
Abstract
This study aimed to characterize the main mechanisms of acquired antimicrobial resistance of 103 multidrug-resistant Acinetobacter baumannii isolated from bloodstream from 2006 to 2016 from a hospital in Londrina, Brazil. All 103 isolates were identified as A. baumannii by amplification of the blaOXA-51-like and rpoB genes. Mortality was observed in the majority (81.6%) of the patients. High non-susceptibility rates (100.0–10.7%) were obtained for the evaluated antimicrobials, including colistin, polymyxin B, and tigecycline, and most isolates were classified as extensively drug-resistant (78.6%). Carbapenemase production was observed in 92.2% of the isolates. All carbapenem-resistant isolates showed a carbapenem-hydrolyzing class D β-lactamase being either blaOXA-23-like (97.9%) or blaOXA-143-like (2.1%). None of the isolates had the genes blaOXA-24-like, blaOXA-58-like, blaOXA-48, blaKPC, blaNDM, blaSPM-1, blaSIM-1, blaVIM, blaIMP, blaGIM, blaGES, mcr-1, qnrA, qnrB, qnrC, qnrS, and qnrVc. As a genetic context of the blaOXA-23-like gene, Tn2006 was predominated (86.0%), and Tn2008 was less frequent (12.9%). Isolates harboring the blaOXA-143-like gene showed the blaOXA-253-like variant. A polyclonal profile was observed among the A. baumannii isolates. The presence of the international clonal complexes CC113/79, CC109/1, CC110/25, and CC103/15 was detected, with prevalence of CC113/79 (38.8%). This study provides essential information to understand the antimicrobial resistance patterns of A. baumannii and can be used to strengthen infection control measures in our hospital. Also, the study reinforces the urgent need to develop stewardship programs to avoid the spread and potential outbreaks by this pathogen.
Introduction
One of the most problematic microorganisms globally disseminated in hospital settings is multidrug-resistant (MDR) Acinetobacter baumannii. 1 Bloodstream infections caused by A. baumannii are responsible for increasing morbidity and mortality rates and demanding considerable higher hospital costs. 2 The risk factors associated with MDR A. baumannii infections include antibiotic exposure, invasive devices, intensive care unit (ICU) stay, and severity of illness.2,3 In 2017, the World Health Organization released a priority list of pathogens threatening human health and classified A. baumannii as the top critical pathogen for research and development of new antimicrobials. 4
Carbapenems are the frontline choices for the treatment of MDR A. baumannii infections. 1 The emergence of carbapenem-resistant isolates is a challenge for treatment because the last antimicrobial resources include polymyxins and tigecycline.5,6 The carbapenem-hydrolyzing class D β-lactamases (CHDL) blaOXA-23-like, blaOXA-24-like, blaOXA-58-like, blaOXA-143-like, and blaOXA-235-like are the frequent cause of carbapenem resistance around the world in A. baumannii. 7 In Brazil, blaOXA-23-like is the prevalent CHDL disseminated in the hospitals. 7 This gene was described as inserted in transposons, including Tn2006, Tn2007, Tn2008, and Tn2009. 8 Generally, upstream blaOXA-23-like, there is ISAba1 (Insertion Sequence A. baumannii 1) acting as strong promoter and causing significant increase of expression of blaOXA-23-like. 9
The A. baumannii ability to acquire genetic resistance determinants is one of the characteristics strongly associated with the successful adaptation of international epidemic lineages. 7 Multilocus sequence typing schemes of the University of Oxford (UO) and Institut Pasteur (IP) for A. baumannii having been applied to evaluate the global lineage trends. To date, some of the internationally clonal complexes (UO/IP) related to spread in Brazilian hospitals are CC113/79, CC109/1, CC110/25, CC103/15, and CC118/2. 10 Clonal and antimicrobial resistance patterns are essential to understand the outstanding dissemination of this pathogen in hospitals across the world.
Hence, the aim of this study was to analyze the antimicrobial susceptibility profile, antimicrobial resistance genes, genetic context of blaOXA-23-like, clonal relatedness, and internationally clonal complexes of MDR A. baumannii isolated from bloodstream infections at a tertiary hospital in South of Brazil.
Materials and Methods
Isolate collection, study setting, and ethics statement
This study evaluated a collection of 103 nonduplicate MDR A. baumannii isolated over 10 years (November 2006 to December 2016) at the Clinical Microbiology Division of Hospital Universitário de Londrina (HU). The clinical microbiology laboratory processes specimens from patients attended in the HU and Ambulatório de Especialidades do HU (HU-AEHU), a complex of two public hospitals belonging to Universidade Estadual de Londrina, located in the Londrina city, Paraná State, Southern Brazil. The HU is the major tertiary hospital of Northern region of Paraná State, has 313 beds, and attends patients of Londrina region and more than 200 surrounding towns. The isolates were recovered from bloodstream of inpatients of ICUs (34.0%), wards (24.3%), emergency (22.3%), burn unit (17.5%), and neonatology care unit (1.9%) as follows: 1 isolate of 2006, 6 of 2007, 1 of 2008, 1 of 2009, 3 of 2010, 13 of 2011, 6 of 2012, 8 of 2013, 11 of 2014, 26 of 2015, and 27 of 2016. The clinical data analyzed included patient gender, age, admitted unit, duration of hospitalization, and outcome. This study was approved by the Research Ethics Committee (REC), Health Sciences Center, Universidade Estadual de Londrina (Protocol No. 14490/2009). Informed consent was waivered by the REC since the study was observational and patient care was not influenced.
Bacterial identification
The clinical isolates were identified by conventional biochemical tests and by automatized systems MicroScan/Siemens® (Beckman Coulter, Inc., Indianapolis, IN), BD Phoenix™ (Becton, Dickinson and Company, Franklin Lakes, NJ), or Vitek2® (bioMérieux, Craponne, France). The identification of the isolates was performed by amplification of blaOXA-51-like 11 and species-specific of rpoB 12 for A. baumannii.
Antimicrobial susceptibility testing
Antimicrobial susceptibility assays were performed by disk-diffusion method and automated systems according to the Clinical and Laboratory Standards Institute (CLSI) instructions 13 to the following antimicrobials: amikacin, gentamicin, ciprofloxacin, levofloxacin, trimethoprim-sulfamethoxazole, tetracycline, piperacillin-tazobactam, ampicillin-sulbactam, cefotaxime, ceftazidime, cefepime, imipenem, and meropenem.
Minimum inhibitory concentration (MIC) determination by broth microdilution method was performed according to guidelines recommended by the CLSI 14 to detect susceptibility to ceftazidime, imipenem, meropenem, colistin, polymyxin B, and tigecycline. The results were interpreted using CLSI breakpoints 13 for all the tested antimicrobials, except for tigecycline in which the criteria for interpretation were adapted from the Food and Drug Administration (FDA) breakpoints 15 for Enterobacteriaceae (susceptible ≤2 μg/mL; intermediate 4 μg/mL; resistant ≥8 μg/mL).
Resistance classification of isolates in MDR, extensively drug-resistant (XDR), and pandrug-resistant (PDR) were defined by guidelines established for Acinetobacter spp by Magiorakos et al. 16
Phenotypic detection of carbapenemases
Carbapenemase production was assessed with the CarbAcineto NP test. 17 The result was considered positive when the color of suspension test changed from red to orange or red to yellow.
Screening of antimicrobial resistance genes
Genomic DNA was extracted using boiling method. 18 Polymerase chain reaction (PCR) assays were applied for the detection of the β-lactamases encoding genes blaOXA-23-like, blaOXA-24-like, blaOXA-51-like, blaOXA-58-like, blaOXA-143-like,19,20 blaOXA-48, blaKPC, blaNDM, 21 blaSPM-1, blaSIM-1, blaVIM, blaIMP, blaGIM, 22 blaGES 23 ; colistin acquired resistance mcr-1, 24 and quinolone resistance determinants qnrA, qnrB, qnrC, qnrS, and qnrVc. 25 For all PCRs, the Top Taq Master Mix (Qiagen, Germantown, MD) was used following the manufacturer's instructions.
The sequencing of blaOXA-143-like amplicons was performed with primers designed in this study. PCR amplification of the 762 bp amplicon was performed using HotStar High Fidelity Taq Polymerase (Qiagen) according to the manufacturer's instructions using 10 pmol of the primers OXA-143-F 5′-CAGCATTTCTACTCTACTTTC-3′ and OXA-143-R 5′-TCATTACGAATAGAACCAG-3′ in the following conditions: initial denaturation at 95°C for 5 minutes, followed by 30 cycles of 94°C for 30 seconds, 50°C for 30 seconds, 72°C for 1 minute, and final extension at 72°C for 5 minutes.
Genetic context of blaOXA-23-like
The isolates harboring blaOXA-23-like were assessed for the occurrence of Tn2006, Tn2007, Tn2008, and Tn2009 using PCR mapping, as previously described. 8 PCR assays were performed using Top Taq Master Mix (Qiagen).
DNA sequencing
Amplicons of blaOXA-143-like and blaOXA-23-like genetic context were sequenced. The amplicons were purified using PureLink PCR Purification Kit (Invitrogen, Waltham, MA). Sequencing reactions were prepared with BigDye Terminator Kit (Applied Biosystems, Foster City, CA) and carried out in the ABI 3500 × L Genetic Analyzer (Applied Biosystems) machine. Chromatogram results were confirmed with Bioedit v7.0.5 (Ibis Therapeutics, Carlsbad, CA), and DNA sequences were analyzed using the BLAST algorithm in the NCBI GenBank database.
Enterobacterial repetitive intergenic consensus typing
Molecular typing of the isolates was performed by enterobacterial repetitive intergenic consensus (ERIC)-PCR according to the protocol previously described, 26 with some modifications. Briefly, the DNA was extracted by boiling method 18 and quantified using NanoDrop™ Lite Spectrophotometer (Thermo Fisher Scientific, Waltham, MA). The amplification reaction mixtures were performed using Top Taq Master Mix (Qiagen) and 100 ng of DNA. The PCR conditions were initial denaturation of 95°C for 2 minutes, followed by 35 cycles of 90°C for 30 seconds, 40°C for 1 minute, 65°C for 8 minutes, and final extension of 65°C for 5 minutes. The amplicons were separated by 2% agarose gel, stained with 0.5 μg/mL ethidium bromide, and visualized by exposure to ultraviolet light (260 nm) in the LPIX transilluminator (Loccus Biotecnologia, Cotia, SP, Brazil). The fragments pattern of each sample was analyzed with BioNumerics software (Applied Maths, Sint-Martens-Latem, Gante, Belgium) using unweighted pair group method with arithmetic averages (UPGMA) for clustering and Dice coefficient with 2.0% tolerance for the similarity of the isolates. The cutoff value of 90% was applied for the isolates clustering.
Trilocus sequence-based (3LST) multiplex-PCR typing
The presence of the international MLST clonal complexes CC113/79, CC109/1, CC110/25, CC103/15, and CC118/2 was investigated using the protocol previously developed. 10
Statistical analysis
Data analysis of the categorical variables was performed using the Statistical Package for the Social Sciences, version 22.0 (SPSS, Inc., Armonk, NY). The Fisher's exact test was used to compare some categorical variables, and p-values <0.05 were considered statistically significant. The association of carbapenemase production, blaOXA-23-like gene, and epidemic clonal complex with XDR and MDR phenotype of A. baumannii was evaluated by calculation of the odds ratio (OR) with a confidence interval (CI) of 95%. A positive correlation was indicated with an OR value >1.0.
Results
Bacterial isolates and clinical characteristics
A total of 103 nonduplicate MDR A. baumannii isolated from bloodstream were recovered in the Clinical Microbiology Division of HU from the period November 2006 to December 2016. All the isolates were identified as A. baumannii by the positive amplification of blaOXA-51-like and rpoB. Of the 103 patients, the median age was 60 years ranging from 16 days to 94 years, and the infections affected more male patients (70.9%). The medium duration of hospitalization was 28 days. Intra-hospital mortality (81.6%) was observed in the majority of the patients.
Antimicrobial resistance patterns
The antimicrobial susceptibility profiles of the 103 A. baumannii isolates are presented in Table 1. Although all the isolates were initially identified as MDR, most of the isolates were correctly classified as XDR (78.6%) followed by MDR (21.4%). None of the isolates was classified as PDR. The MIC50 and MIC90 values of ceftazidime, imipenem, meropenem, polymyxin B, colistin, and tigecycline are shown in Table 2.
Antimicrobial Susceptibility Profile of the Acinetobacter baumannii Isolated from Bloodstream
Minimum Inhibitory Concentration of Ceftazidime, Carbapenems, Polymyxins, and Tigecycline for A. baumannii Isolates
MIC50 minimum inhibitory concentration to inhibit 50% of the isolates.
MIC90 minimum inhibitory concentration to inhibit 90% of the isolates.
Phenotypic detection of carbapenemases
Carbapenemase production evaluated by CarbAcineto NP test was found in 95 (92.2%) isolates, whereas only 8 (7.8%) were negative. Statistical significance association between carbapenemase production and XDR phenotype was observed (Table 3).
Association Between Carbapenemase Production, blaOXA-23-like Gene, and Epidemic Clonal Complex with Extensively Drug-Resistant and Multidrug-Resistant Phenotype of A. baumannii
Fisher's exact test.
XDR, extensively drug-resistant; MDR, multidrug resistant; OR, odds ratio; CI, confidence interval.
Antimicrobial determinants of resistance screening
The antimicrobial resistance genes blaOXA-24-like, blaOXA-58-like, blaOXA-48, blaKPC, blaNDM, blaSPM-1, blaSIM-1, blaVIM, blaIMP, blaGIM, blaGES, mcr-1, qnrA, qnrB, qnrC, qnrS, and qnrVc were not detected in none of the isolates. Positive results were only detected to blaOXA-51-like, the CHDL blaOXA-23-like, and blaOXA-143-like. All A. baumannii were positive for blaOXA-51-like; moreover, every carbapenem-resistant A. baumannii were positive either for blaOXA-23-like or for blaOXA-143-like. Among the 95 carbapenem-resistant A. baumannii, the majority harbored blaOXA-23-like (n = 93; 97.9%). Statistical association between isolates harboring blaOXA-23-like and XDR phenotype was observed (Table 3). Only two isolates harbored blaOXA-143-like (2.1%). Sequencing analysis identified these two isolates being the blaOXA-253 variant, which were classified as XDR, belonged to the same cluster and CC110/25, and were recovered in 2011 and 2016 from inpatients at the ICU and burn unit, respectively.
Genetic context of blaOXA-23-like
Sequencing analysis detected the presence of two different transposons harboring blaOXA-23-like. The Tn2006 harboring isolates (n = 80) was detected every year analyzed, except for 2006, and it was detected in 86.0% of the isolates. While Tn2008 harboring isolates was detected mainly before 2012 (n = 8), and it was found in 12.9% (n = 12) of the isolates. Only one (1.1%) isolate was not positive for Tn2006, Tn2007, Tn2008, or Tn2009.
Molecular typing
The dendrogram representing the ERIC-PCR profiles of the 103 bloodstream A. baumannii isolates showing the year of isolation, resistance phenotype, and clonal complex is shown in Supplementary Fig. S1. The dendrogram analysis revealed 17 clusters, in which 6 were dominant, representing 89.3% of all isolates. The main clusters were H (24.3%), D (20.4%), O (13.6%), G (11.6%), I (11.6%), and M (7.8%), respectively. The other 11 clusters (10.7%) had sporadic detection. The clinical, phenotypic, and molecular characteristics of the clusters H and D are demonstrated in Figs. 1 and 2, respectively.
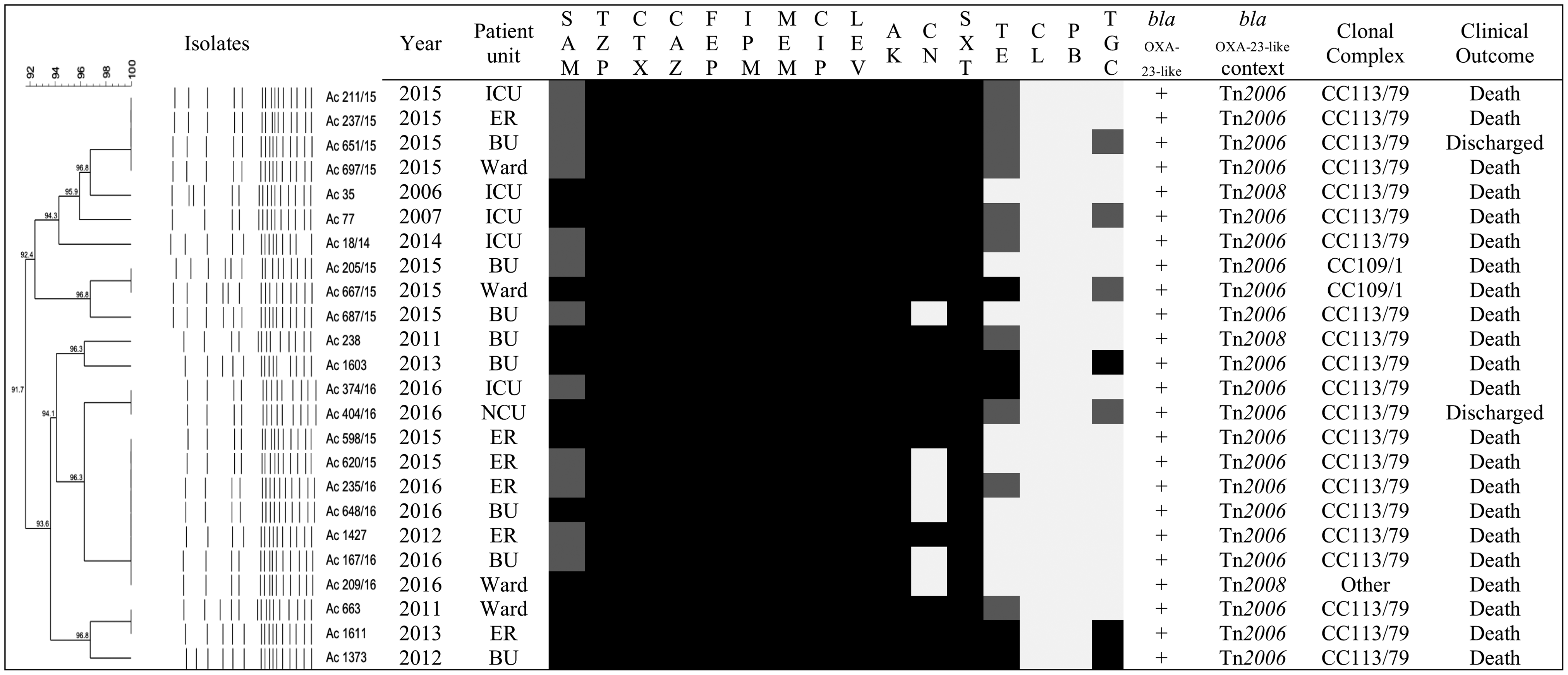
Clinical, phenotypic, and molecular characteristics of Acinetobacter baumannii cluster H. ICU, intensive care unit; BU, burn unit; ER, emergency room; NCU, neonatology care unit; SAM, ampicillin-sulbactam; TZP, piperacillin-tazobactam; CTX, cefotaxime; CAZ, ceftazidime; FEP, cefepime; IPM, imipenem; MEM, meropenem; CIP, ciprofloxacin; LEV, levofloxacin; AK, amikacin; CN, gentamicin; SXT, trimethoprim-sulfamethoxazole; CL, colistin; PB, polymyxin B; TE, tetracycline; TGC, tigecycline. Light gray square indicates susceptible; dark gray square indicates intermediate; black square indicates resistant. −, Not detected; +, detected.
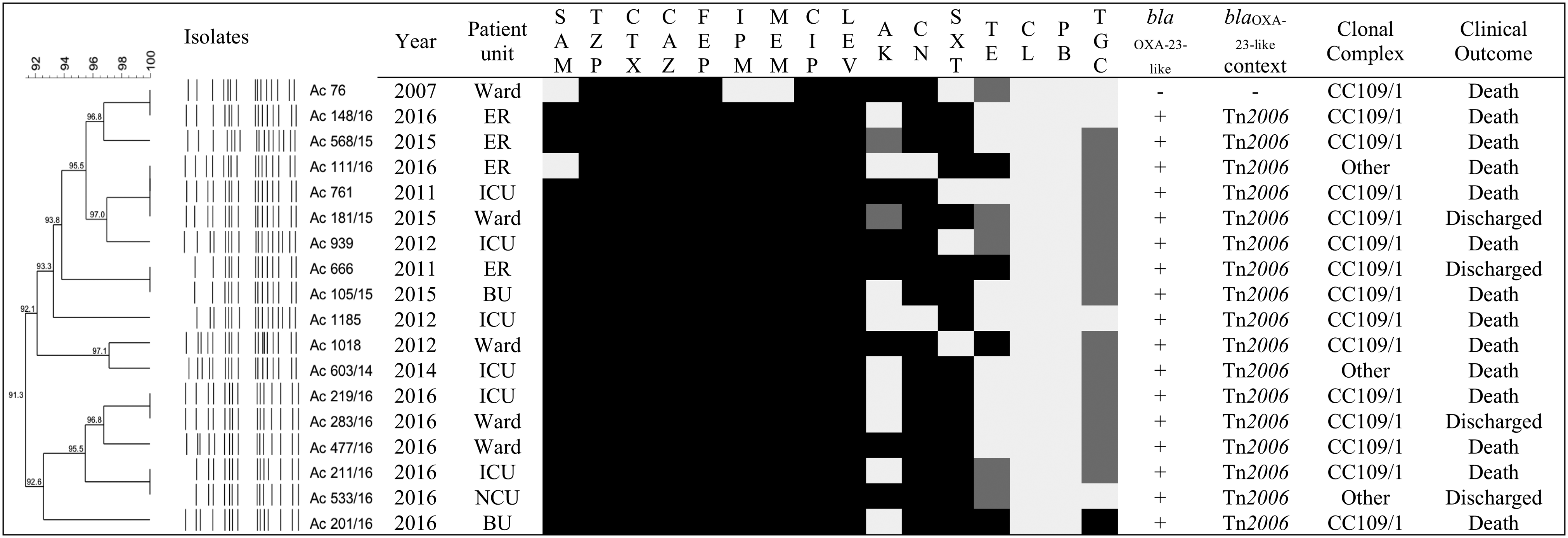
Clinical, phenotypic, and molecular characteristics of A. baumannii cluster D. Light gray square indicates susceptible; dark gray square indicates intermediate; black square indicates resistant. –, Not detected; +, detected.
Nearly all isolates (89.3%) were identified as being one of the international clonal complexes CC113/79 (38.8%), CC110/25 (20.4%), CC109/1 (19.4%), and CC103/15 (10.7%). The XDR phenotype was observed in the majority of the international clonal complexes CC113/79 (77.5%), CC110/25 (100.0%), CC109/1 (80.0%), except for CC103/15 with the prevalence of MDR phenotype (54.5%). However, no statistical association was observed between international CC and XDR phenotype (Table 3).
Discussion
A. baumannii is one of the most successful pathogens in hospital settings associated with worldwide nosocomial outbreaks.12,27 One of the reasons is the accumulation of several antimicrobial resistance mechanisms.7,27 In Brazil, A. baumannii is the fourth most frequent microorganism causing bloodstream infections related to central venous catheter. 28 Bacteremia caused by A. baumannii is a major concern for patients and physicians because it affects the clinical outcome and is associated with considerable mortality, higher than 40.0%. 2 In HU, A. baumannii is the second microorganism with highest mortality (18.5%) among the gram-negative bacilli infections. 29 Due to the importance and urgent need of molecular and epidemiology surveillance of this pathogen in HU, we studied a total of 103 MDR A. baumannii isolated from bloodstream of inpatients over 10 years.
Several risk factors are associated with A. baumannii infections, which include male gender, older age, duration of hospitalization, and ICU stay.1,3,5,30 In fact, our study demonstrated that the frequency of A. baumannii from bloodstream was higher in male patients, with age ≥61 years, and the median hospitalization was 28 days. Moreover, most of the isolates were recovered from patients located in the ICU, in accordance with similar studies reported.1–3,30 Even though epidemiological parameters were not evaluated, and mortality associated with A. baumannii infections could not be performed, higher intra-hospital death rates (81.6%) were observed in this study compared with similar studies developed in Israel and China.2,31
The genetic plasticity of A. baumannii enables this pathogen to adapt to the hospital environment and survive to selective pressure, contributing to acquisition of multiple mechanisms of resistance.5,7 Currently, carbapenem-resistant MDR A. baumannii is a challenge due to generating limitation of clinical treatment, leaving generally only few therapeutic options such as polymyxins and tigecycline.5,6,32 The resistance classification of the isolates in this study revealed alarming rates of XDR phenotype, higher than other study in Brazil. 32 The majority of antimicrobials tested presented high antimicrobial non-susceptibility rates similar to that observed in a Brazilian collection of carbapenem-resistant isolates. 33 Lower antimicrobial rates were seen only for tigecycline and polymyxins. Polymyxins resistance rates are also in accordance with other studies in Brazil.32,34 Nevertheless, tigecycline non-susceptibility rates were higher in this study compared with other studies reported in Latin America, including Brazil.5,32 Thus, the advance of antimicrobial resistance in XDR A. baumannii is concerning to a future of untreatable infections, and stewardship programs are crucial to manage and conserve these last treatment options.
In the latest report developed by Brazilian Health Surveillance Agency, A. baumannii represents the gram-negative bacilli with highest rates of carbapenem resistance in bloodstream infections related to central venous catheter from 2012 to 2016. 28 In this study, carbapenemase production was observed in 92.2% of the isolates, significantly associated with XDR phenotype (p < 0.005). The CarbAcineto NP test has been described as more accurate with higher sensibility and specificity for carbapenemases, mainly CHDL, in A. baumannii isolates, demonstrating sensitivity of 94.7% and specificity of 100.0%. 17
A. baumannii isolates harboring blaOXA-23-like are the leading cause of carbapenem resistance.7,27 In this study, all carbapenem-resistant isolates harbored one acquired CHDL, with major preponderance of blaOXA-23-like (97.9%); furthermore, this resistant determinant was also significantly associated with XDR isolates (p < 0.005). Similar results in Brazil have shown that blaOXA-23-like was prevalent (91.0–100%) in the isolates.35,36 Importantly, a study conducted in HU between 2006 and 2011 showed that blaOXA-23-like was detected in 68.0% of A. baumannii carbapenem-resistant isolates. 37 This increase in frequency of blaOXA-23-like in our study as well as in Brazil7,36 is extremely alarming not only because of the inefficacy of β-lactam antibiotics as a treatment option but also due to the association with XDR phenotype, restricting even more the antibiotic options available for treatment.
Globally, Tn2006 is the genetic environment of blaOXA-23-like most reported, is responsible for mobilization in the genome, and also is related to replicative transposition, resulting in multiple copies of blaOXA-23-like in the A. baumannii genome. 38 In addition, the Tn2006 is flanked in opposite orientation by ISAba1, which might contribute to the increase of expression of this gene resulting in the higher carbapenem MIC values observed for resistant isolates.5,9,27,38 In accordance with the global prevalence, 38 the Tn2006 (86.0%) was the mobile genetic element predominant among the blaOXA-23-like isolates in HU. The Tn2008 (12.9%) was the second genetic context detected, and it is also characterized by the ISAba1 only upstream blaOXA-23-like, thereby enhancing the upregulation of this gene and increasing its expression.7,38
The other acquired CHDL found in A. baumannii at HU is blaOXA-143-like, which was first detected in Brazil in 2004. 39 So far in this country, the detected blaOXA-143-like variants were blaOXA-143, 39 blaOXA-231, 37 and blaOXA-253. 40 The blaOXA-231 variant was also first described in an isolate recovered from urine of an inpatient of HU in 2007, 37 and surprisingly, no additional blaOXA-231 variant has been detected among the isolates during the period evaluated. Noteworthy, in this study, two blaOXA-253 harboring A. baumannii isolates were detected for the first time in South of Brazil. This resistance determinant was early reported in Honduras, 41 and in Brazil detected to date in Belo Horizonte 40 and Recife. 42 Interestingly, the XDR phenotype of the blaOXA-253 harboring isolates in this study was also observed in 25 A. baumannii clinical isolates in Recife 42 ; hence, controlling the potential spread of this high-risk pathogen is essential to avoid further dissemination in other Brazilian cities.
The clonal relatedness and evaluation of international clonal complexes are essential to establish an evolution of possible outstanding epidemic clones and guidance of a route of transmission of A. baumannii isolates, providing infection control knowledge to improve the hygiene policies in critical wards and avoiding cross-transmission to eradicate A. baumannii. Silbert et al. 26 reported ERIC-PCR as a reliable typing method for A. baumannii in local purposes. Several studies in a worldwide scale demonstrate outbreaks of carbapenem-resistant A. baumannii caused by clonally related isolates.8,27,35,42 However, our findings demonstrated a polyclonal diversity of A. baumannii among the isolates in the 10 years analyzed. The clusters H (24.3%) and D (20.4%) represented the majority of the isolates. Both clusters were characterized by isolates predominantly recovered in all years of study, presented similar resistance profile, harbored mostly blaOXA-23-like and Tn2006 genetic context, and patients with higher death rates. Clones H and D also demonstrated long-term persistence in all hospital wards. Regarding the CC, cluster H had a significant number of isolates belonging to CC113/79 and cluster D predominant belonging to CC109/1. The patterns observed suggest the successful adaptation of these clusters along the years in HU, and their dissemination might have occurred by transmission by medical staff, contaminated equipment, and patient transfer. 43 Endemic clusters with reappearance over the years were also detected as clusters O, G, I, and M. These clusters require constant evaluation of their dissemination because their persistence indicates adaptation in the hospital environment and represents a risk of future outbreaks.
The 3LST multiplex-PCR has been reported as a trustworthy method for molecular evaluation of A. baumannii international epidemic clones.10,44 In South America, dissemination of blaOXA-23-like harboring A. baumannii is associated with the international epidemic clones 113/79, 109/1, 110/25, and 103/15,10,34,44,45 and all these clonal complexes were detected in isolates from HU. These findings are consistent that blaOXA-23-like is not restricted to a main CC, 34 which is not surprising due to its acquired mechanism of resistance. Additionally, our results demonstrate that HU has mainly disseminated epidemic CC globally widespread. Although the CC113/79 was predominant among the isolates, the CC110/25, CC109/1, and CC103/15 should be monitored to determine their evolution. The clonal complex CC113/79 has been related to MDR phenotype. 34 However, most of the CC113/79 isolates in this study presented an XDR phenotype. These findings are concerning to the emergence of this phenotype in Brazilian hospitals. Also, A. baumannii harboring blaOXA-253 was detected in CC110/25, which was observed in a previous report. 42 Although no association between international epidemic clones and XDR phenotype was noticed (p > 0.005), the advances of internationally epidemic XDR clones harboring important antibiotic genes are alarming to the emergence of future PDR isolates.
Epidemiology measures such as antimicrobial stewardship and infection control continuously need to be applied and reinforced to contain the spread of these successful clinical isolates. 43 These measures are monitored by the Infection Control Commission (ICC) in our hospital. The main objectives of the ICC are implementing strategies of infection control such as hygiene policies, instructing health professionals, conducting patient isolation, and informing patient contact precaution for the professionals and visitors. Moreover, the ICC is responsible for controlling the use of antimicrobials and managing the treatment of concerning patients with MDR, XDR, or even PDR bacteria. Other important liability of the ICC is surveillance antimicrobial susceptibility patterns of important pathogens involved in outbreaks or epidemic in our hospital as A. baumannii. Although these restricted measures and infection control interventions are performed in our hospital, the ICC reported that A. baumannii maintain the infection rates and antimicrobial resistance patterns during the years of this study (personal data). The inefficacy of strategies to reduce infections by A. baumannii reinforces this pathogen as an extremely problematic in hospital settings as also noticed in another study in Greece. 46
In conclusion, to the best of our knowledge, this is the first study at HU to evaluate the temporal evolution of A. baumannii by performing phenotypic and molecular characterization of MDR and XDR isolates. Here, we report extremely high rates of XDR isolates and alarming rates of polymyxin B, colistin, and tigecycline resistance. Furthermore, our study has shown that carbapenemase production plays an important role in carbapenem resistance with high prevalence of blaOXA-23-like, mainly inserted in Tn2006, in the 10 years analyzed. It was also detected, for the first time, in HU and South of Brazil isolates of XDR A. baumannii harboring blaOXA-253 belonging to CC110/25. Interestingly, our study has demonstrated that the epidemic international clonal complexes 113/79, 109/1, 110/25, and 103/15 were detected in most of the isolates, thus representing a troublesome pathogen responsible for potential outbreaks of MDR and XDR A. baumannii in HU. Finally, we emphasize the importance of constant molecular and epidemiological studies to evaluate and establish control effective antimicrobial resistance programs to avoid the spread of new resistance mechanisms and the dissemination of successful high-risk pathogens.
Footnotes
Acknowledgments
We would like to thank Ana Cristina Gales (Universidade Federal de São Paulo) and Renata Cristina Picão (Universidade Federal do Rio de Janeiro) for kindly providing the control strains. This study was supported by grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES)-Finance Code 001, Fundação Araucária, and Programa de Pesquisa para o SUS: Gestão compartilhada em saúde (PPSUS). P.R. was supported by a student scholarship from CNPq (grant No.133021/2016-5). R.L.P. and S.B.D.P.-P. were supported by a student scholarship from CAPES. L.S.F. was supported by a student scholarship from Fundação Araucária. This study is part of the MSc dissertation of P.R.
Ethical Approval
Approved by the local ethics committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Disclosure Statement
The authors declare that they have no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.