
Abstract
Purpose:
To investigate the differences in parental knowledge, attitudes, and practice about antibiotic use and resistance among the urban and rural populations in Croatia.
Materials and Methods:
A cross-sectional study based on a structured questionnaire was distributed to 1,000 parents of children attending 11 elementary schools of Primorsko-Goranska County in 2017.
Results:
The overall response rate was 65.1% (651/1,000)—50.6% (253/500) in urban and 79.6% (398/500) in rural population. Urban parents had a higher overall knowledge about antibiotics (p < 0.001), while urban and rural parents held mostly similar knowledge and attitudes related to antibiotic use when split into individual statements (p > 0.05). Age, education, income, work, and family member working in a health-related field were significantly related with the overall knowledge about antibiotics. In the previous year, 28.2% of children and 28.9% of parents reported using an antibiotic. Croatian parents had a high level of trust in doctors' antibiotic-prescribing practices (96.3% reported trusting the doctors' decision not to prescribe antibiotics, 93.5% to prescribe antibiotics) and high awareness of antimicrobial resistance (94.8%). The public's misconception regarding the terms “bacteria” and “virus” was found in 15.5% of parents. The source of information about antimicrobial resistance was television (60.4%), internet (57.1%), newspapers (44.2%), and medical professionals (30.9%).
Conclusions:
Although the knowledge about antibiotics was higher in urban parents, it was not reflected on the level of antibiotic consumption. There are indications that medical professionals should be more involved in communicating the problems of antibiotic use and resistance to patients.
Introduction
Antimicrobial resistance is at the top of the list of global threats to public health. 1 During the last several years, there has been a Europe-wide increase in antimicrobial resistance. 2 Extreme differences in attitudes, beliefs, and knowledge concerning antibiotic use and self-medication have been recorded in European countries. The level of misconceptions contributing to inappropriate antibiotic consumption was the highest in southern and eastern countries.3,4 The irrational antibiotic use is certainly a complex and multifactorial problem, but also one of the major drivers for the emergence and spread of antimicrobial resistance in the community.5–8
Since 2006, the Croatian Intersectoral Coordination Mechanism for the Control of Antimicrobial Resistance (Interdisciplinarna sekcija za kontrolu rezistencije na antibiotike [ISKRA]) has coordinated all activities related to antibiotic control on a national level. ISKRA has designed and distributed educational materials to the general public, national guidelines to physicians on antimicrobial therapy for the most frequent indications, but despite all efforts on the local and national levels (educational campaigns, posters, informative flyers, messages broadcasted on television, internet and other mass media, etc.), Croatia still belongs to the group of European countries with a high overall antibiotic use and consequently high antimicrobial resistance in the community.9–12 Parental pressure and expectations is often cited as one of the key drivers for antibiotic prescribing.13–16
The aims of this study were to investigate the differences in parental knowledge, attitudes, and practice (KAP) about antibiotic use and resistance among the urban and rural populations and to raise awareness about the need for more prudent antibiotic use in the outpatient setting.
Materials and Methods
The study was conducted in one county of Croatia, the Primorsko-Goranska County (P-GC), that consists of three well-defined entities: coastal area with hinterland, including the city of Rijeka (about 34% of the area), islands (about 29% of the area), and Gorski kotar (about 37% of the area). According to the Croatian Bureau of Statistics—Census of Population, Households and Dwellings in the Republic of Croatia in 2011—the total population of P-GC is 296.195 inhabitants. 17 A school-based stratified geographical clustering sampling was used to select a representative sample of children attending the fifth to the eight grade of elementary schools, whose parents (legal representatives or guardians) were asked to fill in a questionnaire after explaining the importance of the topic and their cooperation to the study through a letter. The total number of children attending the fifth to the eight grade of elementary schools in P-GC in 2016 was 9,275, according to the data of the Department of School and University Medicine, Teaching Institute of Public Health of P-GC (Rijeka, Croatia). The sample size was determined using the Raosoft Sample Size Calculator with confidence interval of 95% and a margin of error of 5%. It was estimated that a minimum sample size should include 369 respondents. 18 Assuming a response rate of 50% and anticipating good-quality data, the number of parents enrolled in the study was rounded to 1,000 (500 urban and 500 rural) having children aged between 10 and 16 years. From May 15 to June 14, 2017, a cross-sectional study based on a structured questionnaire was carried out in 11 elementary schools in P-GC. The schools were selected from a number of different venues in P-GC to increase the generalizability of the findings (Fig. 1). A KAP questionnaire regarding the use of antibiotics was developed and distributed (by children) to Croatian parents. Parental participation was voluntary, anonymous, and without compensation. The researchers assured that anonymity would be maintained and ethical principles would be followed. The returning of a completed questionnaire was considered as consent for participation. All the participating schools were contacted several times (personally, by phone) during the study period.

Number of respondents (response rate) per study site.
A 43-point self-administered questionnaire, composed of five parts, was used (Supplementary Data). The questionnaire was developed after a literature review of comparable studies. 1 Most of the questions about antibiotics were copied from other similar questionnaires used in scientific papers (questions 11–26, 29–31, 34, 35, 38–43),19–21 while the rest of the questions originated from our scientific team (questions 27, 28, 32, 33, 36, 37). To assure clarity, accuracy, and consistency of the questions, the questionnaire was pretested among a group of 50 parents. The first part of the questionnaire explored sociodemographic characteristics of parents: age, gender, residence, educational level, monthly family income, working in a health-related field, and at least one family member working in a health-related field. Children's age, gender, and school grade were also recorded. The questionnaire also investigated the frequency of antibiotic use by parents and children in the last year (according to the one parent–one child principle), parental knowledge about antibiotics, awareness about antimicrobial resistance, and attitudes and behavior regarding antibiotic consumption. The response alternatives were: written answers, dichotomous answers (yes/no), multiple choice, filter questions, and a 5-point Likert scale (strongly disagree, disagree, no opinion/neutral, agree, strongly agree). The overall median knowledge of the respondents about antibiotics was estimated by the sum of points (min. 8–max. 40) achieved on a Likert scale. The threshold for the score was fixed according to the range (8–40). A score of 8–13 points was interpreted as insufficient knowledge; between 14 and 20 as sufficient; between 21 and 27 as good; between 28 and 34 as very good; and ≥35–40 as excellent.
All statistical analyses were performed using the statistical packages Statistica13.1 (StatSoft, Inc., Tulsa, OK) and MedCalc12.1.3 (MedCalc Software, MariaKerke, Belgium). Data were presented as frequencies (absolute, relative), median, and percentiles (5th and 95th). Age was presented as a median with minimum and maximum values. For categorical variables, chi-square test was calculated. Kruskall–Wallis test with post hoc analysis was used to analyze the data. To assess the normal distribution of the variables, we used the Kolmogorov–Smirnov test. Mann–Whitney U test for independent variables was used to examine the differences between urban and rural participants. Data were presented with box and whisker plots. Correlations between attitudes, knowledge, and antibiotic use were calculated with Spearman correlation coefficient. Multiple regression analysis was used to identify the factors associated with the overall knowledge about antibiotics. p-Values <0.05 were considered statistically significant.
Results
The response rate in our study was 65.1% (50.6% for urban and 79.6% for rural population). The city of Rijeka, mountainous region of Gorski kotar, and four islands (Krk, Cres, Mali Lošinj, and Rab) were, respectively, targeted by 38.9% (253/651), 23.5% (153/651), and 37.6% (245/651) of respondents (Fig. 1). The study population included 651 parents—101 (15.5%) males and 550 (84.5%) females. Median age for all responders was 41 (range 29–61 years, 44 [min. 31–max. 54] for males and 41 [min. 29–max. 61] for females). Median age for urban participants was 42 (min. 31–max. 61) and 41 (min. 29–max. 59) for rural. The rural population had a higher response rate (χ2 = 58.78, p < 0.001). The urban population earned a significantly higher salaries compared to the rural population. Also, urban parents were more frequently employed in a health-related field compared with rural parents (p < 0.001). Other sociodemographic data of the participants are presented in Table 1. All the respondents (N = 651) answered all the requested questions.
Demographic Characteristics of the Study Population
Statistically significant.
Average salary in March 2017 was 6.022 HRK ( = 813.7 EUR; 1 EUR = 7.40 HRK, Croatian kuna).
Of all the respondents, 28.9% claimed to have used antimicrobial drugs in the last year. Of the school children, 28.2% have taken antibiotics in the last year. There was no significant difference between urban and rural populations; neither did age, gender, education, income, participant or family member working in a health-related field, and knowledge about antibiotics show any difference.
The overall median knowledge score about antibiotics was 32, representing very good knowledge. The urban population had statistically significant more overall knowledge about antibiotics compared with the rural population (median 33 [min. 24–max. 39] vs. 32 [min. 18–max. 39]; p < 0.001). The lowest value of knowledge about antibiotics was 18, interpreted as sufficient knowledge about antibiotics, while the highest value was 39, representing excellent knowledge about antibiotics (Fig. 2). Multiple regression was made on a sample of 651 respondents; the coefficient of multiple regression was R = 0.39 and the coefficient of determination was 15% (R2 = 0.15, p < 0.001). The regression model presented in Table 2 shows age, education, income, working in a health-related field (health care worker [HCW]), and one family member working in health care to be significantly related with the overall knowledge about antibiotics. Younger parents from the urban environment had greater knowledge compared with rural parents, while parental knowledge about antibiotics in the rural area was better among older parents. Urban and rural populations showed a relatively high, similar knowledge level about antibiotic use in individual statements (p > 0.05). Of all the respondents, 89.4% knew that “antibiotics are useful for the treatment of bacterial infections,” but of these, 15.5% also agreed that “antibiotics are useful for the treatment of viral infections” (Table 3).
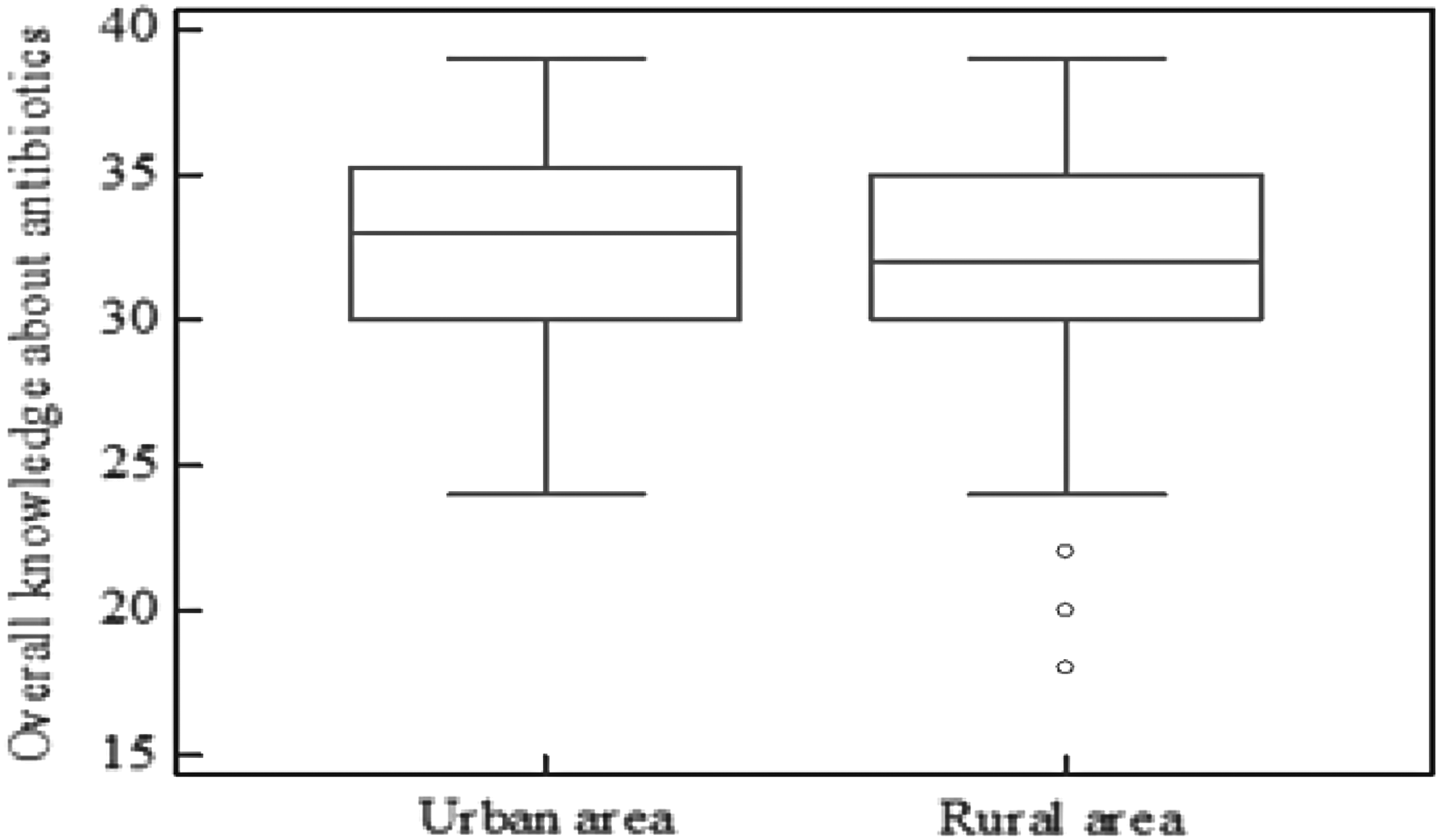
Parental overall knowledge about antibiotics (urban vs. rural) represented with median, 25th and 75th percentiles, and minimum and maximum.
Factors Significantly Related to the Overall Knowledge About Antibiotics
β, coefficient of regression; HCW, health care worker; SE β , standard error of β coefficient.
Knowledge About Antibiotics
The “agree” response represents the sum of percentages of “agree” and “strongly agree.” The “disagree” response represents the sum of percentages of “disagree” and “strongly disagree.”
93% versus 97% might be statistically significantly different, but in practice these are both >90%.
Most parents (91.9%) heard about antimicrobial resistance. Of all the respondents, 80% considered that antimicrobial resistance is a global problem, but only 63.9% thought it is a problem on a national level. There was no significant difference between urban and rural respondents, all p > 0.05. Television (60.4%) was the main source of information about antimicrobial resistance, followed by internet (57.1%), newspapers (44.2%); only 30.9% of the respondents learned about antimicrobial resistance from a general practitioner, a family medicine practitioner, or a pediatrician (more than one answer was possible). There was no significant difference by area, all p > 0.05. Of all the respondents, 9.2% received information about antimicrobial resistance from other sources (friends, family members, neighbors, schooling, professional literature, professional lectures, promotional actions about antibiotics), which was significantly different between the urban and rural parents (urban 13% vs. rural 7%; p < 0.015). Of all the respondents, 94.8% were aware that excessive use of antibiotics can lead to increased bacterial resistance to antibiotics, with no significant difference between the urban and rural populations (p > 0.05). The overall median knowledge score about excessive use of antibiotics and development of bacterial resistance was 5, representing excellent knowledge (min. 1–max. 5).
Most parents (96.3%) expressed confidence in doctors deciding not to prescribe antibiotics, while 93.5% expressed confidence in doctors deciding to prescribe antibiotics. The majority of participants (73.1%) have taken the full dose of the antibiotics prescribed, but some claimed to have stopped taking antibiotics due to symptom relief (8.9%) and due to their own wish (18%). There was no significant difference between the urban and rural populations, all p > 0.05.
Almost all participants (99.1%) reported they did not use an antibiotic for themselves or their child without physician prescription in the last year. Less than 1% of parents stated they had acquired an antibiotic without a prescription or used leftover antibiotics from previous treatments. There was no significant difference between the urban and rural respondents (p > 0.05). A large majority (97.8%) reported taking antibiotics only when prescribed by a doctor. However, 6.1% of participants wanted to buy an antibiotic from a pharmacist without physician prescription. Of all the parents, 9.1% saved leftover antibiotics because these might be useful in the future. There was no significant difference by the area, all p > 0.05.
Of all the participants, 82.3% stated they would never use an antibiotic for themselves without consulting a doctor. The most common indications for intended self-medication were toothache (11.2%), followed by earache (6.9%), sore throat (6.5%), fever (2.9%), and cold (2.2%); more than one answer was possible. Also, 93.7% of all parents would not give an antibiotic to their child without consultation with a doctor. Toothache (2.6%) was the main condition for intended antibiotic use, followed by earache (2.5%), sore throat (2.5%), fever (2.3%), and cold (0.8%); more than one answer was possible. There was no significant difference between the participants, all p > 0.05. The urban and rural populations showed similar attitudes related to antibiotic use in most individual statements (p > 0.05). A significant difference between urban and rural parents was noted only for the statement “pharmacists often tell you how to take antibiotic” (p = 0.040) (Table 4).
Attitudes Regarding the Consumption of Antibiotics
The “agree” response represents the sum of percentages of “agree” and “strongly agree.” The “disagree” response represents the sum of percentages of “disagree” and “strongly disagree.”
Statistically significant.
Discussion
The results of the present study showed that the frequency of antibiotic use in the previous year in P-GC (28.9% parents and 28.2% children) was lower than the Croatian (36%) and European average (34%), according to the Special Eurobarometer Report in 2016. Our results still indicate a higher use than in Germany (23%), the Netherlands (20%), and Sweden (18%), but much lower than in Malta (48%), Spain (47%), and Italy (43%). 22 Interestingly, although there was a difference between urban and rural populations in the overall knowledge about antibiotics related to age, education, income, working in a health-related field, and one family member working in health care, there was no difference in the frequency of antibiotic use related to these categories. The reasons for lower antibiotic consumption in P-GC compared to the Croatian average are complex but could, at least partially, be due to the enforced national guidelines on antibiotic use and awareness campaigns by HCWs.23,24
Mothers represented 84.5% of our respondents, which is probably a reflection of their higher involvement in raising family in our society. We obtained a higher response rate from rural areas, which was probably due to the fact that people in these areas spend more time for each other and show more commitment to community wellbeing. Some studies have reported that patients' expectations influence doctors' prescribing practices.13–16 In our study, the trust in doctors prescribing antibiotics was higher than in two Swedish studies.21,25 Also a Greek study has demonstrated that parents do not pressurize physicians to prescribe antibiotics. 26 As suggested by a Swedish study, 21 doctors themselves may be an important target for improving rational antibiotic consumption. Notably in our study, <1% of parents confirmed self-medication with antibiotics in the last year, which is similar to the Swedish restrictive behavior toward self-medication.21,27 In comparison, self-medication in Denmark (3%) and Greece (44.6%) was higher than in our study.28,29 Specifically for the pediatric population, Greek authors showed that 10% of parents administered antibiotics to their children without medical advice. 26 Although the reported rate of self-medication was low, the intended use of antibiotics for themselves (17.7%) or their children (6.3%) was high, but still lower than in the United States (25.4%). In our study, 8.9% of participants didn't understand the need to complete the prescribed dose of antibiotics, and 9.1% of respondents saved leftover antibiotics for future consumption, in comparison to 6.1% of Swedish and 14.2% of American citizens.25,30 The most common indications for intended use were toothache, earache, and sore throat. Intended self-medication and storage of antibiotics are strong predictors of actual self-medication.3,30 The level of knowledge about antibiotics varies by countries. The proportion of respondents who knew that antibiotics are not meant to kill viruses was the highest in Sweden (72%) and the Netherlands (62%) and the lowest in Spain (37%) and Italy (28%), while Croatian findings (44%) were close to the European average (43%). 22 The high rate of positive responses to this question may be due to the public campaigns on antibiotic awareness that are especially active in this region of the country. 10
Awareness regarding bacterial resistance is generally higher in Scandinavia than in southeastern European countries.21,25,31 Responders in our study perceived antimicrobial resistance to be more of a global (80%) than a national (63.9%) problem.
In our study, the role of pharmacists in providing information about appropriate antibiotic treatment seems to be higher than in Sweden and Italy, and higher than the Croatian and European average. On the contrary, the role of medical professionals in promoting awareness about bacterial resistance to antibiotics is similar to the European but lower than the Croatian average.22,31
There are several limitations in our study. Due to logistical reasons, it was not possible to conduct telephone or internet interviews. As questionnaires were answered at home, there was a possibility that parents searched for answers on the internet or took guidance from other people around them. Also they did not have the opportunity to ask for clarification regarding unclear questions. Another limitation was that parents who participated were more interested in the subject, thus leading to a potential overestimation of KAP about antibiotic use and resistance. The finding that a higher percentage of urban parents were employed in a health-related field may have biased the interpretation of results. Although it is not appropriate to generalize our findings to the whole parental population in Croatia, these results are useful for streamlining the activities of national public health campaigns.
Of all the respondents, 37.5% stated that doctors do not explain how and why an antibiotic should be taken. The main reason for that is the lack of time for communication due to overcrowding in most primary care offices. Public campaign materials and communication tools available at the European Centre for Disease Prevention and Control (ECDC) and World Health Organization (WHO) antibiotic awareness campaign website may be helpful in educating patients. In Croatia, educational posters, flyers, and a picture book promoting care without antibiotics for upper respiratory tract infections are available, but still not widely in use. In conclusion, although the knowledge about antibiotics is higher among urban parents, it is not reflected on the level of antibiotic consumption. According to our study, there are indications that medical professionals should be more involved in communicating the problems of antibiotic use and microbial resistance to patients.
Footnotes
Acknowledgments
The authors would like to thank all the children and their parents (legal representatives or guardians) who agreed to participate in the survey. The authors are additionally grateful to the directors, pedagogues, and teachers of the schools that participated in the study for their time and cooperation. The authors extend special thanks to Đ. Malatestinić and Ž. Sesar for help with comments, N. Dragaš-Zubalj for help in contacting the schools, and T. Čulina for taking part in data collection. This research was supported in part by the Teaching Institute of Public Health of Primorsko-Goranska County, Rijeka, and also partially by M.F.
Ethical Approval
The study design and questionnaire were approved by the Ethics Committee of the Teaching Institute of Public Health of Primorsko-Goranska County in Rijeka and the Ethics Committee of the University of Split School of Medicine.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.