
Abstract
Introduction:
Carbapenem-resistant Acinetobacter baumannii (CRAB) is recognized to be among the most difficult antimicrobial-resistant gram-negative bacilli to control and treat. An understanding of the epidemiology of CRAB and the mechanisms of resistance to carbapenems is necessary to develop strategies to curtail their spread.
Methods:
Electronic databases were searched from January 1995 to December 2017 for all studies, which: (1) provide data on the frequency and antibiotic resistance profile of the isolated A. baumannii and (2) describe the mechanisms of carbapenem resistance in detail.
Results:
Sixty-eight studies were found referring to mechanisms of carbapenem resistance in clinical isolates of A. baumannii, and 56 studies were found referring to the frequency of CRAB. The pooled frequency of carbapenem resistance was 85.1% (95% confidence interval [CI]: 82.2–88.1) in 8,067 clinical isolates of A. baumannii. Resistances due to blaOXA23 (55.3%), blaOXA24 (41.4%), and blaOXA58 (5.2%) genes were the most prevalent reported mechanisms of resistance to carbapenem, respectively.
Conclusions:
Our data warn that CRAB will rise if the current situation remains uncontrolled. Better control infection strategies and antibiotic managements, particularly in the health care systems, are needed to limit the spread of this pathogen.
Introduction
A
One of the most common mechanisms of carbapenem resistance is the production of carbapenem-hydrolyzing enzymes (carbapenemases).5,6 These enzymes belong to classes A, B, and D based on molecular Ambler classification.5,6 Class A carbapenemases consist of six different members (SME, IMI, NMC, GES, SFC, and KPC families) (13). Of these, GES carbapenemases are the most prevalent in A. baumannii, which confer a low level of resistance to carbapenems.5,6 These carbapenemases are more common in Enterobacteriaceae than A. baumannii. 10 Class B enzymes called metallo-β-lactamases (MBLs) are potent carbapenemases and four types of MBLs have also been reported in A. baumannii, namely IMP, VIM, SIM, and NDM.5,11 Carbapenem-hydrolyzing class D β-lactamases (CHDLs), also referred to as OXA-type enzymes or oxacillinases, are the most common carbapenemases in A. baumannii. 5
Currently, six subclasses of OXA related to A. baumannii have been identified (i) OXA-23-like (OXA-23, OXA-27, OXA-49, and OXA-239), (ii) OXA-24-like (OXA-24, OXA-25, OXA-26, OXA-40, and OXA-72), (iii) OXA-51-like, (iv) OXA-58, (v) OXA-143-like (OXA-143 and OXA-231), and (vi) OXA-235-like (OXA-235, OXA-236, and OXA-237).5,6
The second major mechanism of resistance is loss and/or decrease in outer membrane proteins (OMPs), which leads to a reduction in the permeability of antibiotics.5,6 Three OMPs (a 29-kDa protein [also known as CarO], a 33- to 36-kDa protein, and OmpW) have been identified in A. baumannii.5,6 Finally, overexpression of resistance-nodulation-cell division (RND)-type efflux pumps such as AdeABC, AdeFGH, and AdeIJK plays a significant role in carbapenem resistance.5,6 Iran is a country with the highest rates of CRAB, reaching 92% for imipenem and meropenem. 12
In Iran, several studies reported the CRAB13–16 ; however, a comprehensive study on the prevalence as well as the mechanisms of CRAB has not yet been performed. Therefore, the aims of this study were: to determine the frequency of carbapenem resistance among clinical isolates of A. baumannii and to understand the mechanisms responsible for the emergence of carbapenem resistance in this bacterium.
Methods
Search strategies and study selection
A comprehensive search in PubMed, Web of Science, Scopus, and Iranian databases [i.e., MAGIRAN (www.magiran.com) and SID (www.sid.ir)] was performed from January 1995 to December 2017 for all articles that included the search terms “acinetobacter” AND “Carbapenem*” OR “imipenem” OR “panipenem” OR “Doripenem” OR “Meropenem” OR “Biapenem” OR “Tebipenem” AND “Iran” in their title and/or abstract. Similar strategies and related Persian keywords were used for Iranian databases. The study focused on original articles that were published in English and Persian. Two reviewers (A.F.S. and M.A.) independently performed systematic search, study selection, and data extraction from included studies. Any discrepancies were resolved through consensus discussion.
Inclusion and exclusion criteria
Studies that provided data on the antibiotic resistance in clinical isolates of A. baumannii and/or described the mechanisms of carbapenem resistance in detail were selected. Studies were included if resistance was determined according to Clinical and Laboratory Standards Institute (CLSI) Guideline. Review articles, congress abstracts, studies with languages other than English or Persian, case reports, and editorials were excluded.
Data extraction
For each study, the following information was extracted: author's name, published year, study period, study design, sample size, type of infection, sites of infection, number of A. baumannii tested, proportion of carbapenem resistance, the method of diagnosis of carbapenem resistance, and the mechanisms of carbapenem resistance.
Quantitative data synthesis
The pooled prevalence of CRAB, with 95% confidence intervals (95%CI) was calculated by the random-effects model. The I2 test was used to assess between-study heterogeneity, where I2 values of 0% indicate no observed heterogeneity whereas larger values indicate increasing heterogeneity. Egger's and Begg's tests were used to check the publication bias (p < 0.05 was considered indicative of statistically significant publication bias). All the analyses were conducted by using Stata 14.0 (StataCorp, College Station, TX).
Quality assessment of studies
The checklist provided by the Joanna Briggs Institute was used to perform the quality assessment. 17
Results
Figure 1 shows the steps that we followed to select the relevant studies. We initially identified 1,000 potentially relevant studies from databases. In the end, there were 88 studies fulfilling the inclusion criteria. Table 1 summarizes the characteristics of each included study. The total number of A. baumannii isolates included in the study was 7,938. All studies exclusively examined the mechanisms of carbapenem resistance in A. baumannii. Disk diffusion, Microbroth dilution, E test, Modified Hodge test, and Multiplex PCR were the methods used in the included studies.
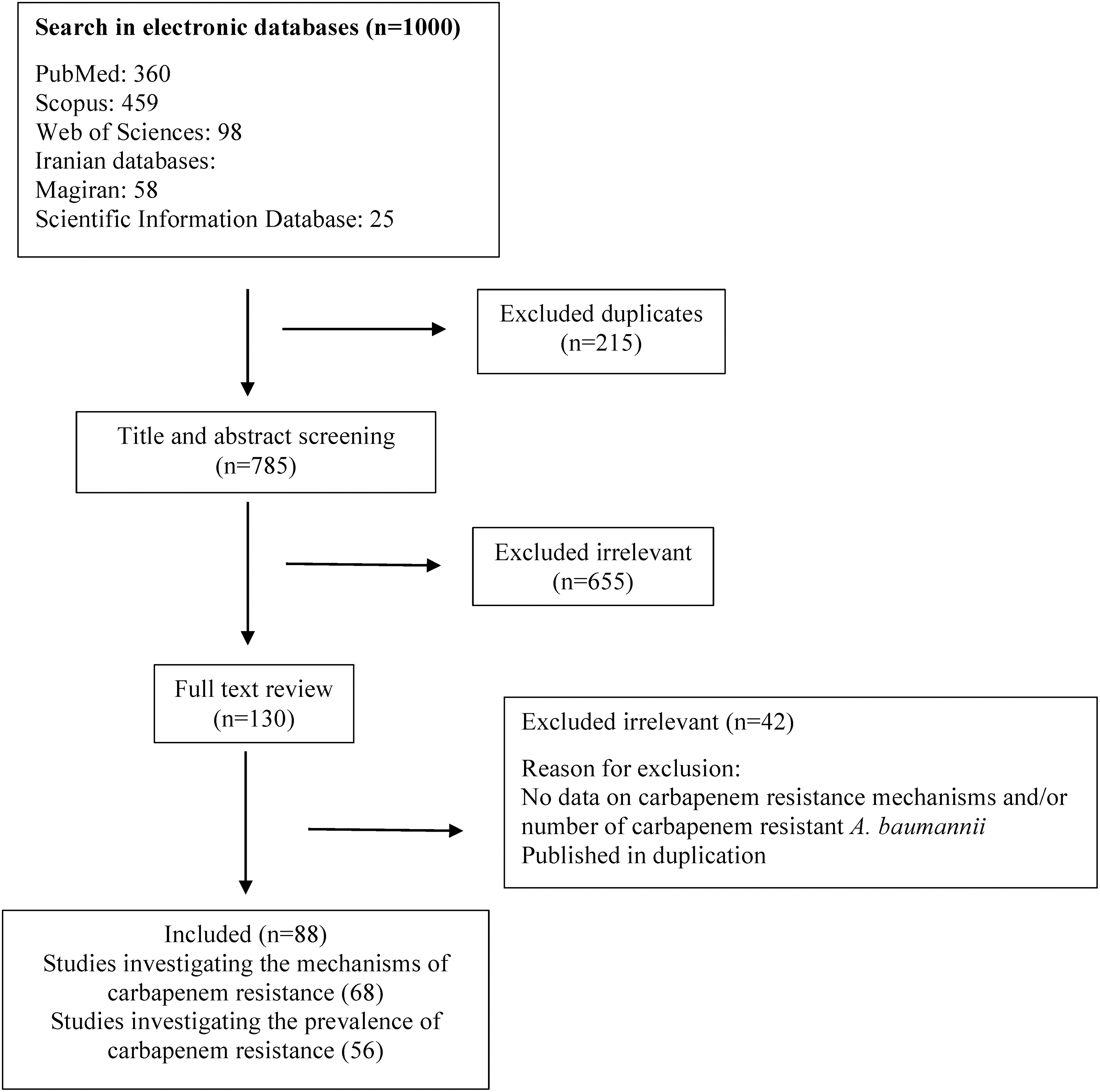
Flowchart of study selection for inclusion in the systematic review and meta-analysis.
Characteristics of Included Studies
All included studies were cross-sectional studies, among which 10 studies examined patients with burn wounds, three studies examined pneumonia, and the other studies examined all sources of infections. Studies were mostly conducted in the center and capital of Iran (50 in Tehran, 5 in Isfahan, 5 in Kashan, 5 in Shiraz, 3 in Kerman, 2 in Arak, and 1 in Qom).
Prevalence of carbapenem resistance in clinical isolates of A. baumannii
Based on the quality assessment, 56 studies were included for quantitative analysis. In these studies, the reported resistance to carbapenem varied across studies, ranging from 26.6% to 100%. The pooled frequency of carbapenem resistance in clinical isolates of A. baumannii was 85.1% (95%CI: 82.2–88.1; I2 = 100%) (Fig. 2). Based on Begg's (p = 0.00) and Egger's (p = 0.01) tests, there was some evidence of publication bias.
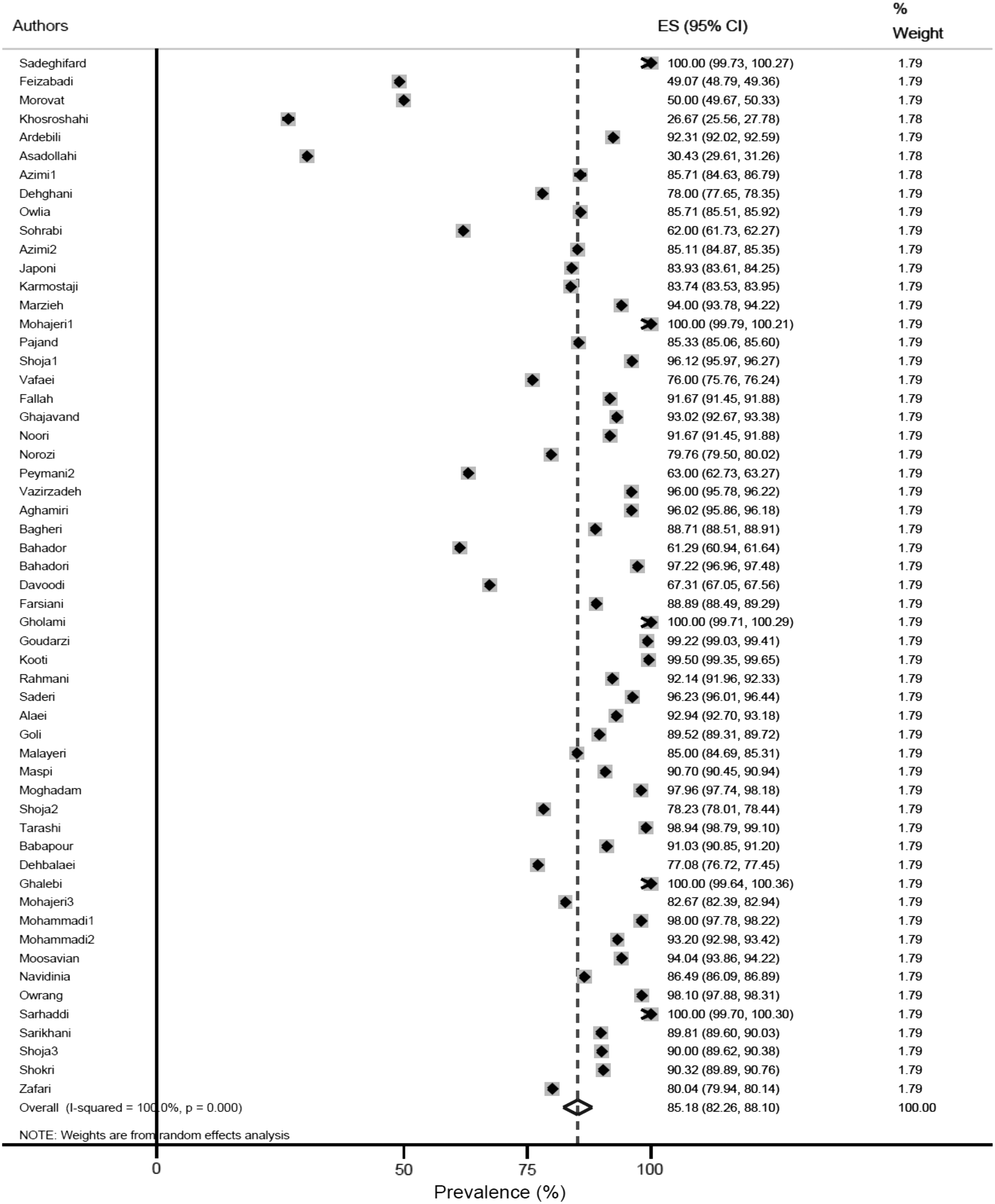
Forest plot of frequency of carbapenem resistance in clinical isolates of Acinetobacter baumannii.
Mechanisms of carbapenem resistance in clinical isolates of A. baumannii
Sixty-eight studies fulfill the criteria for this section. Resistance due to the blaOXA23 gene has been reported in 44 papers. Analysis of these studies revealed that 55.39% (2,489/4,493) of resistant A. baumannii strains possessed blaOXA23 gene. Therefore, blaOXA23 was the most common gene responsible for resistance to carbapenem among A. baumannii strains. Table 2 showed the other prevalent genes that were responsible for resistance to carbapenem.
Mechanisms of Carbapenem Resistance in Clinical Isolates of Acinetobacter baumannii
Discussion
The emergence and spread of CRAB, occurring in the outbreak of health care associated infections, is a concerning public health crisis, especially in the ICU setting. The presence of CRAB could be sufficient to consider this bacteria as highly resistant.18,19 A. baumannii isolates from different countries have shown resistance to carbapenems in a wide range; especially in developing countries, the occurrence of CRAB infections has become an emergent public health concern in nosocomial infections. 20 In Iran, the prevalence of CRAB has been increasing rapidly during the past years, which influences emerging multi-drug resistance.13,21
According to this analysis, the high rate of resistance to carbapenem (85.1%) was assessed. The CRAB that was reported by different studies ranged from 26.6% to 100%. This level of resistance is higher than previous reports of resistance to imipenem from Iran.13,21 Increasing the resistance to carbapenems, which were considered the choice of treatment for A. baumannii infections, has created obstacles for the effective treatment of these infections. In addition, rapid expansion of the CRAB infection could be principally because of the dissemination of established resistant clones or the acquisition of resistance elements by susceptible strains. Although the main reason is not obvious, some studies support the second reason.21–24 The neighboring countries of Iran, including Pakistan, Turkey, Afghanistan, and Iraq, have particularly high rates of CRAB.25–28 The trends of these countries also were increasing, for example, in Turkey, resistance to carbapenems reached 97.8% in 2015. 29 Also, some evidences about community-acquired Multi-Drug Resistant A. baumannii infections have been reported from Afghanistan and Iraq through the past decade. 30 Thus, a combination of some factors such as cross-border communication between these countries for travel, work, trade, and medical cure as well as unbounded accessibility of antibiotic drugs such as carbapenems and antibiotic pollution could be the most important cause of this increasing trend. 6
The main carbapenem resistance mechanism in A. baumannii is frequently related to carbapenemase production, among which the most common ones are CHDLs or OXA-type enzymes and the next ones are MBL enzymes such as VIM, IMP, and NDM. Furthermore, the loss or decrease in OMPs and overexpression of RND-type efflux pumps are the other major mechanisms of resistance. 5 According to this analysis, in Iran, the production of carbapenemase due to the presence of blaOXA23 (55.3%) was the most prevalent reported mechanism of carbapenems resistance followed by the existence of blaOXA-24 like (44.1%) genes. These data indicated that increase in resistance to carbapenems in clinical A. baumannii is principally related to the distribution of OXA-producing strains. Genes encoding OXA carbapenemase such as blaOXA23 can be allocated in the plasmid elements belonging to the IS4 family. The presence of specific IS such as ISAba1, located upstream of blaOXA genes, explained that they could often provide promoter sequences for these genes. 19 So an increase in the expression of blaOXA genes results in diminishing the carbapenems' susceptibility.31–33 The main issue about OXA carbapenemases is their capability to quickly mutate and develop their range of activity. 5 OXA-23 belongs to a CHDL subgroup named OXA-23-like, which is the most common acquired resistance mechanism in the different parts of the world.34–36 In neighboring countries such as Turkey, Afghanistan, and Pakistan they have been frequently presented.10,37
Twenty five percent and 29.1% of these reported CRAB contained blaOXA-40 and blaOXA-24 genes, respectively, that belong to a second subclass of CHDLs termed OXA-24-like comprising OXA-24, OXA-25, OXA-26, OXA-40, and OXA-72. OXA-40 was recognized in CRAB isolates and has been found to be prevalent in France, Spain, and Portugal.38–40 Moreover, OXA 24 and OXA40 indicate that OXA-72 is the most common mechanism of carbapenem resistance in some countries in the Southern part of Europe such as Croatia, Bosnia and Hecegovina, Serbia.20,22
The other subclass of CHDLs consists of OXA-58, which was originally known in a CRAB isolate in France, 41 responsible for about 5% of reported CRAB in Iran. Several investigations have identified the blaOXA-58 gene in A. baumannii isolates from different countries such as Iraq, Kuwait, Turkey, Romania, Greece, Austria, the United Kingdom, and Spain.33,42,43 The blaOXA-58 and blaOXA-23 genes have also been identified in A. baumannii isolated from damaged U.S. military personnel in Iraq and Afghanistan. 10
In addition, in most of the studies conducted in Iran and other countries, VIM- and IMP-type genes were the most predominant genes in MBL producer A. baumannii.42–45 Besides, the highest rate of resistance caused by NDM carbapenemases has been found to be in Pakistan, whereas in other regions of the Middle East they have been reported sporadically. 10
Diversity of carbapenemase enzymes may be influenced by historical and social dealings and may also be due to wars and travels. Thus, proper management is desirable to control these infections. The remarkable therapeutic choices for CRAB infections are tigecycline and colistin; if resistance to them develops in recent years, the drug resistance crisis may cause high morbidity and mortality.
There were some limitations to this study that should be considered. First, there were limited data regarding non-carbapenemase-resistant mechanisms such as porin loss and specific efflux pump systems in A. baumannii isolates. Increased information about these mechanisms, in addition to the production of carbapenemase, can fortify the real judgment about CRAB in Iran. Second, it cannot fully represent the prevalence of CRAB, because the extent of this bacterium has not yet been assessed in some regions of Iran. Third, we were unable to determine the risk factors for CRAB infection due to the limited information obtained from the studies. Forth, heterogeneity exists among the included studies. Finally, as with any systematic review, the existence of potential publication bias should be considered.
In conclusion, this article warns that antimicrobial resistance will rise every year if the current situation remains uncontrolled. We also propose that the blaOXA-23 gene may be one of the most widespread reported mechanisms for the development of CRAB in Iran. Better control infection and antibiotic management, particularly in the health care systems, should be obligate to decrease the dissemination and emergence of antimicrobial resistance. It is suggested that a susceptibility test for carbapenems could be predominantly needed if the patient had been cured with carbapenem and glycopetides earlier. Further, to achieve the goal, to decrease the development of CRAB, the regional collaboration has been highlighted by Iran and its bordering countries.
Footnotes
Acknowledgment
The authors thank the reviewers of the Microbial Drug Resistance Journal for their helpful and thoughtful comments.
Authors' Contributions
M.J.N. and P.T.: Designed the protocol.
M.J.N., S.Z., F.F., M.A., R.B., and B.H.: Performed the search, data extraction, and statistical analysis.
M.J.N. and S.Z.: Wrote the first draft of the article.
M.J.N., S.Z., H.G., H.D., M.M.F., and P.T.: Revised the article.
Disclosure Statement
No competing financial interests exist.