporin, cefepime, is rapidly gaining resistance. Interestingly, ceftazidime, cefepime, and cefoperazone/sulbactam showed a recent decreasing trend of drug resistance. These situations may present a risk for treating children with septicemia and should be closely monitored and treated.
Introduction
Septicemia is a type of bloodstream infection that causes significant morbidity and mortality.1,2 In addition, septicemia is a serious disease stimulated by bacterial infection and is more common among children than adults throughout the world, especially for neonates.3,4 From 2003 to 2015, the number of speculated global cases of sepsis and severe sepsis was at least 5.68 million and 3.51 million per year, respectively, which is 437 and 270 cases per 100,000 individuals each year, respectively.5,6 It is estimated that 1.2 million children worldwide are stricken with sepsis each year, from a systematic review between 1979 and 2016. 7 Furthermore, U.S. studies also indicated that >70,000 children were hospitalized for sepsis at a cost of ∼$5.0 billion and a mortality rate of ≤20%.8,9
The causative agents of septicemia are diverse, including all types of gram-positive10–14 and gram-negative bacteria. 15 Among them, Escherichia coli is the most common gram-negative bacteria associated with septicemia.16–18 Recently, since E. coli drug resistance continues to rise and new multidrug-resistant E. coli have emerged, 19 the clinical selection of effective antibiotics to treat E. coli infections in children has become a challenging issue. The Infectious Diseases Society of America views antimicrobial resistance as a serious threat to public health, patient safety, and national security, and has published policy recommendations for the US Congress to address the increasing rates of antibiotic resistance together with the decline in new antibiotic approval. 20
In both the United States and Europe, penicillin is combined with aminoglycoside antibiotics to treat neonatal sepsis 21 ; however, hospitals in China rarely carry out tests for the concentration of drugs in the blood. Due to the nephrotoxicity and ototoxicity associated with aminoglycosides, penicillin is used in combination with cephalosporins (often third-generation cephalosporins) or the third-generation cephalosporin alone to treat neonatal sepsis. 22 Cephalosporins 23 are a type of antibiotic, which display broad-spectrum inhibitory effects on both gram-positive and gram-negative bacteria. Cephalosporins include the following: (1) first-generation cephalosporins, which primarily comprise half of all broad-spectrum antibiotics and are mainly used to treat gram-positive bacterial infections (e.g., cefazolin and cefalotin); (2) second-generation cephalosporins, which are particularly effective against gram-negative bacteria (e.g., cefoxitin and cefuroxime); (3) third-generation cephalosporins, which have the characteristics of strong antibacterial activity, a broad antibacterial spectrum, and good β-lactamase stability. They can be used to treat normal drug-resistant bacteria (e.g., cefotaxime, ceftriaxone, and ceftazidime); and (4) fourth-generation cephalosporins, which were developed in the early 90s and generally exert a higher activity on most drug-resistant strains than the third-generation cephalosporins; however, they are also subject to very strict restrictions for clinical use.24,25
Over time, there has been an increase in the isolation of E. coli that are resistant to commonly used antibiotics from children with septicemia in China. 26 However, in reviewing past reports, the descriptions of E. coli resistance to cephalosporins have become somewhat fragmented regarding different regions and time periods. There is also a lack of reports presenting a systematic comparison and analysis of the resistance to the different generations of cephalosporin drugs. To understand the status of E. coli resistance to cephalosporin drugs in children with septicemia in China, as well as the associated developmental trends, we searched both Chinese and English databases for all articles describing cephalosporin resistance among E. coli strains isolated from children with septicemia in China from 2007 to 2017, and conducted a meta-analysis.
Materials and Methods
Search strategy and selection criteria
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 27 We searched the PubMed, EMBASE, EBSCO, ISI Web of Knowledge, Chinese National Knowledge Infrastructure (CNKI), and Wanfang (Chinese) databases to identify relevant studies of drug-resistant E. coli isolated from children with septicemia in China published between January 2007 and December 2017. The following search terms were used: “sepsis” or “septicemia” and “drug resistant” or “antibiotic resistant” or “antimicrobial resistance” and “Escherichia coli” or “E. coli” and “China.” In the Chinese databases, the key word “China” was removed from the search words because some reports in Chinese presented data from provinces or regions in China but did not mention the word “China” in the report. Additional articles were identified from the reference lists and review articles.
Inclusion and exclusion criteria
The inclusion criteria consisted of the following: (1) studies in which the drug resistance rates and total number of E. coli strains were available (or the available data to calculate these values).
The exclusion criteria consisted of the following: (1) studies with duplicate data; (2) studies with insufficient data; (3) data from review and abstracts; (4) E. coli strains isolated out of the study range (from January 2007 to December 2017); (5) E. coli strains isolated from countries other than China; (6) E. coli strains were not selected randomly. Before drug-resistant tests, those E. coli strains were preselected by other standards, such as the presence of certain genes; (7) E. coli strains isolated from individuals of other ages (i.e., not children, age ≥14) 28 ; and (8) E. coli strains isolated from fewer than 10 cases. The references of the selected articles and reviews were also scanned manually to identify any additional eligible studies.
Statistical analyses
Data regarding the total incidence of resistance for 11 cephalosporins from different generations in different regions and years were calculated independently using Microsoft Excel 12.0 (Microsoft Co., Ltd., Washington). All data manipulation and statistical analyses were performed using R-3.4.4 in this meta-analysis. A random-effects model was selected, given the possibility of significant heterogeneity between the studies. A stratified analysis was conducted in accordance with the geographic areas and subject enrollment time. Pooled prevalence rates and 95% confidence intervals (CIs) were calculated from raw proportions under a random-effects model (DerSimonian and Laird method). The data were entered and a statistical analysis was performed and presented as a forest plot. Forest plots were generated to show the prevalence proportions with corresponding 95% CIs for each study and the overall random-effects pooled estimate. Publication bias was detected by funnel plotting and the p value of an Egger's weighted regression analysis.
Results
Search results
In accordance with the literature retrieval method referred to in the Search Strategy and Selection Criteria section , we identified 1,332 articles published from 2007 to 2017 (55 in PubMed [English], 43 in EMBASE [English], 31 in EBSCO [English], 29 in ISI Web of Knowledge [English], 415 in CNKI [Chinese], and 759 in the Wanfang databases [Chinese]). After an initial evaluation of the titles and abstracts, 1,127 articles were excluded due to their irrelevance and duplication. The full text of the remaining articles was reviewed. A total of 94 articles were included after excluding those that only described the prevalence of mycobacteria and were not able to extract information regarding the rates of resistance, and those that provided rates of resistance but did not describe specific drugs. Among these 94 articles, 51 were excluded for the following reasons: 21 articles did not include data from 2007 to 2017; 8 articles did not originate from mainland China; 6 articles did not include data from children; 2 articles used the same samples; 2 articles provided incomplete information; and in 12 articles, E. coli strains were isolated from fewer than 10 cases. Finally, 43 articles were included in this systematic review and meta-analysis (Fig. 1).
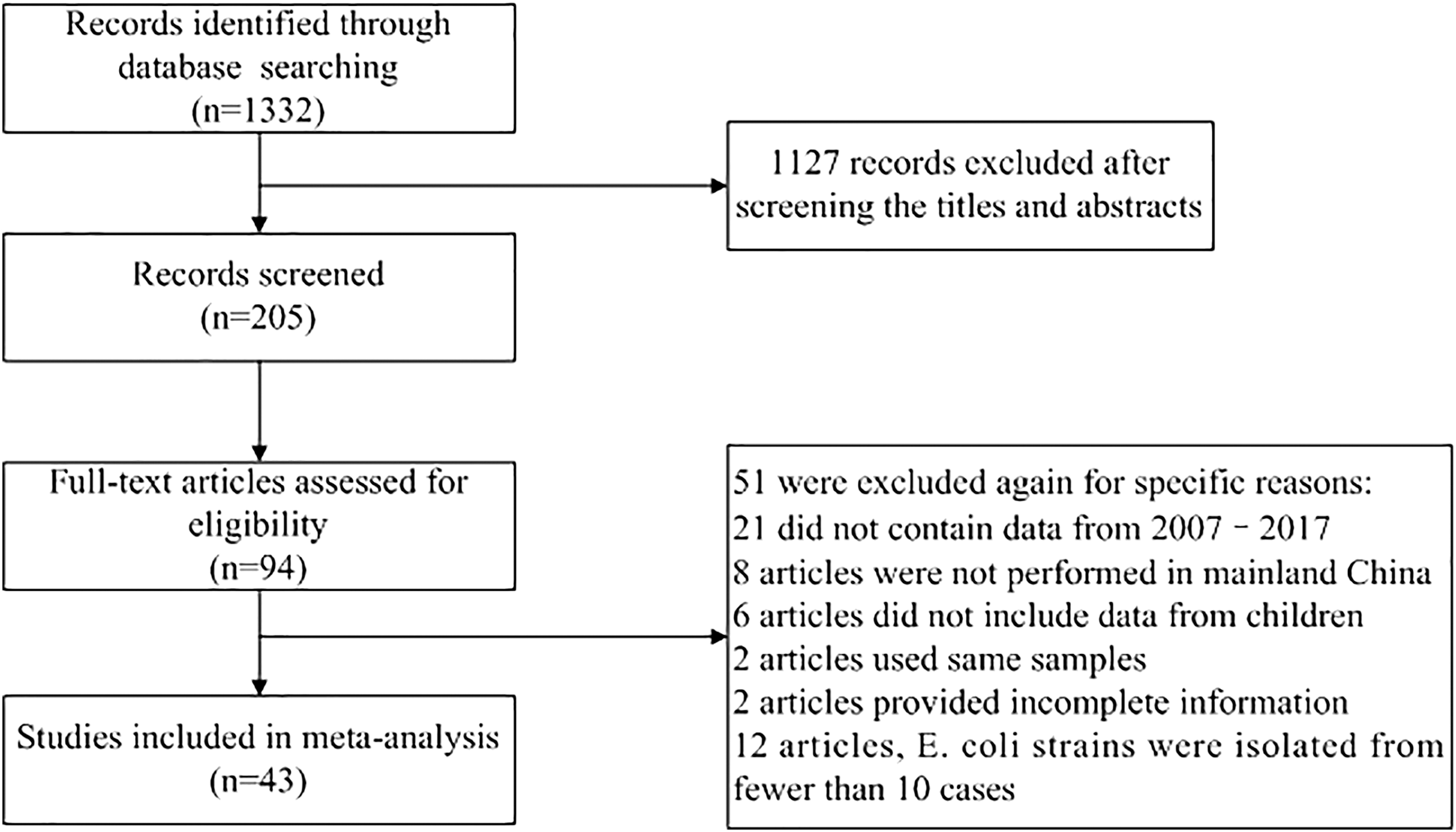
PRISMA flow diagram. Flowchart depicting the study selection process.
Characteristics of the eligible studies
A total of 43 eligible articles were included for analysis. Based on the setting of this study, the information in these articles was classified according to the different generations of cephalosporins, regions, and time periods. In general, China can be divided to seven regions, consisting of eastern, southern, northern, northwestern, southwestern, northeastern, and central China. If the information in an article covered different regions and could not be clearly distinguished, then the 17 articles were excluded from the subregional meta-analysis. We divided the 11 years of 2007 − 2017 into two time periods, 2007 − 2011 and 2012 − 2017. This was because the two time periods were roughly equal, and the Chinese government introduced strict clinical antibiotic use guidelines in 2012, which quickly achieved better implementation nationwide. Thus, separating the time periods might help us to observe the trend of E. coli resistance to cephalosporins over time and after the implementation of the government antibiotic use policy. 29 If the information in an article covers different time periods and could not be clearly distinguished, then the article was excluded from the subtime meta-analysis. The total number of articles and other detailed information for the different regions and time periods are listed in Table 1.
Characteristics of the Eligible Studies
First, the first-generation cephalosporins. Second, the second-generation cephalosporins. Third, the third-generation cephalosporins. Fourth, the fourth-generation cephalosporins. NA, not available; CZO, cefazolin; KF, cephalothin; FOX, cefoxitin; CXM, cefuroxime; CTX, cefotaxime; CAZ, ceftazidime; CFP, cefoperazone; SCF, cefoperazone/sulbactam; CRO, ceftriaxone; CTT, cefotetan; FEP, cefepime.
The incidence of drug resistance toward first-generation cephalosporins in mainland China
In total, 22 studies, which included 584 samples, reported the incidence of cefazolin resistance in mainland China (Table 2). There were only 58 samples included in three studies for cephalothin.
Incidence of the First-Generation Cephalosporin Resistance in Mainland China
n, number of events; N, total number of samples from the studies; NA, the data were not applied to the statistical calculation.
Our meta-analysis revealed that the pooled summarized prevalence estimate of cefazolin was 74.96% (95% CI: 64.79–83.91) (Supplementary Fig. S1). The resistance rate of E. coli to cefazolin did not change significantly between 2007 − 2011 and 2012 − 2017. The pooled summarized prevalence estimate of cephalothin resistance was 62.28% (Supplementary Fig. S2). The regional pooled prevalence estimate of cefazolin in central China was 89.28% (95% CI: 77.24–100.00), which was higher than in eastern China (69.88%), southern China (71.12%), and southwestern China (69.18%).
The incidence of drug resistance toward second-generation cephalosporins in mainland China
The results regarding the incidence of cefoxitin and cefuroxime (second-generation cephalosporins) resistance are shown (Table 3). A total of 12 studies, including 280 samples, reported the incidence of cefoxitin resistance in mainland China. There were 16 studies, including 408 samples, that reported the incidence of cefuroxime resistance in mainland China.
Incidence of the Second-Generation Cephalosporin Resistance in Mainland China
n, number of events; N, total number of samples from the studies; NA, the data were not applied to the statistical calculation.
The pooled summarized prevalence estimate of cefoxitin was 23.85% (95% CI: 10.60–40.40) (Supplementary Fig. S3). The pooled prevalence estimate of cefuroxime resistance was 60.32% (95% CI: 51.25–68.73) (Supplementary Fig. S4). The prevalence of cefuroxime was significantly higher than cefoxitin (60.32% vs. 23.85%). When the resistance rate between 2007 and 2011 was compared with that of 2012–2017, there was an increasing trend toward cefuroxime resistance during the later years (52.25% vs. 70.56%).
The incidence of drug resistance toward third-generation cephalosporins in mainland China
Our study consisted of 22, 35, 3, 17, 26, and 4 studies, which included 502, 870, 115, 346, 644, and 91 samples for cefotaxime, ceftazidime, cefoperazone, cefoperazone/sulbactam, ceftriaxone, and cefotetan (third-generation cephalosporins) in drug resistance tests, respectively, from mainland China (Table 4).
Incidence of the Third-Generation Cephalosporin Resistance in Mainland China
n, number of events; N, total number of samples from the studies; NA, the data were not applied to the statistical calculation.
The pooled summarized prevalence estimate of cefotaxime was 51.34% (95% CI: 40.08–62.54) (Supplementary Fig. S5). The resistance rate of E. coli to cefotaxime did not change significantly between 2007 − 2011 and 2012 − 2017. The regional pooled prevalence estimate of cefotaxime in eastern China was 30.42% (95% CI: 12.50–57.23), which is much lower than in southern China (53.75%), southwestern China (61.93%), and central China (58.20%).
The pooled summarized prevalence estimate of ceftazidime was 40.43% (95% CI: 31.07–50.15) (Supplementary Fig. S6). The resistance rates to ceftazidime exhibited a downward trend in recent years (44.08%; 2007 − 2011 vs. 33.31%; 2012 − 2017). In addition, the pooled summarized prevalence estimate of cefotetan and cefoperazone was 0% and 45.51% (95% CI: 20.41–70.61), respectively (Supplementary Fig. S7).
The pooled summarized prevalence estimate of cefoperazone/sulbactam was 12.10% (95% CI: 6.55–18.76) (Supplementary Fig. S8), which was much lower than most of the other cephalosporins. In addition, in the past few years, the prevalence of cefoperazone/sulbactam even displayed a decreasing trend (11.13%; 2007 − 2011 vs. 4.65%; 2012 − 2017).
The pooled summarized prevalence estimate of ceftriaxone was 62.99% (95% CI: 55.00–70.98) (Supplementary Fig. S9). At the time level, the pooled prevalence of ceftriaxone in the later years remained similar to that between 2007 and 2011.
The incidence of drug resistance toward fourth-generation cephalosporins in mainland China
There were a total of 29 studies included in our analysis, which comprised 718 samples that reported the incidence of cefepime resistance in mainland China (Table 5). The pooled summarized prevalence estimate of cefepime was 34.08% (95% CI: 25.91–43.31) (Supplementary Fig. S10). In the time analysis, the pooled prevalence of cefepime decreased over the last few years, from 36.45% (95% CI: 19.85–57.05; 2007 − 2011) to 23.53% (95% CI: 12.49–36.78; 2012 − 2017).
Incidence of the Fourth-Generation Cephalosporin Resistance in Mainland China
n, number of events; N, total number of samples from the studies; NA, the data were not applied to the statistical calculation.
Publication bias
Since a minimum of 10 studies are required to assess any potential publication bias, it was only possible to conduct this analysis for eight cephalosporins. Except for cephalothin, cefoperazone, and cefotetan, the shapes of the funnel plots were symmetrical for the eight studies of cephalosporin resistance (Supplementary Fig. S11, S12, S13, S14, S15, S16, S17, S18), which suggested that there was no publication bias. Moreover, all of the data had corresponding p values >0.05, which further verified the results of the funnel plots.
Discussion
Since cephalosporins are widely used to treat E. coli infections in children with septicemia, bacterial resistance has been monitored during the past decades in China. 30 However, such data are scattered, not written in English, and have not been effectively disseminated to the world. Thus, a meta-analysis was performed to elucidate the overall situation and trend of cephalosporin-resistant E. coli isolated from children with septicemia in China. Among a total of 11 cephalosporins, cefazolin and cephalothin (first-generation cephalosporins) displayed the highest resistance rates, pooled to be 74.96% (95% CI: 64.79–83.91) and 62.28% (95% CI: 36.45–100), respectively. These high resistance rates are likely explained by the fact that they represent the earliest cephalosporins to be used. Ceftriaxone (generation 3) displayed the next highest resistance of 62.99% (95% CI: 55.00–70.98), followed by cefuroxime (generation 2) with 60.32% (95% CI: 51.25–68.73), which may be attributed to the widespread use of these drugs in China.
Other second- or third-generation cephalosporins, including cefotaxime with 51.34% (95% CI: 40.08–62.54), cefoperazone with 45.51% (95% CI: 20.41–70.61), and ceftazidime 40.43% (95% CI: 31.07–50.15), display midrange resistance. However, cefoxitin (generation 2) with 23.85% (95% CI: 10.60–40.40) was mostly sensitive, which was possibly due to the infrequent usage in the past. A meta-analysis on the antimicrobial resistance of pathogens for neonatal septicemia in China showed that almost 50% of E. coli were resistant to third-generation cephalosporins from 2009 to 2014. 25 Another meta-analysis about community-acquired neonatal and infant sepsis in 13 developing countries (not including China) showed that susceptibility to third-generation cephalosporins was 56% and 64% for neonates and older infants, respectively. 31 These results were in line with our findings regarding the resistance of E. coli to third-generation cephalosporins.
Cefepime resistance as a fourth-generation cephalosporin was found to be 34.08% (95% CI: 25.91–43.31), indicating that the latest antibiotics are also rapidly becoming resistant, posing challenges to the future treatment of bacterial infections.32,33 Fortunately, cefepime displayed a reduced resistance rate after 2012. Of note, cefoperazone/sulbactam exhibits an extremely lower resistance prevalence. The pooled summarized prevalence estimate of cefoperazone/sulbactam was 12.10% (95% CI: 6.55–18.76), which was much lower than other cephalosporins, and the rate of 45.51% for cefoperazone (95% CI: 20.41–70.61) when used alone. This suggested that an appropriate drug complex may be a useful method of treatment for preventing increased resistance.
Among all the 11 cephalosporins that had sufficient data and were studied over time, the resistance rates of cefazolin, cefotaxime, and ceftriaxone remained elevated over 11 years without significant changes. Contrary to our expectations, only cefuroxime displayed a significant increase in drug resistance in recent years, increasing from 52.25% (95% CI: 26.73–77.77), between 2007 and 2011, to 70.56% (95% CI: 58.18–81.56), between 2012 and 2017. Ceftazidime, cefepime, and cefoperazone/sulbactam even displayed a trend toward decreasing drug resistance over the past 5 years. These phenomena suggest that most cephalosporins exhibit a recent trend of a drug resistance plateau. This may be a benefit arising from the increasingly strict control of antibiotics by Chinese health regulators in recent years (e.g., Administrative Measures for the Clinical Use of Antibacterial Drugs), particularly after 2012, 28 suggesting that the strict government drug control measures that were introduced in 2012 may have helped to prevent bacterial resistance rates from rising. From the limited data, the general difference in the prevalence of cefazolin, cefuroxime, ceftriaxone, and cefepime resistance among the different regions was not significant, whereas the prevalence of cefotaxime resistance in eastern China appears to be significantly lower than in southern China, southwestern China, and central China.
This study had several limitations. Significant heterogeneity was observed among certain studies. This may be due to inconsistencies among the subject demographic information, standards of quality, and methodologies adopted by different studies. Those inconsistencies would certainly influence the results of this meta-analysis. Moreover, some of the original information from the geographic and time segment subgroup analysis was insufficient, which unfortunately prevents us from obtaining further in-depth findings.
In conclusion, we performed a systematic review and meta-analysis on the prevalence of cephalosporin-resistant E. coli isolated from children with septicemia in mainland China from 2007 to 2017. The most commonly used cephalosporins, which belong to the second and third generations, have already developed high resistance rates. Moreover, the new-fourth generation cephalosporin, cefepime, is also rapidly gaining resistance status. This situation may present a risk for the treatment of septicemia in children and should be closely monitored and treated.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.