
Abstract
This study was designed to investigate, at the molecular level, the antimicrobial resistance mechanisms of different antimicrobial resistance genes, including, extended-spectrum β-lactamases, AmpC β-lactamases, class 1 and 2 integrons, and plasmid-mediated quinolone resistance genes of Gram-negative bacteria isolated from clinical settings in Egypt. A total of 126 nonduplicate Gram-negative isolates were recovered from different clinical samples taken from hospitalized patients in Egypt in 2014. Antimicrobial susceptibility testing showed that, 93.6% (118/126) of the isolates had a multidrug-resistant phenotype. Interestingly, we reported a high level of antimicrobial resistance nearly for all tested antibiotics; to our knowledge, this is the first report from Egypt indicating very high level of antibiotic resistance in Egypt. Polymerase chain reaction screening and DNA sequencing revealed that, 75.4% (95/126) of the isolates harbored at least one extended-spectrum β-lactamase-encoding gene, with blaCTX-M being the most prevalent (65.9%), followed by blaSHV (46.8%). The AmpC β-lactamase, blaCMY, was detected in 7.1% (9/126) of bacterial isolates, with blaCMY-42 being the most prevalent. Class 1 integrons were detected in 50.8% (64/126) of the isolates, and class 2 integrons were detected in 2.4% (3/126) of the isolates. The plasmid-mediated quinolone resistance gene, qnr, was detected in 58.7% (74/126) of the tested isolates, with qnrS being the most prevalent. Several antimicrobial resistance determinants were identified in Egypt for the first time, such as SHV-27, SHV-28, SHV-33, SHV-63, SHV-71, SHV-82, SHV-142, CMY-42, CMY-6, and the new CMY-72 like. This study highlights the importance of the conscious use of conventional antimicrobials to overcome the multidrug resistance problem.
Introduction
Infections caused by multidrug-resistant (MDR) Gram-negative bacteria have been reported as one of the most onerous growing problem worldwide. Moreover, this problem is exaggerated by the limited pipeline of new antibiotics in production. This results in high morbidity and mortality rates and increased health care costs worldwide. It is, therefore, imperative to understand antimicrobial resistance in Gram-negative bacteria at the molecular level to enable the development of strategies, to overcome this problem. Furthermore, such information could be helpful for all public health officials, practicing physicians, prescribers, and clinical microbiologists, and to guide specific empirical antibiotic therapy. 1 Our previous studies showed high levels of carbapenem resistance in clinical settings in Egypt.2,3 Moreover, the problem of high carbapenem resistance was also recorded in different countries, especially in developing countries.4,5
Extended-spectrum β-lactamases (ESBLs) have been recorded as one of the major antimicrobial resistance mechanisms. ESBLs include a group of β-lactamases that hydrolyze the extended-spectrum cephalosporins, the penicillins, and monobactams, but not carbapenems. 6 Therefore, ESBL producers are difficult to treat because such strains are resistant to multiple antimicrobial agents and therapeutic options can be limited, which may lead to therapeutic failure. Moreover, previous studies have reported the poor therapeutic outcome when patients with severe infection due to ESBL producers are treated with antibiotics to which the organisms are resistant. 7 In Egypt and other developing countries, the β-lactam antibiotics, such as the cephalosporins, have become first-choice empirical-use antibiotics for the treatment of bacterial infections. 8 Moreover, a higher mortality from bacteremia with ESBL producers than nonproducers has been reported. 9 Therefore, it is imperative to understand the molecular mechanism of β-lactam resistance, especially in developing countries due to the high dependence on these drugs as an economic and available weapon for the treatment of Gram-negative bacterial infections.
Among the most serious mechanisms, which are responsible for the worldwide dissemination of MDR microorganisms, is the ability of bacteria to acquire and disseminate exogenous genes through mobile genetic elements, such as insertion sequences, transposons, plasmids, and genomic islands. 10 Moreover, the unique mechanism involving integrons for the dissemination of resistance genes contributes to the rapid transmission of antibiotic resistance in bacterial pathogens. 10 This mechanism acts as a natural genetic engineering system capable of the capture and excision of antimicrobial resistance genes by a site-specific recombination system. 11 There are five different classes of integron, each with a specific integrase gene. 11 However, class 1 integrons are the most widespread among MDR Gram-negative bacteria and act as reservoirs and exchange platforms of resistance genes in these bacteria. 11
In Egypt, several independent studies on MDR bacteria have reported on either one category of antimicrobial resistance gene determinants or on specific bacterial strains.11–15 However, the prevalence of different categories of antimicrobial resistance gene determinants, including ESBL, AmpC, integrons, and plasmid-mediated quinolone resistance genes, among different bacterial strains remained untested. Therefore, this study was designed to characterize, at the molecular level, the mechanism of resistance of a wide range of antimicrobial resistance genes among Gram-negative bacteria in Egypt.
Materials and Methods
Bacterial isolates
In 2014, 128 nonduplicate Gram-negative isolates were recovered from clinical samples that included blood, urine, respiratory sputum, pus, skin/wound, and other sources (Fig. 1), and previously showed high resistance to carbapenem antibiotics. 2 Two isolates were incapable to be recultured during the various experiments; therefore, they were excluded in this study and only the results of 126 isolates were recorded. The isolates were obtained from 126 patients hospitalized in different wards from 6 hospitals in four Egyptian cities: Kafr El-Sheikh city (Kafr El-Sheikh City Public Hospital, Kafr El-Sheikh Legitimacy Society Hospital and Alobour Hospital), Baltim city (Baltim Legitimacy Society Hospital), Alreyad city (Alraghama Hospital), and Cairo city (National Cancer Institute). 2 Most of the isolates were previously identified to be Klebsiella spp. (n = 89); however, Escherichia coli (n = 19), Serratia marcescens (n = 8), Pseudomonas aeruginosa (n = 7), Salmonella arizonae (n = 1), Providencia stuartii (n = 1), and Morganella morganii (n = 1) were also identified (Fig. 1). Klebsiella pneumoniae isolates were confirmed in our previous study by analysis of the 16S-23S rRNA internal transcribed spacer region, while the other bacterial isolates were identified using the API 20 E detection system (BioMérieux, Marcy-l'Etoile, France). 2
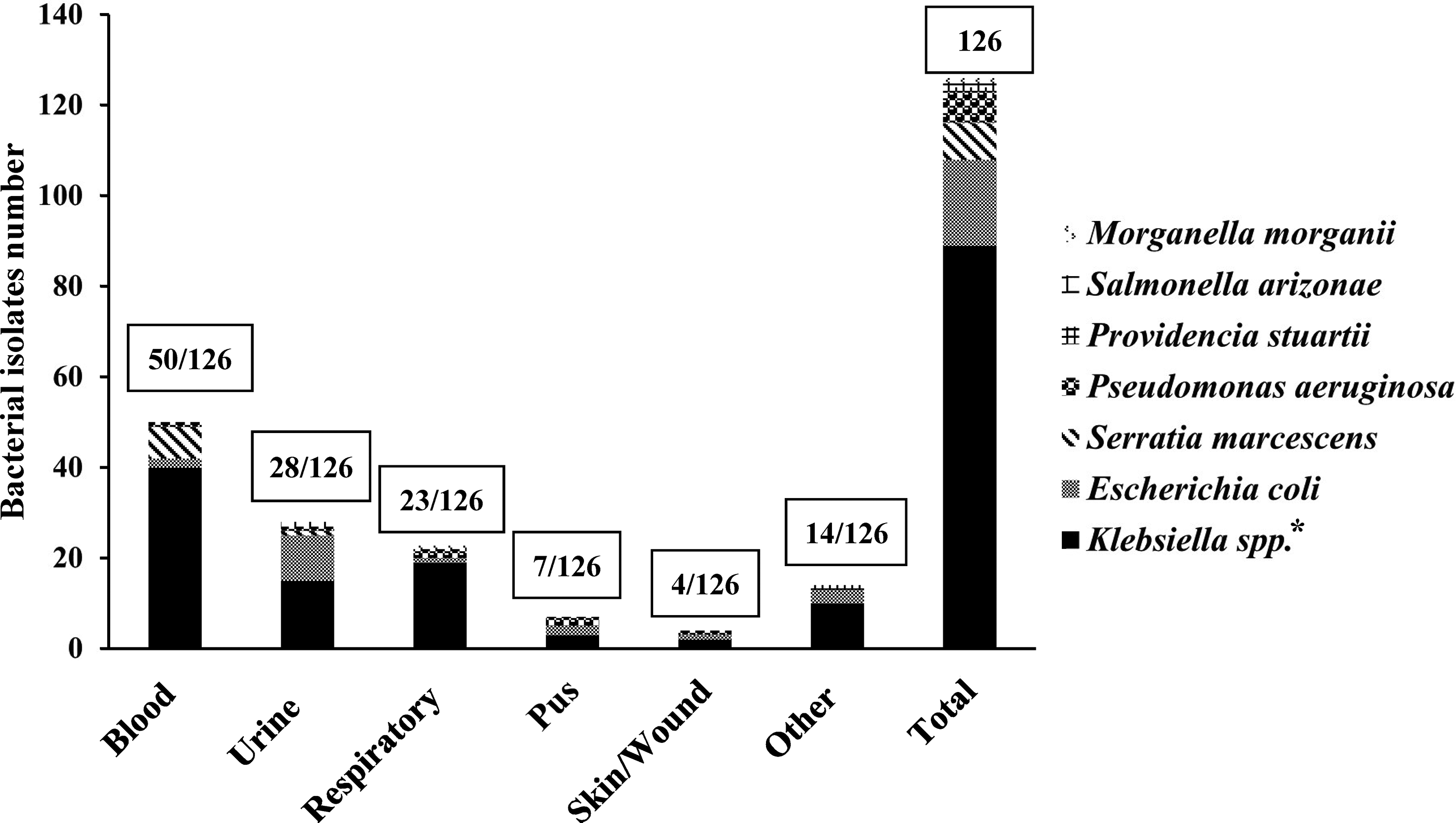
Distribution of isolates among clinical specimens. *Eighty-eight isolates of Klebsiella pneumoniae, one isolate of Klebsiella oxytoca.
Antimicrobial sensitivity testing
The bacterial isolates were previously tested for antimicrobial sensitivity phenotypes to different classes of antibiotics by Kirby–Bauer disc diffusion method on Mueller–Hinton agar plates. 2 Moreover, in this study, the isolates were also tested for resistance to cefotaxime (CTX) and cefoxitin (FOX), and the results are estimated according to the guidelines of the Clinical and Laboratory Standards Institute. 16
Screening for β-lactamase-encoding genes
Polymerase chain reaction (PCR) was conducted to detect different β-lactamase-encoding gene families such as SHV, TEM, OXA, CTX-M, and CMY in bacterial isolates by using universal primers as previously described (Table 1).17,18 Previously described primers were used to detect whole SHV and CMY gene when required, based on consensus sequences that flank many β-lactamase genes. 17 Of note, all PCR experiments were performed using the DNA that was previously prepared for detection of carbapenemases. 2
Oligonucleotides Used in This Study
Molecular detection of class 1 and 2 integrons
Class 1 and class 2 integrons were detected as previously recorded. 17 Briefly, class 1 integron primers, 5′-CS and 3′-CS, which amplify the region between the 5′ and 3′ coding sequences, were used (Table 1), while class 2 integrons were detected by PCR using the primer pair hep74 and hep51 and two other primers, IntI2-F2 and IntI2-R2, located within class 2 integrons, to amplify fragments of the whole class 2 integron segment for complete sequencing of both DNA strands (Table 1).
Molecular detection of plasmid-mediated quinolone resistance genes
Multiplex PCR was used for plasmid-mediated quinolone resistance gene screening (the qnrA, qnrB, and qnrS genes) using previously described primers (Table 1). 17
Sequencing and analysis of sequence data
The detected PCR reaction products were analyzed by electrophoresis in 1.0%–2.0% agarose gels, followed by ethidium bromide staining, and visualized under ultraviolet light. The FastGene Gel/PCR extraction kit (Nippon Genetics Co., Tokyo, Japan) was used for purification of PCR fragments from agarose gels. Both DNA strands of the PCR product were sequenced using an ABI automatic DNA sequencer (Model 373; Perkin-Elmer, Foster City, CA). BLAST program available at the NCBI BLAST homepage (http://blast.ncbi.nlm.nih.gov/Blast.cgi) was used for similarity search study.
Results
Prevalence of clinical isolates with MDR Gram-negative bacteria
A total of 126 clinical isolates of Gram-negative bacteria were isolated from several Egyptian hospitals. An MDR phenotype was detected in 93.6% (118/126) of the isolates, where all P. aeruginosa, P. stuartii, M. morganii, and S. arizonae isolates were MDR (Fig. 2). Around 95.5% of K. pneumoniae, 90% of E. coli, and 75% of S. marcescens isolates showed MDR phenotype (Fig. 2). Resistance phenotypes to three or more antimicrobial agents from different antimicrobial classes were detected in all of these isolates.
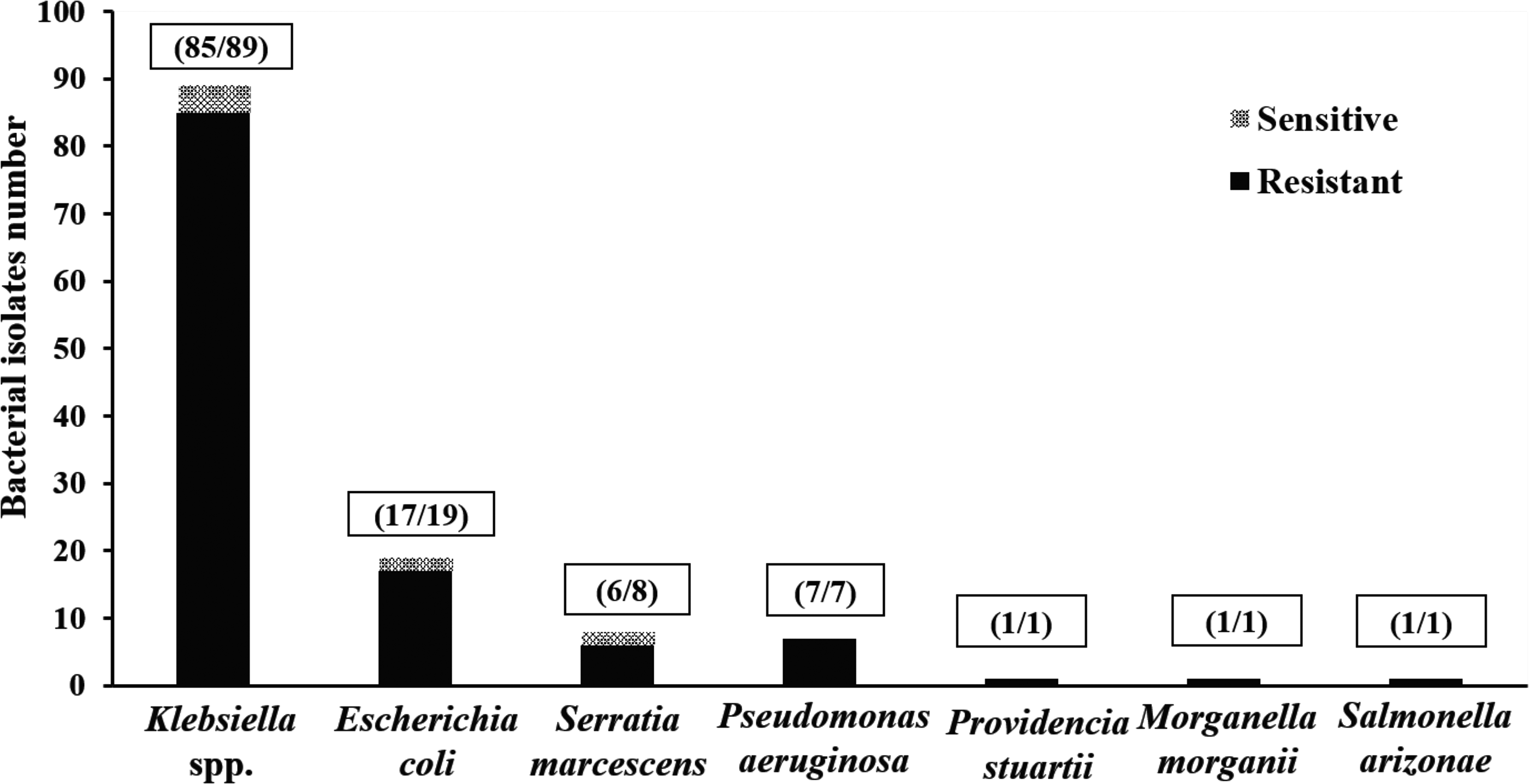
Incidence of multidrug-resistant clinical isolates of Gram-negative bacteria.
Prevalence of ESBL- and AmpC-encoding genes
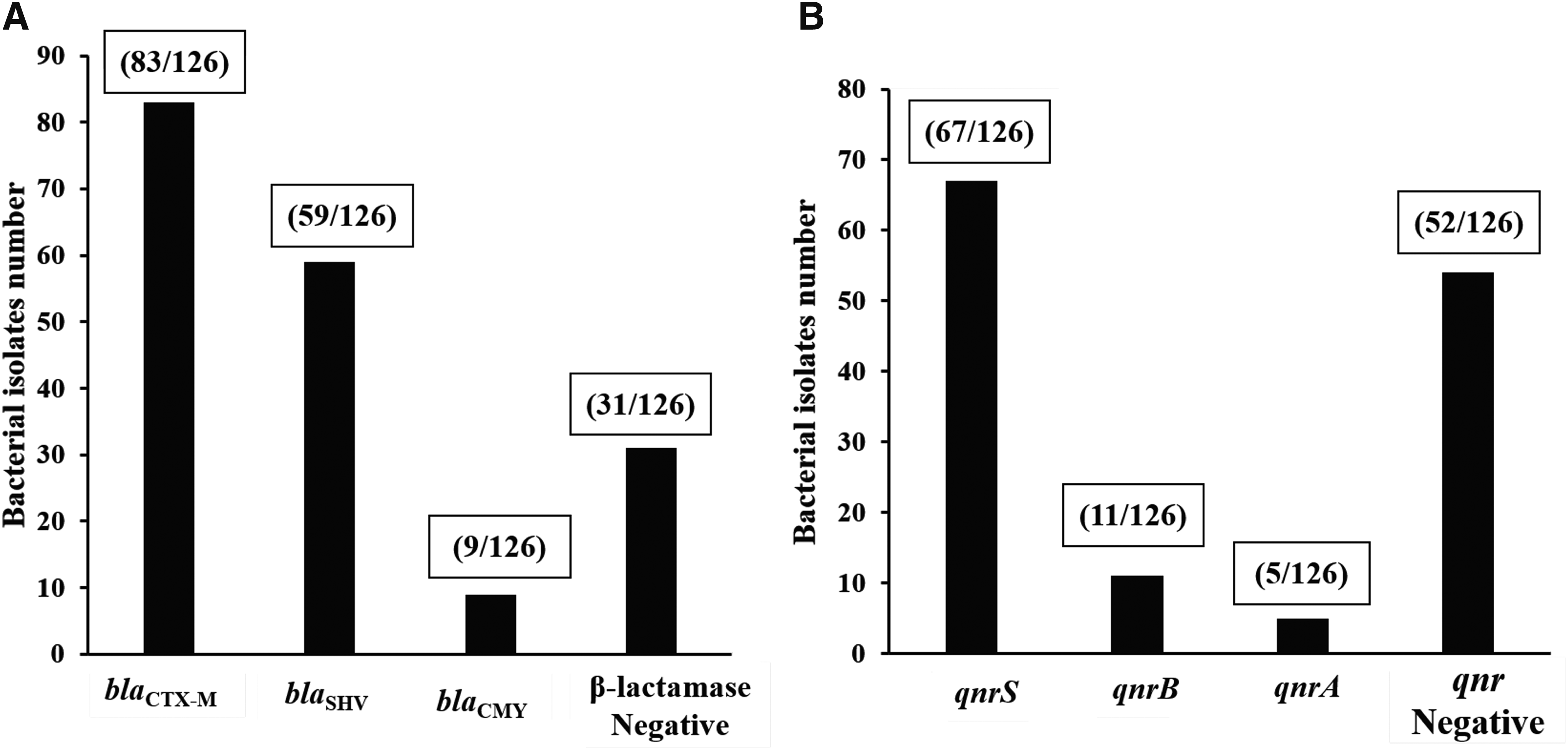
Screening by PCR and DNA sequencing identified various ESBL-encoding genes in 95 (75.4%) bacterial isolates (Table 2 and Fig. 3A). The most prevalent ESBL was blaCTX-M, which was present in 65.9% of bacterial isolates, 50 isolates harbored only blaCTX-M-15, 27 isolates harbored both blaCTX-M-15 and blaCTX-M-14, and 6 isolates harbored both blaCTX-M-15 and blaCTX-M-9 (Table 2 and Fig. 3A). blaSHV was the second most prevalent ESBL after blaCTX-M-, identified in 46.8% of bacterial isolates, while 22 isolates harbored blaSHV-11, 14 harbored blaSHV-28, 7 harbored blaSHV-12, 7 harbored blaSHV-142, and 4 harbored blaSHV-27, and blaSHV-71, blaSHV-63, blaSHV-82, blaSHV-33, and blaSHV-2 were each identified in single isolates (Table 2 and Fig. 3A). AmpC blaCMY- was detected in 7.1% of bacterial isolates, while six isolates harbored blaCMY-42, one harbored blaCMY-2, and one harbored blaCMY-6 and one new variant that is closely related to blaCMY-72, only differing by a Met126Leu substitution (Table 2 and Fig. 3A). Of note, many narrow-spectrum β-lactamase genes, such as blaSHV-1, blaTEM-1, and blaOXA-1, were identified; however, in this study, we focus on ESBL-encoding genes.
Molecular analysis of β-lactamases
Resistance Phenotypes and Prevalence of Integrons and Antimicrobial Resistance Genes in Gram-Negative Bacteria
aad, aminoglycoside adenyltransferase; AMC, amoxicillin/clavulanic acid; AMP, ampicillin; AZT, aztreonam; CAZ, ceftazidime; CHL, chloramphenicol; CIP, ciprofloxacin; CRO, ceftriaxone; CTX, cefotaxime; dfr, dihydrofolate reductase; ESBLs, extended-spectrum β-lactamases; FOX, cefoxitin; GEN, gentamicin; linF, lincosamide nucleotidyltransferase; NAL, nalidixic acid; sat, streptothricin acetyltransferase; TET, tetracycline.
Prevalence of class 1 and 2 integrons
PCR screening and DNA sequencing showed that 50.8% (64/126) of the isolates were positive for class 1 integrons. Interestingly, 18 gene cassette profiles were detected in 64 bacterial isolates and 6 bacterial isolates harbored 2 different gene cassette profiles (Table 2). Several gene cassettes were identified for dihydrofolate reductases (dfrA1, dfrA5, dfrA7, dfrA12, dfrA15, dfrA16, dfrA17, and dfrA30), which are responsible for resistance to trimethoprim; aminoglycoside adenyltransferases: aadA1, aadA2, aadA5, aadA6, aadA7, and aadA22, which are responsible for resistance to streptomycin and spectinomycin; aminoglycoside adenylyltransferase type B, aadB, which is responsible for resistance to kanamycin and low levels of gentamicin; aac(3)-Id, which is responsible for resistance to gentamicin and sisomicin; chloramphenicol acetyltransferase type B3, catB3, which confers resistance to chloramphenicol; and two different β-lactamases, blaOXA-10 and blaVIM-2. The most common profiles were for the dfrA17-aadA5, which was identified in 14 isolates, followed by dfrA1-aadA1 and dfrA12-orfF-aadA2 gene cassettes, which were identified in 8 isolates for each (Table 2).
Class 2 integrons were detected in only three (2.4%) isolates (Table 2), namely two K. pneumoniae isolates and one P. stuartii isolate. DNA sequencing of all class 2 integrons identified only two different gene cassette profiles. The identified gene cassettes were the aminoglycoside adenyltransferase (aadA1) gene cassette, which confers resistance to streptomycin and spectinomycin; the dihydrofolate reductase (dfrA1) gene cassette, which confers resistance to trimethoprim; the streptothricin acetyltransferase (sat2) gene cassette, which confers resistance to streptothricin; and the lincosamide nucleotidyltransferase (linF) gene cassette, which confers resistance to lincosamides.
Prevalence of plasmid-mediated quinolone resistance genes
Multiplex PCR screening detected the plasmid-mediated quinolone resistance gene, qnr, in 58.7% of the tested isolates (Table 2 and Fig. 3B). qnrS was the most prevalent qnr and was identified in 53.2% of isolates, followed by qnrB, identified in 8.7% of isolates, and finally, qnrA, identified in 3.9% of isolates (Table 2 and Fig. 3B).
Discussion
The development and spread of antibiotic resistance in clinical practice is a major threat to human health worldwide. In Egypt and other developing countries, data are lacking regarding the distribution of different categories of antimicrobial resistance gene determinants (ESBLs, AmpC-β-lactamases, integrons, and plasmid-mediated quinolone resistance genes) among Gram-negative bacteria. Previously, we reported high level of carbapenem resistance among clinical Gram-negative bacteria from Egypt. 2 Therefore, in this study, the same bacterial isolates were used to detect the other different mechanisms responsible for clinical Gram-negative bacteria resistance at the molecular level in Egypt.
The production of ESBLs by Gram-negative bacteria is a major resistance mechanism. 6 ESBL production has been previously investigated in Egypt.1,19,20 However, such studies at the molecular level are very rare in Egypt. Our results demonstrated that ESBL-encoding genes were detected in 75.4% of bacterial isolates, which is much higher than previous findings from Egypt.19,20 The high prevalence of ESBL production in Egypt compared with many European countries is attributed to the lack of controlled access to antibiotics in Egypt, with many antibiotics being available over the country. 19 The most prevalent ESBL-encoding gene was blaCTX-M-15 (65.9%), which is in accordance with the results of other studies carried out in Egypt and Europe, which reported CTX-M-15 as the predominant ESBL type. 19 blaSHV is second in prevalence to blaCTX-M-15 (46.8%), with blaSHV-11 being the most common, which is in agreement with previous results from Egypt. 19 blaSHV-2 and blaSHV-12 were previously detected in nosocomial and community-acquired K. pneumoniae in Egypt. 21 However, to our knowledge, this report is the first to demonstrate the occurrence of SHV-27, SHV-28, SHV-33, SHV-63, SHV-71, SHV-82, and SHV-142 variants in Egypt. Our results indicate high variability of SHV subtypes in Egypt.
AmpC β-lactamases is responsible for resistance to a wide variety of β-lactam antibiotics, mainly to 7-methoxy-cephalosporins (cephamycins). One of the major problems of AmpC β-lactamases is that the high-level of its expression may mask the recognition of ESBLs because AmpC-producing organisms can act as a hidden reservoir for ESBLs. 22 Although several groups of AmpC β-lactamases have been identified, the most common are the CMY-type AmpC β-lactamases. 14 blaCMY was detected in 7.1% of the bacterial isolates, which was a higher rate than that previously recorded in different countries, including Egypt (3%). 14 This could be explained by the difference in bacterial source; our bacterial isolates were isolated from infected patients, but in the previous study, bacterial isolates were isolated from healthy workers. Moreover, it is much higher than that detected previously in Iran. 23 blaCMY-42 was the most prevalent blaCMY variant identified in this study (6/9), and to our knowledge, this is the first report of blaCMY-42 in Egypt. Moreover, for the first time in Egypt, we identified blaCMY-6 and the new blaCMY-72-like variant.
Integrons are often embedded in transferable genetic elements such as plasmids and transposons, which facilitate their lateral transfer into a wide range of pathogens, and therefore play a central role in the worldwide dissemination of antibiotic resistance because they can capture and express diverse resistance genes.10,11 Despite this, few studies have investigated the prevalence of integrons in clinical Gram-negative bacteria from Egyptian hospitals. 12 Our study demonstrated that, 50.8% of the bacterial isolates harbored at least one integron, which is in accordance with previous studies in different countries.12,24,25 However, a low integron prevalence rate of 31.7% was reported in Palestine. 26 Such variation can be attributed to diverse geographical distribution or differences in antimicrobial therapy schemes.
In this study, highly variable gene cassette profiles were identified for class 1 integrons conferring resistance to nearly every major class of antibiotics, with exception of the quinolones, which is in agreement with previous studies.12,27,28 dfrA and aadA gene cassettes were the most common, as seen in previous studies.12,26–28 The high prevalence of both gene cassettes may be owing to the wide use of trimethoprim, streptomycin, and spectinomycin in the treatment of clinical Gram-negative bacteria. 12 Moreover, in this study, we identified the aminoglycoside resistance genes (aadB, aac(3)-Id). The extensive use of aminoglycoside in Egyptian hospitals 12 may act as a selective pressure for the development of such determinants.
Chloramphenicol resistance gene cassettes (catB3) were detected in one P. aeruginosa isolate. Recently, these gene cassettes were identified from Enterobacter cloacae and Acinetobacter spp. in China,29,30 and from P. aeruginosa in Taiwan. 31 The low prevalence of chloramphenicol resistance gene cassettes may be because of the limited use of chloramphenicol in hospitals, owing to complications that can arise from its use. 12 We identified three β-lactamase gene cassettes (two blaOXA-10 and one blaVIM-2) within two different unique class 1 integrons in P. aeruginosa, (blaVIM-2-blaOXA-10-aadA1 and aadB-catB3-blaOXA-10). To our knowledge, this is the first report to identify such unique gene cassette profiles in class 1 integrons. Interestingly, blaOXA-10 and blaVIM-2 were previously identified in P. aeruginosa in Egypt, either co-occurring in the same bacterial isolates or blaOXA-10 occurring alone. 15 On the basis of these findings, we speculated that these integrons are responsible for the dissemination of blaOXA-10 and blaVIM-2 within P. aeruginosa in Egypt.
Class 2 integrons have been reported less frequently than class 1 integrons in Gram-negative bacteria and are associated with the Tn7 transposon. 26 Class 2 integrons were detected in 3 isolates, compared with 64 isolates harboring class 1 integrons. We identified the classical gene cassette profile, dfrA1-sat2-aadA1, in two bacterial isolates, while one P. stuartii isolate harbored a unique gene cassette profile of linF-dfrA1-aadA1. To our knowledge, this is the first identification of this integron in Egypt. In fact, this is only the second report of this integron, after its identification in Proteus vulgaris in China (GenBank accession number HQ386831).
Plasmid-mediated quinolone resistance associated with qnrA, qnrB, and qnrS has gained great interest because these resistance determinants are potentially spread among bacteria by plasmid mobility. 32 These genes are responsible for quinolone resistance by encoding a protein of the pentapeptide repeat family, which blocks the action of ciprofloxacin on purified DNA gyrase and topoisomerase IV. 32 Interestingly, 58.7% of the isolates harbored at least one qnr gene, which is a much higher prevalence than in developed countries. For instance, qnr genes were detected in only 1.63% of nalidixic acid-resistant E. coli isolates in Denmark, 33 in 1.6% of ESBL-producing E. coli and Klebsiella spp. in France, 34 and in only about 1% of ciprofloxacin- and/or tobramycin-resistant E. coli and Klebsiella spp. in Canada. 35 Moreover, our results are higher than that discovered in African countries, including Egypt, where 26.6% of ESBL-producing E. coli clinical isolates harbored qnr genes, 13 and Tunisia, where 25.8% of ESBL-producing Enterobacteriaceae harbored qnr genes. 36
Interestingly, unlike most previous reports,13,30,34 a high prevalence of qnrS over qnrB was detected in this study. However, a low level of qnrA was detected in this study, which is in agreement with most previous surveillance studies.10,32,36 The prevalence of ESBLs, AmpC β-lactamases, and qnr genes detected in this study may be explained by the excessive and unwise use of β-lactams and fluoroquinolones in the treatment of clinical Gram-negative bacteria.
The finding presented in this study declares the limited value of using conventional antimicrobials for the treatment of bacterial infections in Egypt. Unfortunately, this problem is exacerbated with the dramatic decline in the development of new antimicrobial agents over the past 30 years. 37 Therefore, there is an urgent demand for developing new strategies, for combating microbial infection to prevent the return to preantibiotic era. Although new strategies have been developed for the treatment of bacterial infections, such as immunoglobulins, antimicrobial peptides, bacteriophage, and prebiotics, few will produce promising effective products within the near future. 38 The prudent use of conventional antimicrobials in clinical setting in Egypt as well as other developing countries may have a significant value to overcome this problem.
In summary, this study confirms the high prevalence of different antimicrobial resistance mechanisms in Egypt. Furthermore, we identified various antimicrobial resistance genes in Egypt for the first time. The high prevalence of multiple antimicrobial resistance genes in bacterial isolates is extremely concerning because therapeutic options become very limited and high mortality rates will be associated with bacterial infections. Our study highlights the importance of the reasonable use of antimicrobials in treatment of bacterial infections and the need to develop new antimicrobial agents to combat MDR bacteria. Moreover, a more widespread surveillance, strict antibiotic supervision, and effective infection control measures are urgently needed to control this problem.
Footnotes
Acknowledgments
H.O.K is supported by postdoctoral fellowship from Egypt-Japan Education Partnership (EJEP). A.M.S. was supported by a doctoral fellowship from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (Fellowship no. 153532).
Disclosure Statement
No competing financial interests exist.