
Abstract
Aims:
To determine the prevalence and the antibiotic resistance patterns of Campylobacter jejuni isolated from pediatric diarrhea patients in central Iran.
Materials and Methods:
Stool specimens (n = 230) were investigated using a modified Gram stain, two specific culture media, and C. jejuni-specific PCR. Antibiotic resistance profiles and relevant resistance genes were determined. Genetic relationships among a selection of the isolates were studied by Fla typing.
Results:
Out of the 230 diarrhea samples, 48 (20.8%) cases of C. jejuni were identified using modified Gram stain, 45 (19.5%) using the culture media, and 76 (33%) cases were identified using PCR. The highest antibiotic resistance rates were observed in 37 (82.2%) strains against tetracycline, in 32 (71.1%) against ciprofloxacin, and in 31 (68.8%) against erythromycin. Twenty (44.4%) isolates were resistant to ciprofloxacin and erythromycin simultaneously. Genotypic investigations found 36 (97.3%) strains carrying the tet (o) gene, 31 (96.8%) harboring the cmeB gene, 22 (68.7%) strains with the gyrA6 gene, 20 (64.5%) strains containing a 23S rRNA mutation, and 21 (65.6%) strains with the qnrS gene. Fla typing of a random subset of 14 strains revealed 11 different types showing the genomic diversity of the isolates. Strains sharing the same Fla type could be easily distinguished by their resistance gene profile.
Conclusions:
This is the first study to demonstrate that genetically diverse quinolone–macrolide-resistant C. jejuni is an important cause of gastroenteritis in children from central Iran. Pediatricians should consider these resistance features once the antibiotic prescription is necessary for prevention of possible complications, especially in those under 5 years of age. Of note, most cases of Campylobacter diarrhea are self-limiting and antibiotics should only be prescribed in those cases where severe complications evolve.
Introduction
According to the World Health Organization, diarrhea causes the death of about 525,000 children under five every year. 1 The most common pathogens causing gastroenteritis in children in Iran are Campylobacter spp., Shigella spp., Salmonella spp., pathogenic Escherichia coli prototypes, Norovirus, Adenovirus, Rotavirus, Giardia lamblia, and several other but more minor pathogens.2–8 Campylobacter infection has been reported to be one of the most common causes of acute diarrhea, especially in children under three and in the elderly. 9 The epidemiological data on campylobacteriosis in Africa, Asia, the Middle East, and developing countries are incomplete. 10 Although in most cases Campylobacter infections are self-limiting, children's stool samples should be microbiologically examined for Campylobacter, since diarrhea in children can cause serious complications and sequelae. 11 However, in most cases, conservative treatment will suffice and antibiotic prescription is recommended only for severe and prolonged diarrhea, mostly in immunocompromised patients and other clinically complicated cases. Currently, macrolides are considered the drugs of choice for the treatment of campylobacteriosis. However, fluoroquinolones are also commonly used, 11 whereas also tetracycline and gentamicin may be administered for systemic treatment of Campylobacter spp. infections. 11 This infection can arise due to several factors, including exposure to natural Campylobacter reservoirs (mostly birds and water reservoirs), the immunity level of the population examined, various nutritional habits leading to the consumption of poorly cooked food, differences in lifestyle and diet (especially poultry consumption), and close interactions with animals and the environment. 10 The most commonly reported sources of Campylobacter infection are poultry products, particularly chicken, and contaminated water. 10 For example, one study showed that 70% of sporadic Campylobacter infections were associated with eating poorly prepared chicken. 12 The current evidence suggests that infection with antibiotic-resistant Campylobacter spp. causes longer and more severe disease. 13 Antibiotic resistance, especially against fluoroquinolones and macrolides, has emerged in Campylobacter jejuni worldwide. 13
The gold standard for identifying Campylobacter is a stool culture, but PCR can also be used to confirm a diagnosis. 14 Still, the diagnosis of Campylobacter infection using PCR is relatively expensive and needs experienced technicians to perform the test. PCR technology is not available in all clinical diagnostic laboratories especially in the emerging economies. Hence, Campylobacter screening is not routinely performed in hospitals and medical diagnostic laboratories in Iran. Previously, no comprehensive studies have been conducted on the role of Campylobacter in pediatric infectious diarrhea in this country. Even if Campylobacter is implicated or suspected in a case of developing pediatric diarrhea, no information is available on the bacterial susceptibility to or resistance against the antibiotics that might be used for treatment. Among the various methods of typing, restriction fragment length polymorphism (RFLP) analysis of the flagellin gene (flaA) is widely used because of its speed, ease of application, and cost-effectiveness. 15 The presence of highly conserved regions in conjunction with polymorphic regions has made it an optimal genomic target for use in Campylobacter epidemiology. 16
In this study, we present the first report on the prevalence, antibiotic resistance (both phenotypically and genotypically), and genetic diversity of C. jejuni isolated from stool samples of pediatric patients in central Iran.
Materials and Methods
Sample collection
This descriptive cross-sectional study included samples from 230 children with diarrhea who were referred to the Children's Educational Therapeutic Center affiliated with the Arak University of Medical Sciences from May to September 2015. All the patients who were able to produce at least one stool sample were included in the study.
A questionnaire and a consent form were provided to patients and their parents or guardians. The inclusion criteria were direct observation of over five white blood cells per high-power field in a nonformed stool sample and completion of the consent form. 17 None of the patients had taken antibiotics in the week before they were referred to the hospital. Thirty-four children were excluded from the study for three main reasons. Some (n = 20) were already on antibiotics, parent refusal led to refusal in 10 cases, and 4 patients provided insufficient specimens. This study was approved by the Ethics Committee of the Arak University of Medical Sciences under approval number IR.ARAKMU.REC.1395.83.
Phenotypic investigation
Modified gram stain
A mixture of sample containing mucus, phlegm, and red and white blood cells were used to prepare smear less than 10 minutes after the sample was obtained. The slide was then stained using a modified Gram stain (1% carbol fuchsin for 5 minutes while heating) and examined through a microscope. 18
Culture
Culture media
For enrichment, a 2 mL stool sample was directly inoculated into Preston medium (Ibresco, Iran) and incubated in a jar with a C class gas-pack (Merck, Germany) at 42°C for 72 hours. A sample from this medium was then cultured on modified charcoal cefoperazone deoxycholate agar (mCCDA) medium (Ibresco) and placed in a jar with a C class gas-pack for 72 hours at 42°C. 19
Brucella agar with 10% lysed sheep blood with filter
From each enriched Preston medium, 200 μL of microbial sediment was deposited on a 45 nm cellulose acetate membrane filter (Sartorius, Germany) that was placed on Brucella agar medium (Merck) containing 10% lysed sheep blood. The plate was placed in a jar with a C class gas-pack at ambient temperature for 45 minutes. Then, the filter was removed, and the plate was incubated in the jar with a new C class gas-pack at 37°C for at least 72 hours. 19
Identifying Campylobacter from the infectious diarrhea samples
Modified Gram staining as well as oxidase, catalase, and hippurate tests (Merck) were performed on suspicious colonies (small white colonies in mCCDA media and Brucella agar with 10% lysed sheep blood with filter). A clinical specimen from the microbial collection of the Department of Microbiology, Faculty of Medical Sciences, Arak University of Medical Sciences was used as a positive control.
Investigating Campylobacter antibiotic resistance by disk diffusion
Once C. jejuni had been isolated, antibiotic resistance profiles were determined using the disk diffusion method according to the Clinical and Laboratory Standard Institute (CLSI) guideline. The antibiotics used included tetracycline (30 μg), erythromycin (15 μg), ciprofloxacin (5 μg; Mast Diagnostics, United Kingdom), and MICs for ampicillin and gentamicin were determined by antibiotic gradient testing (Liofilchem, Italy). Zone of inhibition equal or less than 12, 20, and 22 mm for erythromycin, ciprofloxacin, and tetracycline, respectively, were considered as resistant. For gentamicin an MIC level of ≥8 and for ampicillin ≥32 were considered as resistant. 20
Genotypic investigation
DNA extraction
DNA extraction was performed directly from the stool samples and the cultured C. jejuni isolates using the QIAamp DNA Stool Minikit (Qiagen GmbH, Hilden, Germany) according to the protocol. The amount and purity of extracted DNA were measured using a NanoDrop device (Thermo Fisher Scientific) and then confirmed using bacterial universal primers of 16SrRNA. 21 The oligonucleotide primer 16SrRNA-F 5-AGGAGGTGATCCAACCGCA-3 and 16SrRNA-R 5-ACCTGGAGGAAGGTGGGGAT-3 were used for amplification of 16srRNA gene. The PCR program to amplify the 16srRNA gene included an initial denaturation at 95°C for 5 minutes, 40 cycles of 95°C for 30 seconds, 55°C for 30 seconds, and 72°C for 1 minutes, and a final elongation step at 72°C for 5 minutes. 21
PCR amplification
The MapA gene was used as a genetic marker for confirming the isolates to be C. jejuni by PCR. The PCR program to amplify the MapA gene included an initial denaturation at 95°C for 10 minutes, 35 cycles of 95°C for 30 seconds, 59°C for 1.5 minutes, and 72°C for1 minute, and a final elongation step at 72°C for 5 minutes. 22 As positive control we used DNA isolated from C. jejuni ATCC 33560 and for negative control tubes were included 1 in every 20 tubes containing no external DNA extract.
Investigating genotypic resistance
PCR using primers specific for the antibiotic resistance genes, tet (O), CmeB, 23S, gyrA4, gyrA5, gyrA6, BlaOxa61, qnrS, and aphA-3-123–26 , were used to genotypically investigate antibiotic resistance. The 25 μL final volume of the PCR included 12.5 μL of master mix (1 × ), 2 μL of DNA template (5 ng), 1 μL of each forward and reverse primer (10 pM), 0.5 μL of Taq DNA polymerase (2.5 units), and 8 μL of double-distilled water (all reagents were purchased from Yekta Tajhiz Company, Tehran, Iran). For each positive sample representing one of the genes mentioned above, one was used for DNA sequencing of the PCR product (Gene Fanavaran Company, Tehran, Iran) and the sequence was identified by BLAST analysis.
Flagellin gene typing
Flagellin (Fla) gene typing was carried out as described by Tsang et al. (2001). PCR of the Fla gene was performed for the DNA extracted from isolates identified as C. jejuni. 23 RFLP analysis using the restriction enzyme Ddel was performed according to the protocol (Thermo Scientific, Germany). Results were interpreted visually.
Results
Phenotypic and genotypic investigation
Out of the 230 samples included in this study, 48 cases (20.8%) of Campylobacter were staining Gram positive or positive upon direct observation (Fig. 1). Forty-five cases (19.5%) were found positive for Campylobacter using one of the culture methods and differential tests for identification of C. jejuni. Twenty-eight cases (12.2%) of Campylobacter were identified through the use of specific mCCDA culture media. Thirty-seven strains (16%) of Campylobacter were isolated by means of Brucella agar medium with filtering. All of the 45 cases of positive samples (using one of the culture methods) were confirmed by PCR. Using specific primers to identify C. jejuni in DNA samples extracted from stool, 76 of the 230 samples (33%) were shown as positive.
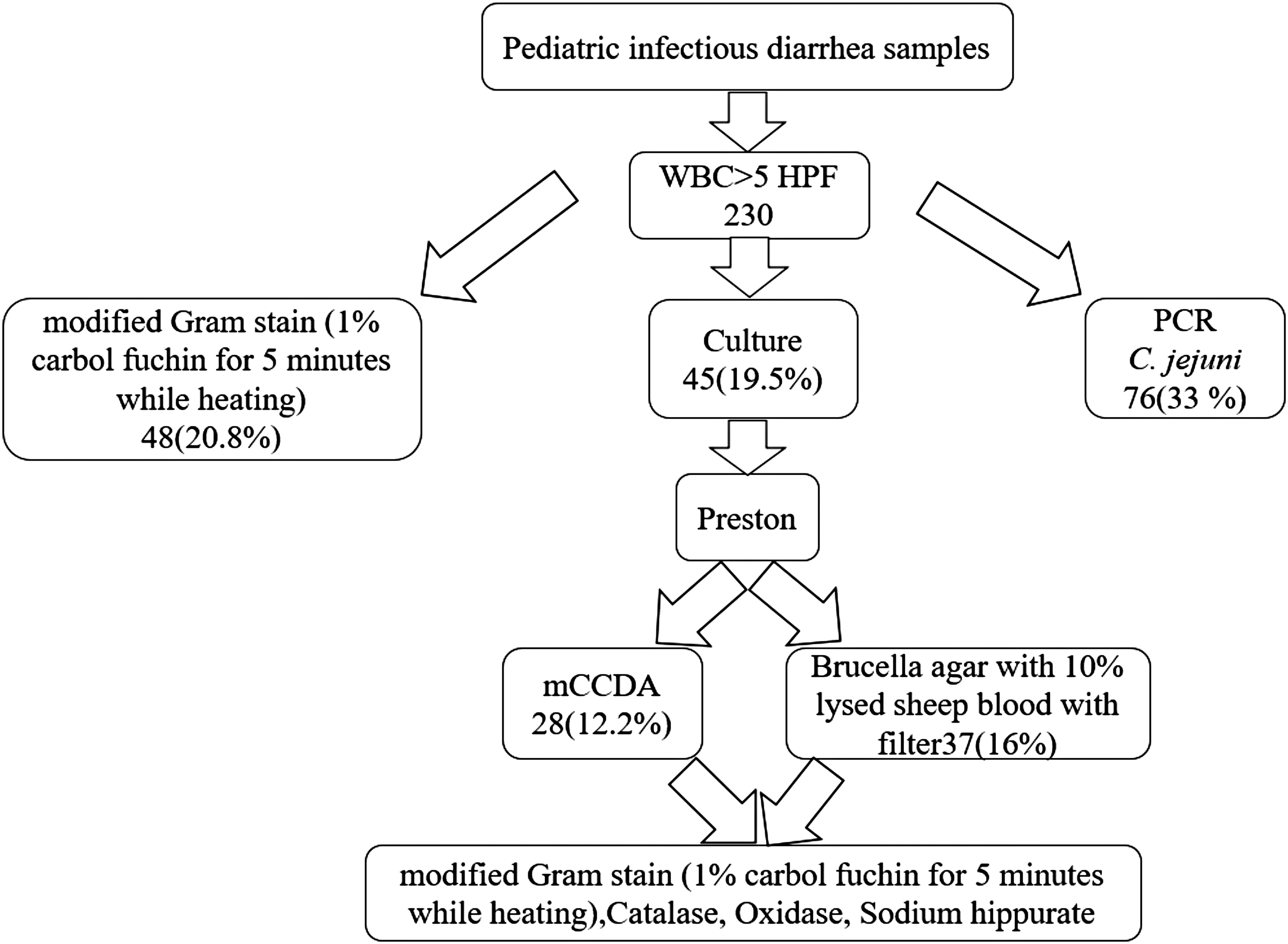
Testing for Campylobacter infections in pediatric patients from central Iran in 2015. Diagnostic flowchart used in this study.
Out of the total number of 230 children with infectious diarrhea included in the study, 42 (55.2%) male and 34 (44.7%) female patients were infected by Campylobacter, giving an infection ratio of males to females of 1.2:1. The average age of the patients with Campylobacter was 3 years and 4 months. The youngest of these patients was a 3-month-old boy and the oldest was a 10-year-old boy. The majority of Campylobacter infections (64 cases, 84.2%), were observed in children under the age of 5 years, especially in the age groups between 1 and 2 years of age (26 cases, 34.2%) (Table 1). Clinical symptoms of the children with Campylobacter infection included mucus in the stool (98.5%), abdominal pain (95%), blood in the stool (63.1%), fever (56%), and vomiting (11%).
Classification of Age Groups and Gender of 230 Pediatric Patients Infected by Campylobacter jejuni from Central Iran in 2015
Determination of antibiotic resistance using disk diffusion
Using the CLSI guidelines, the highest resistance rates in C. jejuni were observed against tetracycline (37 cases, 82.2%), ciprofloxacin (32 cases, 71.1%), and erythromycin (31 cases, 68.8%). Most C. jejuni isolates were found to be sensitive to gentamicin, and only four strains (8.8%) were found to be resistant (Table 2).
Phenotypic and Genotypic Antibiotic Resistance Rates in Campylobacter jejuni
Genotypic investigation of resistance
Genotypically, tet (O) and CmeB resistance genes were present in 36 (97.3%) and 31 (96.8%) of C. jejuni isolates, respectively. In addition, we found 20 cases (64.5%) with 23srRNA mutations. The least frequently encountered resistance gene was aphA-3-1, which was only found in three cases, which is 75% (Table 2).
Fla typing
This study used a convenience sample for Fla typing. Upon Fla typing of 14 selected strains we identified 11 different Fla types. One type occurred twice, another three times. Given the relatively low resolution of Fla typing this suggest significant genetic variability among the C. jejuni isolates. Of note, the strains that shared Fla types could be very easily distinguished based on their resistance gene profiles (see Supplementary Table S1, strains 8 and 38, and 29, 31, and 33).
Discussion
Increasing C. jejuni resistance to antimicrobials is a serious public health problem worldwide. 27 The prevalence of C. jejuni in infectious diarrhea samples obtained from children admitted to the children's hospital was determined using culture methods (45 cases, 19.5%) and PCR (76 cases, 33%). In similar studies in Egypt, Campylobacter spp. identified by culture methods accounted for 16 (4.6%) and those identified by PCR accounted for 23 (6.6%) cases. 28 In similar studies in Iran that used PCR, Campylobacter prevalence in pediatric diarrheal stool samples was reported to be much lower with 8% in Tehran and 9.6% in Hamadan.8,29 In studies that used culture detection methods, 7.5% of infectious diarrhea samples from all age groups that were referred to medical centers in Shiraz and 11.6% of samples that were referred to medical centers in Zahedan were identified as Campylobacter positive.30,31 Worldwide, Campylobacter prevalence has been shown to vary from 4.5% to 41.3% when testing nonformed fecal samples.32,33 A comparison of the present results with the abovementioned studies indicates that C. jejuni is an important causative factor in developing diarrhea in children in central Iran. Since Campylobacter detection is not part of Iran's routine diagnostic programs, a microbiological study isolating Campylobacter in hospital and medical diagnostic laboratories is needed. 30
In this study, the average age of the patients infected with Campylobacter was 3 years and 4 months. This result contrasts with the Pakistan average age report of 18 months. 12 Most of the infections analyzed in our study occurred in children under five, especially in the age range of 1–3 years. In similar studies in Pakistan, China, and Tanzania, the age range was under 2 years and in Bangladesh this age ranged between 2 and 3 years. 12 Likely, these differences are attributable to weaknesses in the immune systems or different nutritional statuses. 12 In this study, the infection ratio of males to females was 1.2:1, which is similar to the ratios found in other Campylobacter prevalence studies. 34
Among our strains, C. jejuni phenotypic resistance to macrolides was found in 31 (68.8%) cases, and 23 (74.1%) cases revealed that the presence of the CmeB gene was associated with this type of resistance. This resistance was previously reported to be 2.9% in Tehran and increased from 49.3% in Poland (1994–1996) to 88.9% (2005–2008).8,11 The prevalence of the 23srRNA mutation in erythromycin-resistant Campylobacter strains has been reported as zero percent in The Netherlands and 0.14% in Spain.35,36 This difference may be due to the significant variation in the genes that affect macrolide resistance, each of which acts separately and differently in variant strains. 37 Considering the high levels of resistance, macrolides are not effective for the treatment of Campylobacter infections anymore in this geographical area. Pediatricians should consider this information when treating children, especially when no culture media or detailed antibiograms are available. Of note, the vast majority of Campylobacter infections are fortunately self-limiting.
Resistance to fluoroquinolones was observed in 32 cases (71.1%) and the genes highly involved in this resistance were CmeB in 31 cases (96.8%), qnrS in 21 cases (65.6%), gyrA4 in 21 cases (65.6%), gyrA5 in 14 cases (43.7%), and gyrA6 in 22 cases (68.7%). Phenotypic resistance to fluoroquinolones in C. jejuni has been reported to be as high as 61.7% in Tehran and even higher (72%) in Spain.8,38 The prevalence of CmeB in ciprofloxacin-resistant Campylobacter strains has been reported to be 60% in Slovakia. 39 As was the case for macrolide resistance, many different genes are involved in fluoroquinolone resistance. This may result in complex associations between a phenotype and the underlying genotype. Generally, increased resistance to ciprofloxacin in C. jejuni species has been observed over the past two decades in many parts of the world. 40
In this study, the resistance to tetracycline in C. jejuni was phenotypically observed in 37 cases (82.2%), and in 36 cases (97.3%) the tet (O) gene seemed to be involved in this resistance. This resistance has been reported as 20.5% in Tehran and 85.7% in Iraq.8,41 Also, the prevalence of tet (O) in tetracycline-resistant Campylobacter strains has been reported to be 77.7% in Slovakia. 39
In general, β-lactam antibiotics have a limited effect on Campylobacter species and resistance to this class of antibiotics appears to be β-lactamase mediated and inherent. 11 In this study, resistance to ampicillin in C. jejuni was phenotypically observed in 13 cases (28.8%) and 3 (23%) out of 13 harbored the Oxa61 resistance gene.
Phenotypic resistance to ampicillin has been reported as 11.7% in Tehran, 29.3% in Spain, and 71.4% in Iraq.8,38,41 Also, prevalence of BlaOxa61 in ampicillin-resistant Campylobacter strains has been reported as 61.1% in Slovakia. 39
Resistance to gentamicin in C. jejuni was phenotypically observed in 4 cases (8.8%) and out of 4 cases 3 (75%) harbored aphA-3-1 gene, whereas this phenotypic resistance has been reported as 0% in Tehran, as 0% in Iraq, and 8.6% in Spain.8,38,41
Considering the use of macrolides, fluoroquinolones, and tetracyclines as growth promoters in poultry food and as drugs for the treatment and prevention of bacterial infections in veterinary medicine, resistance to these antibiotics has increased in the central part of Iran as in other parts of the world. 40 Studies in south and north Iran illustrated that the frequency of C. jejuni in turkey and chicken carcases was 80.8% and 41.6%, respectively. The frequency of ciprofloxacin resistance among these isolates was 62.1% and 81.9%. At the same time 67.8% and 69.2% of the isolates from carcases were resistant to tetracycline. Clearly this presents a health risk that should not be overlooked.42–44
Fla typing is often used to type C. jejuni. This is the first report on Fla diversity among C. jejuni isolated from stool samples obtained from patients in the central part of Iran. In combination with the selective presence of resistance genes, all isolates described in this study were found to be genetically different. Since Campylobacter is a natural inhabitant of water, sewage, and animals' digestive system, it can be claimed that different Campylobacter species possibly originate from different sources. 45 However, specific strains have been isolated in some geographic regions in some studies indicating that they are endemic and these strains have been isolated from different samples (for instance, from poultry farms, slaughterhouses, and patients) and are known as endemic strains.46,47 But due to diversity of our Campylobacter strains there is no single endemic strain in Central Iran.
Conclusion
Given the elevated prevalence and antibiotic resistance of C. jejuni from infectious diarrhea samples in children under 5 years of age from central Iran (especially those between 1 and 2 years of age), health and laboratory staff in the Markazi Province should be trained in diagnostic methods to identify Campylobacter and determine its antibiotic resistance. Also, specific support measures and additional practical information are required for improved food preparation methods and surveillance of food safety measures for everyone especially those at risk. Although the majority of Campylobacter infections are self-limiting, the existence of extensive resistance to the three first-line therapeutic antibiotics (macrolides, fluoroquinolones, and tetracycline) should always be considered by pediatricians. The efficacy of the prescribed treatment should be reinvestigated in follow-up visits. Developing a coherent program and controlling and monitoring antibiotic care (surveillance program) can help to resolve the resistance problem in the long run.
Footnotes
Acknowledgment
The authors appreciate the financial assistance from Arak University of Medical Sciences (Grant No. 2571).
Disclosure Statement
No competing financial interests exist. A.v.B. is an employee of bioMerieux, a company designing, developing, and selling infectious disease tests. The company had neither influence on the design and execution of the study nor in the writing of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.