
Abstract
Antibiotic resistance is an increasing phenomenon and has become a serious public health concern. Nowadays, limited therapeutic options exist for the treatment of invasive infections caused by drug-resistant strains, particularly methicillin-resistant Staphylococcus aureus (MRSA). The present study was conducted to analyze the published literature on the in vitro activity of tedizolid toward MRSA strains. A systematic literature search was conducted on the Web of Science, PubMed, Scopus, and Google Scholar electronic databases from January 2000 to December 2017 to cover all published articles relevant to our study. Then, 18 publications that met our inclusion criteria were selected for data extraction and analysis by the Comprehensive Meta-analysis software. The overall antibacterial activity of tedizolid on 10,119 MRSA isolates was estimated 0.25 and 0.5 μg/mL for MIC50 and MIC90 (minimum inhibitory concentration at which 50% and 90% of isolates were inhibited, respectively), respectively. The pooled prevalence of tedizolid susceptibility was estimated at 99.6% (95% confidence interval: 99.5–99.8%). Only 4 of 18 included publications have reported the antibacterial activity of tedizolid against linezolid-resistant isolates, of which the MIC range of tedizolid was 0.25–16 μg/mL. Of the four studies, all of the linezolid-resistant isolates were susceptible to tedizolid in one study, and in the other studies, the susceptibility rates were <50%. Based on the results of the systematic reviews, tedizolid had a promising antibacterial activity against MRSA isolates from different clinical sources. However, future studies are needed to provide clinical evidence to support these observations.
Introduction
S
Antibiotic resistance is an increasing phenomenon and has become a serious public health concern in the treatment of diseases. 7 Nowadays, limited therapeutic options exist for the treatment of invasive infections caused by multiple drug-resistant (MDR) strains, most notably methicillin-resistant S. aureus (MRSA).8,9 Vancomycin remains as the most important therapeutic drug of choice for treatment of infections caused by MDR strains of Gram-positive cocci, particularly MRSA. 10 However, in the past years, intermediate and complete resistance to vancomycin has emerged as a consequence of the overuse of this antibiotic in hospitals. 7 The increasing trend of vancomycin nonsusceptible strains of S. aureus has triggered alarms for the management of related life-threatening infections in hospitalized and nonhospitalized patients. 11
The oxazolidinone antibiotics such as linezolid have demonstrated promising antimicrobial activities against Gram-positive pathogens such as MRSA strains. 12 Linezolid inhibits bacterial protein synthesis through binding to the peptidyl transferase center of the 50S ribosomal subunit. 12 However, linezolid-resistant strains were reported rarely in the hospital environment. 13 Although resistance to linezolid has been slow to develop, the emergence of linezolid-resistant S. aureus containing a horizontally transferable gene known as cfr represents a potential risk for its widespread dissemination. 14
Tedizolid is a novel oxazolidinone-class antibiotic approved by the U.S. Food and Drug Administration (FDA) in 2014 for the treatment of acute bacterial skin and skin structure infections. This substance also is under investigation for the treatment of hospital-acquired pneumonia. 15 Tedizolid phosphate is a phosphate monoester prodrug of the active compound tedizolid, which is effective against acute bacterial skin infections. 16 Despite the similar antibacterial mechanism as linezolid in inhibiting protein synthesis, tedizolid has potential activities against linezolid-resistant strains due to the replacement of the acetamide group with a hydroxymethyl group. 17 Also, a D-ring substituent (tetrazole), which is lacking with linezolid, improves its potency through increased interaction with additional sites on the ribosome. 17 Tedizolid treatment versus linezolid is associated with lower incidence of drug-related adverse events, higher accumulation in alveolar macrophages, and no need for adjustment when switching from intravenous (IV) to oral (PO) route of administration.14,17,18
Tedizolid phosphate is available in both PO and IV formulations that do not require dosage adjustments in renal or hepatic dysfunction. Tedizolid has a longer half-life relative to linezolid, which allows for a once-daily dose with a short 6-day course compared with a twice-daily dose for a 10-day course of linezolid. 19 There are few studies on pharmacoeconomic analyses of tedizolid versus other treatment options. To date, only two studies have reported cost-effectiveness of tedizolid versus linezolid for patients with acute bacterial skin and skin structure infection (ABSSSI). Both results suggested potential cost savings of tedizolid versus linezolid in a standard treatment course. Insinga et al. estimated a net cost savings of 55€ for tedizolid per treated ABSSSI patient versus linezolid. 20 Kauf et al. calculated total drug costs for a standard course of tedizolid and linezolid as $1,562 and $2,816 per patient, respectively. 21 Despite these encouraging findings, additional global data are still needed to determine the economic benefits that may be achieved with tedizolid in both hospitalized and outpatients. 20
Knowledge of antimicrobial resistance patterns is essential to define empirical therapy. However, there is a lack of comprehensive studies comparing tedizolid susceptibility against MRSA strains originating from different regions and samples within previously published data. Therefore, the present study was conducted to analyze the published literature on the in vitro activity of tedizolid toward MRSA strains to contribute to the international data on antimicrobial stewardship programs.
Materials and Methods
Search strategies
A systematic literature search was conducted on the Web of Science, PubMed, Scopus, and Google Scholar electronic databases from January 2000 to December 2017 to cover all published articles relevant to our study. The comprehensive search was performed using the following terms and combinations, including “tedizolid” or “torezolid” or “tedizolid phosphate” or “TR-701” or “TR-700” in combination with “in vitro susceptibility” or “in vitro activity” in the title, abstract, and keywords fields.
Selection criteria and quality assessment
Two reviewers independently screened the search results at the databases with the related keywords and analyzed the titles, abstracts, and full texts to examine their eligibility for inclusion according to the inclusion criteria. Any disagreement between reviewers was resolved by consensus. No language restrictions were applied in our search, but the abstract must be available in English. All articles indexed in the Web of Science or PubMed or Scopus with the following inclusion criteria were retrieved: (1) antibacterial activity was determined using one of the standard methods, including broth microdilution, agar dilution, and epsilometer (E)-test, (2) MIC50 and MIC90 (minimum inhibitory concentration at which 50% and 90% of isolates were inhibited, respectively) and their ranges were available, and (3) original studies that were performed on clinically derived isolates. Meanwhile, exclusion criteria were (1) studies that did not use mentioned antibacterial susceptibility testing methods, (2) studies with a sample size <10 isolates, and (3) studies performed on samples with animal or environment origin. Furthermore, reviews and systematic review articles, case reports, and articles available only in the abstract without necessary information were not included. All susceptibility rates in the present study were estimated and reported based on the Clinical and Laboratory Standards Institute (CLSI) breakpoints. 22
Definitions
MIC breakpoints for tedizolid based on the CLSI guideline are ≤0.5 for susceptible, 1 for intermediate resistant, and ≥2 for resistant. Meanwhile, based on the European Committee on Antimicrobial Susceptibility Testing (EUCAST) definitions, 23 an MIC value of ≤0.5 was considered susceptible and an MIC value of >0.5 was considered resistant. The nonsusceptible term was used wherever MIC range exceeds the susceptible range, but the exact rates of intermediate and resistant isolates were not mentioned.
Quality assessment
The validity of studies was evaluated independently by two authors using the modified Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist 24 and disagreements were resolved by consensus. Items related to title and abstract, introduction, methods, results, discussion, and other information were determined and a score was assigned to each item. One score was assigned to each question and studies that achieved at least eight quality scores were considered eligible and included in the study.
Data extraction
We extracted detailed information of first author name, publication date, the study performing time, antibacterial susceptibility testing method, geographical distribution of samples, sample type, MRSA sample size, MIC results, and antibiotic susceptibility rate based on a preprepared list.
Statistical analysis
A meta-analysis was performed using a random-effects model to estimate the pooled prevalence and corresponding 95% confidence interval (CI). Heterogeneity between studies was measured using the Cochran's Q statistic and I2 index. Publication bias was tested using a visual examination of the funnel plot and Egger's weighted regression test (p < 0.05 was considered indicative of statistically significant publication bias). Analysis of data and construction of graphs were performed by the Comprehensive Meta-analysis software version 2.2 (Biostat). The mode, which is defined as the value that occurs most frequently in the data, was calculated using SPSS™ software version 21.0 (IBM Corp., Armonk, NY). The present study was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.
Results
A total of 2,060 articles were retrieved by the initial search of databases, of which 2,035 were removed following title, abstract, and index review, and 25 studies were selected for full-text analysis.
Among the remaining studies, two were not available in full text, two had results interpretation problems, full text or abstract of one study was not available in English, one study had a sample size <10, and antibacterial activity of tedizolid was not investigated in one study. Finally, 18 studies matched the eligibility criteria and were included in the meta-analysis.15,25–41 A flow diagram illustrating the literature search and study selection is shown in Fig. 1. The detailed characteristics of the included articles are specified in Table 1.
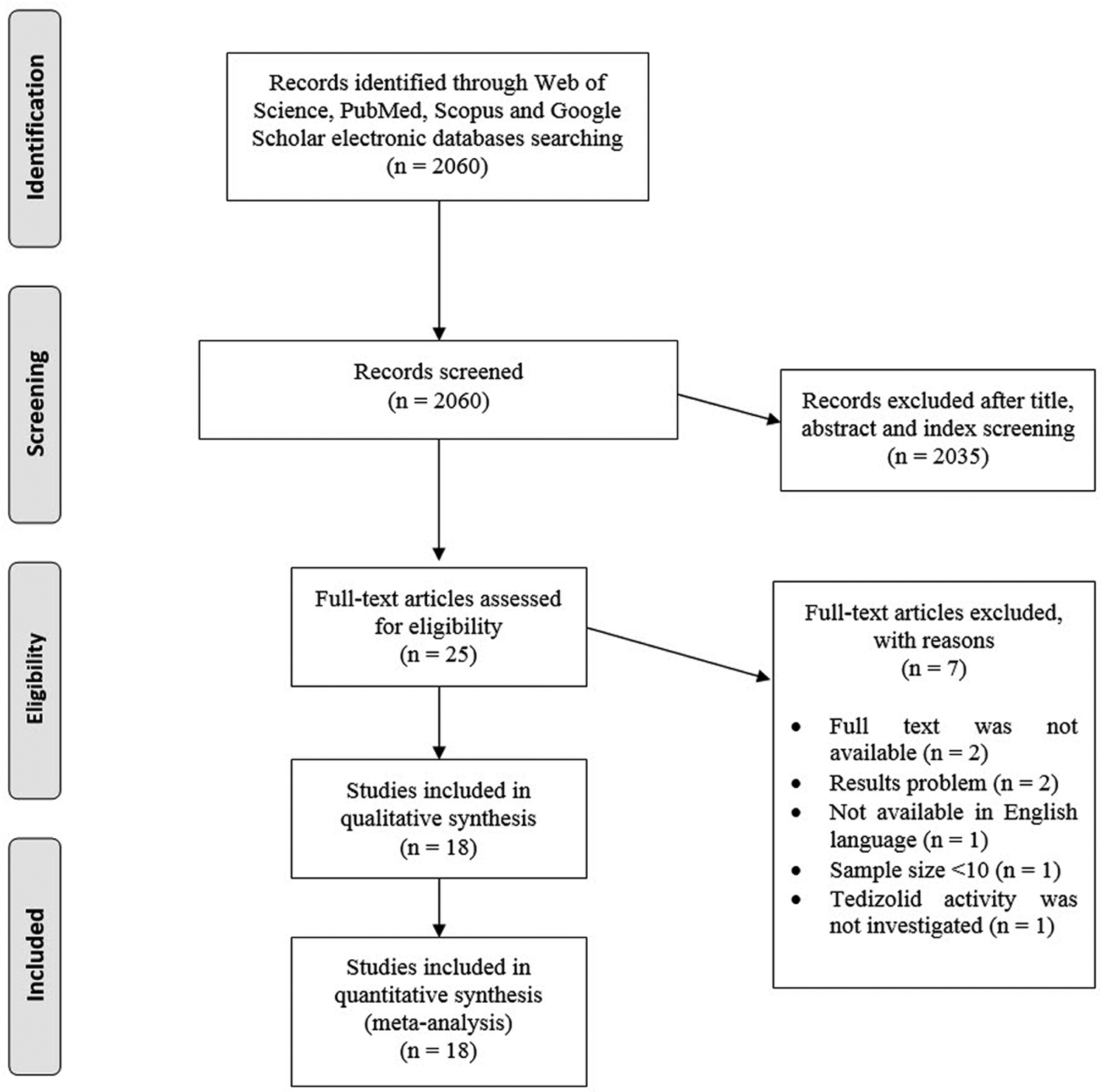
Flowchart of the literature search strategy and study selection.
The Full Characteristics of Studies Included in the Systematic Review
Based on MIC50/90 and CLSI breakpoints, at least 10% of isolates were nonsusceptible to tedizolid. However, 13 linezolid-resistant strains are included in the estimation; so, this might be a reason for increasing tedizolid MIC to the nonsusceptible range.
The tedizolid MICs of 99% of Staphylococcus aureus (100 MRSA and 100 MSSA) were ≤0.5 mg/L; so, <2% of MRSA isolates were nonsusceptible to tedizolid.
BSIs, bloodstream infections; CLSI, Clinical and Laboratory Standards Institute; HAP, hospital-acquired pneumonia; MIC50, minimum inhibitory concentration at which 50% of isolates were inhibited; MIC90, minimum inhibitory concentration at which 90% of isolates were inhibited; MRSA, methicillin-resistant S. aureus; MSSA, methicillin-susceptible S. aureus; PJI, prosthetic joint infection; RTIs, respiratory tract infections; SSSIs, skin and skin structure infections; SSTIs, skin and soft tissue infections; UN, unknown.
In this study, 18 articles from different North and South American, European, and Asian/Pacific countries were reviewed. In total, 21 collections of MRSA isolates were studied to determine the in vitro activity of tedizolid by evaluation of MICs. In the present study, to determine the effective concentration of tedizolid against MRSA isolates, the mode of MIC50, MIC90, and MIC ranges was estimated (Table 2). The overall antibacterial activity of tedizolid toward 10,119 MRSA isolates was estimated at 0.25 and 0.5 μg/mL for MIC50 and MIC90, respectively.
Antibacterial Activity of Tedizolid Against 21 Collections of Methicillin-Resistant Staphylococcus aureus Isolates
Because of the wide variation in detection range, we categorized all MIC ranges <0.2 μg/mL in one group.
The prevalence of tedizolid susceptibility can be estimated in 16 studies. From those studies, the pooled prevalence of tedizolid susceptibility was estimated at 99.6% (95% CI: 99.5–99.8) (Fig. 2). There was no significant heterogeneity among the 16 studies (χ 2 = 14.467; p = 0.49; I2 = 0%). The funnel plot for publication bias showed no evidence of asymmetry (Fig. 3). In addition, Egger's tests were performed to quantitatively evaluate the publication biases. According to the result of Egger's test (t = 0.12, p = 0.91), no evidence of publication bias was observed.
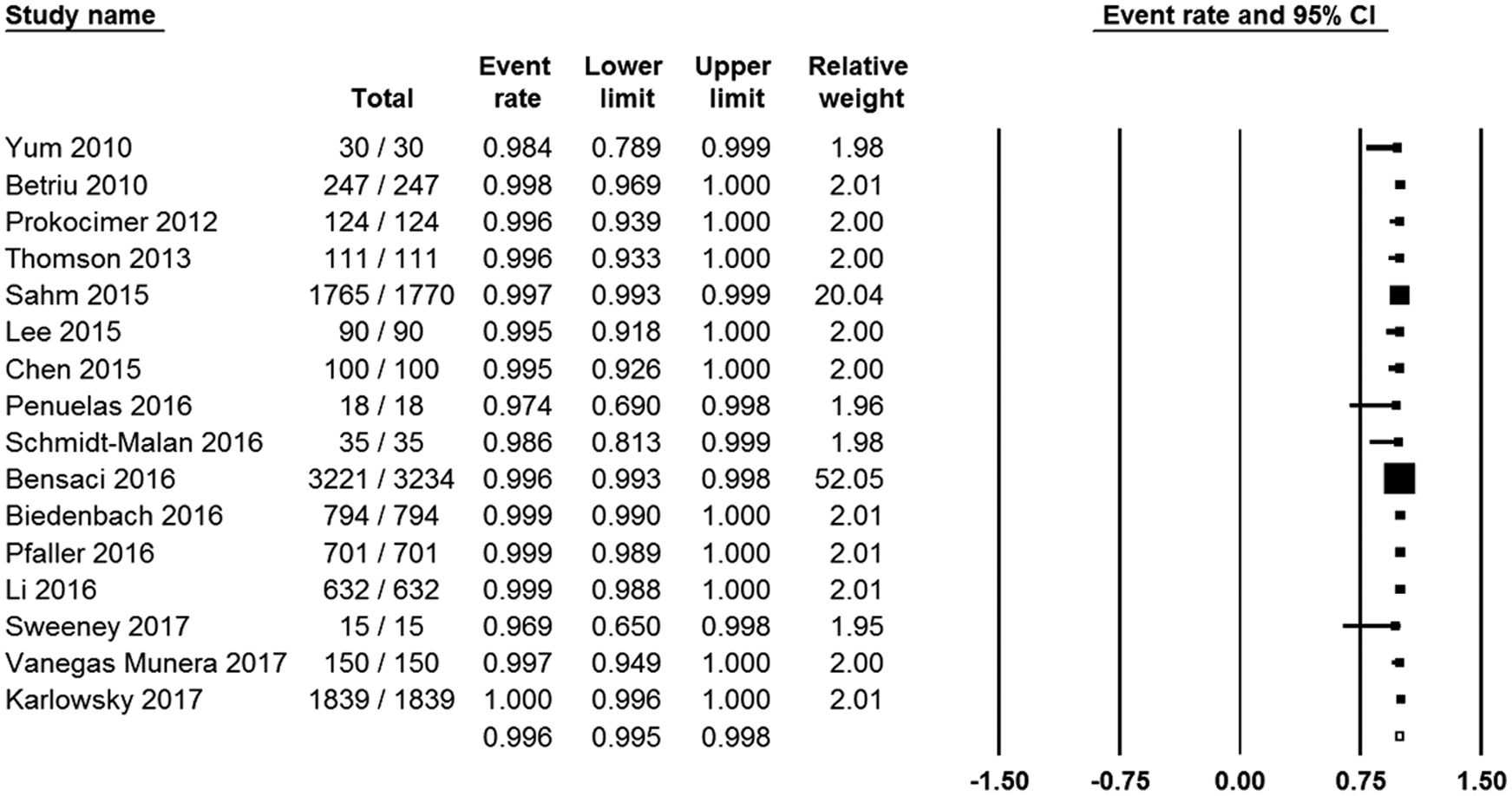
Forest plot of the pooled prevalence of tedizolid susceptibility.
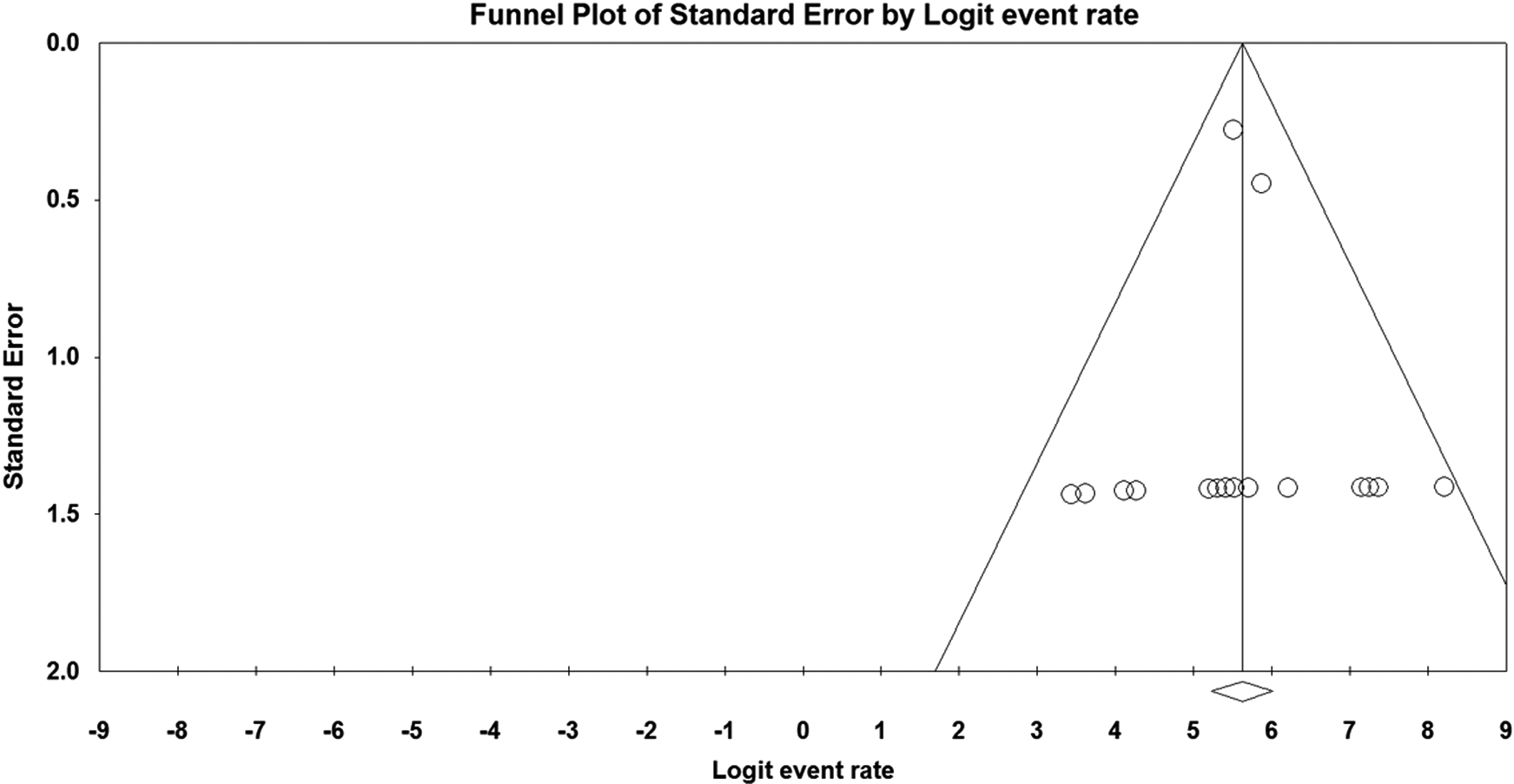
Funnel plot of meta-analysis on the pooled prevalence of tedizolid susceptibility.
Only 4 of 18 included publications reported the antibacterial activity of tedizolid against linezolid-resistant isolates, in which the MIC range of tedizolid was 0.25–16 μg/mL (Table 3). Of the 4 studies, all the linezolid-resistant isolates were susceptible to tedizolid in one study, while in the other studies, the susceptibility rates were <50%.
Antibacterial Activity of Tedizolid Against Four Collections of Linezolid-Resistant Staphylococcus aureus
Based on MIC50 and CLSI breakpoints, at least 50% of isolates were nonsusceptible to tedizolid.
Discussion
Drug-resistant bacteria are a major public health concern and are associated with increased morbidity and mortality. 42 MRSA is among the most important of these bacteria that lead to health problems due to epidemiologic diversity for the management of their infections.43,44 To prevent and control these problems, improvement of stewardship, infection control, and introducing new effective antibiotics are necessary. 45
Glycopeptide antibiotics, particularly vancomycin, are often the main therapeutic option for severe MRSA infections. Therefore, the emergence and spread of MRSA strains with increased resistance to vancomycin are a serious challenge for clinicians.7,46 The recent systematic review and meta-analysis of the epidemiology of vancomycin-intermediate S. aureus (VISA) and heterogeneous VISA (hVISA) at a global scale estimated that the prevalence of hVISA was 6.05% and VISA was 3.01%. 47 MRSA strains that have complete resistance to vancomycin (vancomycin-resistant S. aureus [VRSA]) are rare, but there are infrequent global reports from the United States, India, Iran, Pakistan, and Portugal. 48 A comparison of these reports with our results indicates the promising antibacterial activity of tedizolid against clinical isolates of MRSA because of a low rate of the nonsusceptible isolate (0.4%). Moreover, the estimated MIC value of tedizolid against MRSA with 0.25 μg/mL for MIC50 and 0.5 μg/mL for MIC90 is much lower than the MIC value of vancomycin for MRSA in the literature.15,27,29,33,37 In this regard, Barber et al. reported MIC value of tedizolid against VISA strain in the range of 0.03–1 μg/mL, which is several folds lower than the MIC value reported for vancomycin for VISA (i.e., 4–8 μg/mL). 49 These observations indicate that tedizolid compared with vancomycin more likely will achieve clinical concentrations. 50
The antibacterial activity of linezolid against MRSA in the literature is high (99.7–99.8%)32,36 and is comparable with our results for tedizolid (99.6%). However, based on previous reports, tedizolid with lower MIC had several folds greater in vitro potency than linezolid against MRSA strains.15,32,36,38,40 Regarding the activity of tedizolid on linezolid-resistant strains, these results are not strong enough and testing on larger collections of linezolid-resistant strains is needed before any recommendations for treatment purposes. Besides, it seems that cross-resistance to tedizolid is more likely to be associated with chromosomal resistance rather than a plasmid-mediated mechanism and carrying the cfr gene.32,49 In this context, it has been suggested that tedizolid activity against linezolid-resistant strains containing the cfr gene will be the most important benefit if this resistance mechanism becomes widely disseminated. 14
The results of the present study along with those clinical investigations that showed the use of tedizolid had a more favorable profile, efficacy, and safety compared with linezolid might warrant its use as an appropriate treatment option for MRSA infections.17,51
Finally, the main limitations of the present study are an unadjusted range of tedizolid concentrations through the included studies, self-estimation of resistance rates based on MIC breakpoints in some of the studies, too few strains with linezolid resistance, and performing the same investigation for methicillin-susceptible S. aureus (MSSA) isolates.
In summary, based on the systematically reviewed in vitro data, tedizolid has the promising antibacterial activity against MRSA isolates from different clinical sources. These results are encouraging for the use of tedizolid as a treatment option of infections caused by MRSA, regardless of geographical distribution. However, there is some shortage in the use of tedizolid against MRSA strains with reducing susceptibility to linezolid. Nevertheless, future studies are needed to provide clinical evidence to support these observations.
Footnotes
Disclosure Statement
No competing financial interests exist.