
Abstract
The Beijing family, the most successful Mycobacterium tuberculosis lineage, is considered hypervirulent, associated with clustering and has a strong association with multidrug-resistant tuberculosis. The Beijing strains have spread worldwide and also to Latin America. Genotyping of a countrywide collection of 380 M. tuberculosis strains from Ecuador, with 24-loci mycobacterial interspersed repetitive units-variable number tandem repeats (MIRU-VNTR), revealed only six Beijing strains, but four of these were MDR-TB. There was no clustering as all six strains had very distinct MIRU-VNTR profiles that have not been reported in the rest of Latin America. Although active transmission for Beijing has been described for the neighboring countries Peru and Colombia, there is no evidence that Beijing strains in Ecuador are more frequently transmitted than other strains. Moreover, the low prevalence (1.6%) of the Beijing sublineage in Ecuador challenges the concept of hyperadaptability and transmissibility of the Beijing strains in our country.
Introduction
Tuberculosis (TB) remains a major global health problem and one of the most important infectious diseases worldwide. According to the WHO, in the year 2017 an estimated 10.4 million people fell ill with TB and >1.5 million deaths caused by TB. 1
In a global effort to reduce the TB burden worldwide, molecular epidemiology approaches based on genotypic analysis of Mycobacterium tuberculosis (MTB) isolates have been developed to identify transmission clusters and routes for a better understanding of the dynamics of this pathogen 2 and for describing the global spread of TB. Genotyping results have revealed that MTB strains cluster into seven major lineages, each associated with a specific geographic location. In particular, the MTB Beijing genotype family, belonging to the East Asian lineage 2, has been significantly associated with major TB outbreaks for the past decade throughout the world.
This family is spreading worldwide, due to selective advantages compared with other MTB lineages, such as increased capacity to acquire drug resistance, an increased transmissibility, and hypervirulent features.3,4 The Beijing family emerged 6,600 years ago in northeast China, Korea, and Japan. Migration movement has expanded this strain around the world, with a prevalence ranging from >40% in East Asia to <10% in the Americas, and with an increasing prevalence from Central Asia toward Eastern Europe after the collapse of public health systems of the former Soviet Union countries.4,5 In all these regions, Beijing is strongly associated with drug resistance, especially multidrug resistance (MDR), that is, strains resistant to the anti-TB drugs isoniazid and rifampicin.3,5
Beijing strains have been reported in several countries in Latin America, with a prevalence of <5%6–9 in most countries with the exception of Peru and Colombia. In Peru, a prevalence as high as 16.4% has been reported in local studies and the presence of Beijing strains is strongly associated with MDR strains and with Chinese and Japanese migration to this country during the past century.10–14 In southeast Colombia, in the city of Buenaventura a study showed that the Beijing genotype represented 15.6% of the isolates and was correlated with multidrug-resistant tuberculosis and female sex of the patients. 15
Ecuador is a South American country that shares its land border with these two countries: with Colombia to the north and Peru to the east and south. The only documentation for the presence of the Beijing family in Ecuador is a single strain found in 2017 in a convenience sample of merely 28 M. tuberculosis isolates 16 and two strains found in a convenience sample of 104 MDR strains isolated in the years 2002–2014 in a single hospital in Quito. 17 Considering that Ecuador is a border country with Peru and Colombia, where high rates of Beijing lineage have been found, the aim of our study was to determine the prevalence of the Beijing family in the Ecuadorian population. For this study we used a countrywide collection of M. tuberculosis strains, isolated in the years 2014–2016.
Methods
MTB isolates
For this study we used 380 MTB strains isolated from pulmonary and extrapulmonary TB patients. The strains came from 23 of the 24 provinces of Ecuador and were randomly selected from the strain collection of 2,275 strains isolated in the years 2014–2016 at the Laboratorio de Referencia de Micobacterias from Instituto Nacional de Salud Publica e Investigación (INSPI) in Quito and Guayaquil (Fig. 1 and Table 1). The sample size was calculated using the Yamane formula for determining the sample size of a finite population. 18 This formula assumes a margin of error of 5% and a p of 0.5. The sample size for each of the 24 provinces was calculated proportional to the annual average of TB cases detected in each province of Ecuador in this 3-year period. One province (Carchi) was not represented in our sample because no M. tuberculosis isolates were available in the reference laboratory. Of the 380 isolates, 254 (67%) had a known drug susceptibility pattern; 126 were susceptible to all drugs tested, 57 were resistant to INH, 14 to RIF, and 67 were MDR strains (Table 2 and Supplementary Table S1).

Geographical distribution of MTB isolates included in this study. The 380 MTB isolates were located on the map of Ecuador according to the address provided by the patients. The two-letter codes used for the provinces are detailed in Table 1. Circle with arrow, top left, represents south-north orientation. The province Pichincha (Pi) includes Quito, the capital city (second largest city of Ecuador). The province Guayas (Gu) includes Guayaquil, the most populated city of the country with the highest TB prevalence. MTB, Mycobacterium tuberculosis.
Distribution of Mycobacterium tuberculosis Isolates Across the Provinces of Ecuador and Included in This Study
The provinces in this table are grouped in the three distinct geographical regions of Ecuador: the Costa (coast), Sierra (mountains), and Oriente (east). The two-letter codes used for the provinces can also be found in Figure 1. One MTB isolate, from the insular region the Galapagos Islands (GA), is not included in this table.
Drug Resistance Profiles of the Mycobacterium tuberculosis Isolates Included in This Study
For Drug Resistance Profiles of the Individual Isolates, See Supplementary Table S1)
DNA isolation
M. tuberculosis isolates were grown in Lowenstein Jensen medium and resuspended in Tris-HCl EDTA buffer (10 mM/1 mM) and inactivated by boiling at 95°C for 15 minutes. Inactivated samples were centrifuged for 5 minutes at 10,000 g and the supernatant was directly used for genotyping as previously has been reported 19 and without further DNA purification.
Beijing lineage identification and phylogenetic analysis
All strains were analyzed with 24-loci MIRU-VNTR typing 20 and lineages were assigned by comparing the MIRU-VNTR patterns with those in the MIRU-VNTR plus platforma.
For transmissibility analysis, the MIRU-VNTR data of the Beijing strains were analyzed against published MIRU-VNTR data available for Beijing strains from other countries in Latin America with the software packages available at MIRU-VNTR plus platform using the DSW (stepwise weighted distance) distance measures suggested for MIRU-VNTR data. 21
Results
Identification of Beijing strains
Based on their MIRU-VNTR pattern, six Beijing strains were identified in the strains collection of 380 MTB strains, which means a prevalence of 1.58%. Two strains, both susceptible for the two main TB drugs (isoniazid and rifampicin), were from the Andean region of Ecuador: one from Quito, the capital of the country, and another from the Azogues province. The other four Beijing strains were all MDR strains and came from the most populated city of the country, Guayaquil, which is in the southwest of Ecuador and near the border with Peru.
Population structure of the Beijing family from Ecuador
We analyzed the six Beijing genotypes, and included in this analysis five other Beijing strains from Ecuadorian patients with published MIRU-VNTR data and reported in scientific communications4,16,17 with the help of the MIRU-VNTR plus platform (www.miru-vntrplus.org/). MIRU-VNTR cluster analysis of the 11 strains showed that the strains from Ecuador are genetically diverse and do not form a homogeneous clonal complex (Fig. 2 and Supplementary Table S2). The four Beijing MDR strains from Guayaquil cluster into two related pairs that differ by at least 8 MIRU-VNTR loci. The five strains from the Andean region (two strains from our study and one strain from Jiménez et al., 16 all three strains susceptible to antimycobacterial drugs, and two MDR Beijing strains from Zurita et al. 17 ) have widely different MIRU-VNTR profiles (Fig. 2 and Supplementary Table S2). The two Ecuador strains reported by CDC Atlanta in Merker et al. 4 and isolated from Ecuadorian patients who had lived less than a year in the United States are clonal. However, in the publication only 23 of the 24 MIRU-VNTR loci are shown and no information is available on the drugs susceptibility pattern of these two strains and the region in Ecuador where these patients had lived before migrating to the United States.
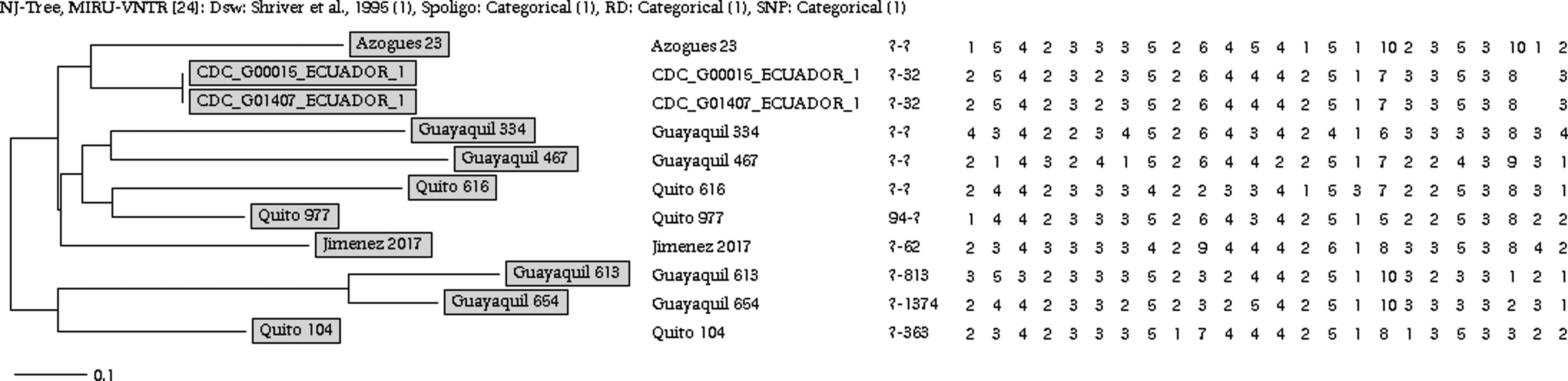
Neighbor joining tree and the 24-MIRU VNTR patterns of 11 Beijing strains from Ecuador. The strains 23, 104 (from this study), and Jiménez 2017 (from Jiménez et al. 16 ) are sensitive to all the first-line TB drugs. The strains “Guayaquil” (from this study) are all MDR strains. The strains Quito 616 (resistant to INH) and Quito 977 (a MDR strain) are both from Zurita et al. 17 The two strains “CDC” (from Merker et al. 4 ) have no information on drug sensitivity.
Comparison of the genotypes of the Beijing family from Ecuador with Beijing strains from other countries of Latin America
To determine the relationship between the Beijing isolates of Ecuador and Beijing strains from the rest of South America, a MIRU-based dendrogram and minimum spanning tree (MST) was drawn with the help of the MIRU-VNTR plus platform. This MST compared the 11 strains from Ecuador with Beijing strains reported from other countries in South America for which the MIRU-VNTR profiles were available; 8 Beijing strains from Brazil, 22 70 strains from Peru, 23 8 strains from Colombia, 24 8 strains from Venezuela, 4 and 1 strain from Bolivia. 4 We also included three strains isolated from Ecuadorian immigrants in Europe. 25 All 24 MIRU-VNTR patterns used for this MST analysis are detailed in Supplementary Table S2, and we show in Figure 3 that the Beijing strains from Latin America in general cluster in country-specific clonal complexes. However, this is not true for the 11 strains from Ecuador, which are genotypically more diverse than the strains from the other countries and cluster with three of the seven complexes: complexes 3, 4, and 7 (although 8 out of the 13, 62%, of Ecuadorian Beijing strains are linked with Brazilian genotypes). By contrast, the three strains isolated from Ecuadorian immigrants in Europe 25 cluster with Peruvian strains (Fig. 3).

MST analysis of the Beijing strains from Ecuador (red), Peru (blue), Colombia (brown), Bolivia (green), Brazil (yellow), and Venezuela (purple). The strains from Ecuador are described in this article and Merker et al., 4 Jiménez et al., 16 and Zurita et al. 17 The strains from Ecuadorian immigrants in Europe are described in Barletta et al. 12 The 24-loci MIRU-VNTR profile for all Beijing strains included in this MST analysis is detailed in Supplementary Table S2. MST, minimum spanning tree. Color images are available online.
Discussion
According to the World Health Organization, in 2016 the incidence of TB in Ecuador was 50 (33–72) cases per 100,000 inhabitants. 27 With a case detection rate of ∼60% and a prevalence rate of multidrug-resistant (MDR) TB of 7, 3% (5.4–9.2), Ecuador has an epidemiological environment that would be susceptible to the spread of highly virulent strains. In addition, the country has open borders with Peru and Colombia, where a high prevalence of expanding Beijing clusters have been reported.11,15
Although Beijing strains in general are associated with drug resistance, a recent report from Ecuador shows a low prevalence of 1.9% for Beijing strains in a collection of 104 MDR tuberculosis strains isolated in a single hospital in Quito in a period of 12 years. 17 In this study, we searched for Beijing strains in a statistically representative countrywide collection of Mycobacterium tuberculosis strains isolated in the years 2014–2016, and we also find a low prevalence of 1.6%. Similar findings of a low prevalence of Beijing strains also have been reported in South America for Brazil, Argentina, and Paraguay. 6 The Beijing strains of our study had a strong association with multidrug-resistant tuberculosis and four of the six strains were MDR strains. No indication for recent transmission of our Beijing strains was found, and the strains of our study are genotypically very diverse, belonging to different clonal complexes indicating several independent introductions of Beijing into the country and suggesting that Beijing strains are not more highly transmitted than other strains in Ecuador. How the Beijing strains were introduced into Ecuador is puzzling and we have not enough epidemiological information from the patients for further epidemiological analysis. The strain collection we used comes from the collection of the Tuberculosis Reference Laboratory of the Ministry of Public Health, and this laboratory is focused on diagnosis and drug susceptibility testing of TB. The only data collected with the strains are the name and surname of the patient and his/her residence. Because of the surname of the patients we presume that the strains were isolated from Ecuadorian patients with no Chinese background. Our MST analysis also shows that Peruvian Beijing strains have not spread across borders of Ecuador challenging the concept that all Beijing strains have an increased capacity for transmission and virulence compared with other strains of other lineages.3,5,22 However, 8 of the 13 Ecuadorian Beijing strains show similarity to Brazilian strains, despite the fact that there are no borders between both countries. This striking finding could be explained based on the different Beijing sublineage strains in Peru and Brazil, as it has been shown in a recent publication where an increased virulence and transmissibility for “modern Beijing sublineage” but not “ancient Beijing sublineage” is reported.28 Our MST analysis of the Beijing isolates from Ecuadorian migrants in Europe 25 shows that these strains are related to Beijing isolates from Peru (Fig. 3), suggesting that the infection of Ecuadorian immigrants could have happened in Europe and through contact with Peruvian immigrants, living in the same communities. However, this is speculation as epidemiological data are not available. To get a better insight into the epidemiology of the Beijing strains from Ecuador and to test the aforementioned hypotheses we have planned in the near future whole genome sequencing and single-nucleotide polymorphism (SNP) analysis of our strains to better characterize their genetic variations potentially associated with the lack of virulence and drug resistance. In addition, this will allow a further characterization of our strains as belonging to the modern/typical or ancestral/atypical sublineages and to study their evolutionary history.
Limitations of the study
The sample we analyzed is relatively small and we do not exclude the presence of other Beijing strains with the same MIRU-VNTR pattern as we have found in this study in the strain collection of 2,275 strains, indication transmission of Beijing strains in Ecuador. We have, therefore, planned to analyze in the future all 2,275 strains and use a simple specific marker, a Beijing-specific SNP, to screen for Beijing genotype in the rest of the strain collection.
Footnotes
Acknowledgments
We thank Dr. Washington Cárdenas from the Laboratorio para Investigaciones Biomédicas of the Escuela Superior Politécnica del Litoral (Guayaquil) for logistical support on this study. We also thank Nathaly Espinel for her dedication, working in the laboratory with MIRU typing at Dr Jeanette Zurita laboratory, and Dr. Howard Takiff for critically reading and editing the article. This study was partially financed by a Medical School Grant of University San Francisco de Quito. The ethics committee of the University San Francisco de Quito approved this investigation with code number 2017-023IN.
Authors' Contributions
All authors participated equally in study design, data analysis, and interpretation. D.G.C., M.A.G.B., and J.H.d.W. wrote the article.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.