
Abstract
In July 2018, a Klebsiella pneumoniae carbapenemase (KPC)-producing Escherichia coli ST131 was isolated from a patient admitted to the Vascular Surgery Unit of the main hospital of Molise region, Central Italy. Sequencing and alignment with the available sequences revealed that the isolate harbored the KPC-2 variant and TEM-1 beta-lactamase. This observation raises great concerns about the spread of carbapenem resistance in national and local settings with high endemicity level of KPC in K. pneumoniae, and underlines the importance of strengthening a proactive surveillance.
Case Description
In July 2018, the local surveillance system was triggered by the isolation of an “Alert Organism” at the “Antonio Cardarelli” hospital in Molise region, Central Italy, which was identified as a carbapenem-resistant Escherichia coli showing a “Klebsiella pneumoniae carbapenemase” (KPC) phenotype. This E. coli was recovered from urine culture of an 84-year-old Italian male patient with an ongoing urinary tract infection, who has admitted to the Vascular Surgery Unit. As consequence of the alert, the patient was isolated in a single room, and nursing staff was encouraged to perform increased hand hygiene, and infection control measures, ensuring patient areas and environment cleaning and proper disinfection, were adopted. The patient died shortly thereafter of multiorgan failure.
We report in this study the first isolation of a KPC-producing E. coli in Molise region, and describe its biomolecular characteristics.
Laboratory Investigations
The E. coli isolate was tested by the hospital microbiology laboratory for antimicrobial susceptibility testing by using BD Phoenix™ Automated Microbiology System (Becton-Dickinson Diagnostic Systems, Sparks, MD), which is equipped with software suitable for results interpretation using the clinical breakpoints as established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST). 1 In particular, the system panels include 20 and 22 antibiotics with minimum inhibitory concentration for gram-negative and for gram-positive microrganisms, respectively. 2 Indeed, the E. coli isolate was tested for 20 antimicrobials, and the susceptibility status was classified as susceptible, S; susceptible, increased exposure, I; and resistant, R based on the updated EUCAST breakpoints. 1 In the hospital, the matrix-assisted laser desorption ionization-time of flight system is also available for a rapid bacterial identification.
This E. coli showed a multidrug resistance (MDR) profile, with a resistant phenotype for 14 out of 20 (70%) tested antimicrobials, including resistance to carbapenems, particularly to ertapenem, and a susceptible, increased exposure profile for both imipenem and meropenem (formerly reported as intermediate). Furthermore, the E. coli isolate was resistant to: amoxicillin-clavulanate and piperacillin-tazobactam (combinations of penicillins, including beta-lactamase inhibitors); ampicillin (penicillins with extended spectrum); cephalexin (first-generation cephalosporins); cefuroxime (second-generation cephalosporins); ceftazidime, cefixime and cefotaxime (third-generation cephalosporins); cefepime (fourth-generation cephalosporins); gentamicin and tobramycin (other aminoglycosides); ciprofloxacin (fluoroquinolones); and tigecycline (tetracyclines). The isolate showed susceptibility only to trimethoprim-sulfametoxazol (combinations of sulfonamides and trimethoprim, including derivatives); trimethoprim (trimethoprim and derivatives); fosfomycin (other antibacterials); nitrofurantoin (nitrofuran derivatives).
There was no evidence for previous treatment with carbapenems for the patient.
The presence of KPC (class A carbapenemase)-encoding gene was confirmed by singleplex PCR assay, as previously reported. 3 Sanger sequencing using both primers for the amplification 4 and following alignment through Basic Local Alignment Search Tool (https://blast.ncbi.nlm.nih.gov/Blast.cgi) revealed that it was KPC-2 allele. We further explored by singleplex PCRs for the carbapenemases VIM, IMP, and NDM-1 (class B metallo-beta-lactamases), and oxacinillase OXA-48-lixe (class D) using oligonucleotides previously designed 4 and specific reaction conditions, 3 as well as for TEM, CTX-M, and SHV beta-lactamases. 5 In addition to the KPC-2 enzyme, the E. coli harbored TEM-1 beta-lactamase (Fig. 1), as revealed through Sanger sequencing of TEM amplicon with both primers for the amplification 5 and BLAST alignment (https://blast.ncbi.nlm.nih.gov/Blast.cgi). None of the other tested enzymes was detected. The multilocus sequence typing scheme 6 assigned the isolate to Sequence Type ST131.
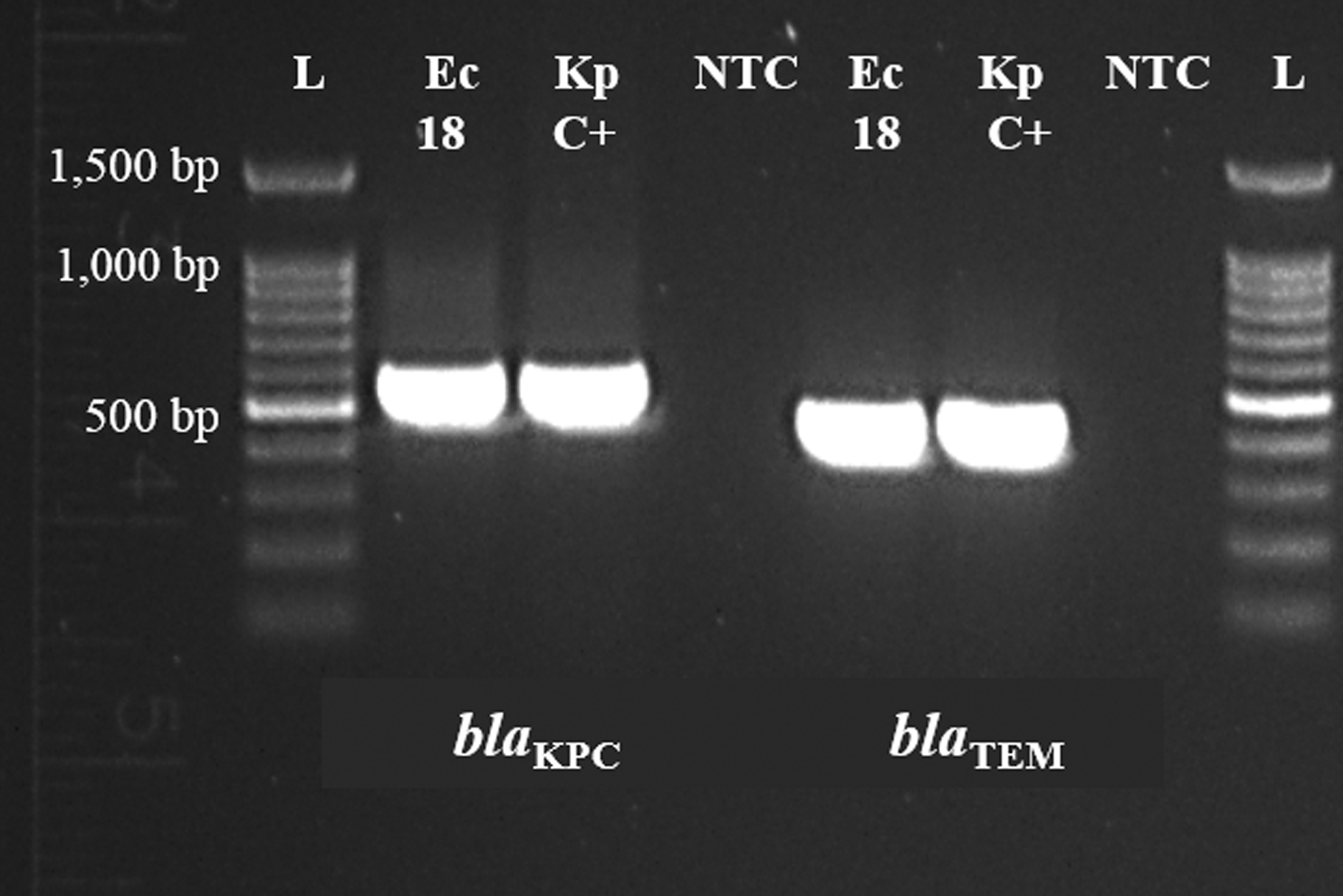
Detection of blaKPC and blaTEM in the Escherichia coli strain isolated on July 2018, Molise region, Central Italy. L: ladder 100 bp; Ec18: E. coli isolated in Molise region on July 2018 carrying blaKPC (538 bp); Kp C+: KPC-producing K. pneumoniae isolated in the same hospital, used as internal positive control; NTC: nontemplate control; Ec18: E. coli isolated in Molise region on July 2018 carrying blaTEM (445 bp); Kp C+: TEM-producing K. pneumoniae isolated in the same hospital, used as internal positive control. KPC, Klebsiella pneumoniae carbapenemase; NTC, no template control.
Discussion
Infections due to MDR Enterobacteriaceae, especially K. pneumoniae and E. coli, represent a serious threat to global public health. In particular, carbapenem resistance is the utmost concern, which is mostly conferred by plasmid-encoded KPC carbapenemase.
The KPC enzyme is usually associated with K. pneumoniae infections in hospital settings, 7 and occasionally observed in other Enterobacteriaceae and Pseudomonas aeruginosa. 8 The first KPC-2 producer was a K. pneumoniae strain isolated in the United States, and unlike other variants, KPC-2 together with KPC-3 have rapidly disseminated to endemic levels in the United States, Greece, Israel, China, and Latin America, as well as in Italy. 7 Epidemiological evidences underscored that the epidemic spread of the K. pneumoniae ST258 lineage has significantly contributed to the global dissemination of blaKPC-2 and blaKPC-3,7,8 as well in other species.
KPC-producing E. coli strains, although globally distributed, are rare, and only described for countries with high prevalence of this carbapenemase in K. pneumoniae, and Italy is characterized with the highest rates in Europe. 8 After the first isolation of KPC-producing E. coli strain, further cases were reported elsewhere, including evidence for the direct transfer of blaKPC plasmid from K. pneumoniae to E. coli. 9
In Europe, the first isolation of E. coli KPC-producing strain was reported in France in a patient initially admitted to a hospital in Israel. 10 Afterward, it was notified in Padua, Northern Italy (Table 1) as a consequence of KPC-2 allele transfer from K. pneumoniae strain to E. coli in the same patient. 11 Isolations of carbapenem-resistant KPC-producing E. coli strains from health care setting have been reported in Italy,12–17 as well by ST131 E. coli KPC-2 and KPC-8 positive in nursing care homes, and the emergence of ST3948 associated with blaKPC-3 (Table 1). 18 Furthermore, the “European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE)” conducted between 2013 and 201419 allowed collecting consistent data on K. pneumoniae and E. coli incidence in 455 hospitals with diagnostic capabilities in Turkey, Israel, and 34 European countries, including 22 hospitals in Italy. Overall, 37% and 19% carbapenemase-producing K. pneumoniae and E. coli were detected, respectively, most often from south and southeast Europe. As expected, KPC prevalence was higher in K. pneumoniae than E. coli (31.5% vs. 7.2%), and Italy showed the highest rate. At the European level, OXA-48-like was the most common (56%) carbapenemase in E. coli, followed by NDM (26%) and KPC (18%), which was only identified in E. coli from Israel (n = 6), Italy (4/5, 80%), Portugal (n = 2), Greece, and Cyprus (n = 1 each). 19
Reports of Thirty Klebsiella pneumoniae Carbapenemase-Producing Escherichia coli Isolated from Multiple Samples in Health Care Settings in Italy
NA, not available; ERT, ertapenem; IMP, imipenem; MER, meropenem; KPC, Klebsiella pneumoniae carbapenemase; I, intermediate; S, susceptible; R, resistant.
It has been reported that more than 60% of KPC-producing E. coli belong to ST131, which are probably responsible for the rapid spread of blaKPC in this bacterium,10,18 and a similar distribution is observed for Italy (Table 1). To date, the KPC-producing E. coli ST131 isolates are of significant concern, being considered a “successful” clinical strain with a global distribution,8,20 including Italy (Table 1). E. coli ST131 along with K. pneumoniae ST258 have extensively spread throughout the world due to hyperendemic properties, such as increased transmissibility, longer duration of infectiousness, and/or higher pathogenic potential compared with other lineages of the same species, 21 and are responsible for the rapid increase of antimicrobial resistance. 22 Since the first identification, E. coli ST131 has been strongly associated with fluoroquinolone resistance, and coresistance to aminoglycosides and trimethoprim-sulfamethoxazole, and alarmingly to carbapenems resistance. 23
E. coli ST131, causing a high proportion of urinary tract and bloodstream infections, 23 is also often associated with extended-spectrum beta lactamase (ESBLs) production, especially cefotaximases (CTX-M-15)22,24 that efficiently hydrolyze cefotaxime, and confer resistance to penicillins, extended-spectrum cephalosporins, and monobactams. 25 Although initially identified through its association with CTX-M-15, the geographical and temporal origin of ST131 ancestor is poorly understood; nonetheless, some events gained the acquisition of virulence-associated genes, followed by development of antibiotic resistance, both likely contributing to the successful ST131 global spreading. 26
E. coli ST131 has been also reported to occur without ESBLs, 24 as found in our study, where CTX-M was not detected. This finding was in agreement with other studies conducted in Italy. In fact, in Italy, the presence of CTX-M, as well as of SHV, in KPC-producing E. coli strains was assessed in all except one 17 study as reported in Table 1. However, data analysis underlined that CTX-M variants were only detected in three cases, and only one CTX-M-15 strain was of ST131. 15 The CTX-M-15 was further found in a strain of ST394, 9 and CTX-M-55 together with SHV-11 in a strain of ST457. 15 Indeed, since multiple studies have been performed on ESBL producers, the role of non-ESBL-producing E. coli ST131 could be underestimated. 27 Interestingly, the reviewed studies (Table 1) revealed a significant prevalence of the oxacillin-hydrolyzing beta-lactamase OXA-9 in Italian KPC-producing E. coli.11,14,18
The E. coli collected from our hospital also carried TEM-1, which hydrolyzes penicillin and first generation cephalosporins, in agreement with other Italian studies, which always found this enzyme when investigated in KPC-E. coli (Table 1). Currently, more than hundred TEM type beta-lactamases have been identified, and all with the exception of TEM-1 and TEM-2 are ESBLs.28,29 Remarkably, TEM-1 prevalence was estimated as of 90% among ampicillin-resistant E. coli isolates.28,30
In this scenario, the spread of carbapenem-resistant E. coli has critical implications in patient management and infection control compared to the most prevalent carbapenem-resistant Enterobacteriaceae (CRE), since E. coli can spread easily to the community. Considering the occurrence of infections due to E. coli ST131 and its capability for the gastrointestinal colonization, 20 the association between ST131 and blaKPC could have severe consequences for infection management, especially in elderly people with comorbidities who are at high risk for ST131 colonization. 18 To date, detailed information concerning the genetics of blaKPC in E. coli and the mechanisms by which these elements can spread are limited. Nevertheless, the increasing emergence of blaKPC in E. coli has been linked to multiple mechanisms, such as the global spread of genetically related strains, plasmid exchange with other Enterobacteriaceae and between lineage, and the transpositional events in the species. 31
Conclusions
Infections with CRE organisms, particularly when KPC-producing, are highly diffusive, and the treatment of a consequently high number of patients is critical, since an optimal therapy is not yet defined, and data on the clinical outcome are still scarce.
The first notification of an infection by a KPC-producing E. coli ST131 strain in Molise region, Central Italy, on July 2018 is noteworthy due to the general low isolation rate in health care settings compared to other CRE organisms, and to its antimicrobial resistance profile. Our findings further support the national epidemiological background, which is characterized by a sporadic occurrence of carbapenem-resistant KPC-2 and TEM-1 E. coli ST131 isolated in health care settings (Table 1), as reported in certain geographical areas (Fig. 2). This report underlines the urgent need to enhance awareness and strengthen education on hand hygiene and appropriate procedures among health care personnel, 32 principally considering that ST131 E. coli isolates are strictly pathogenic due to the spectrum of infections caused in both community and hospital settings, and the virulence-associated genes content.23,33
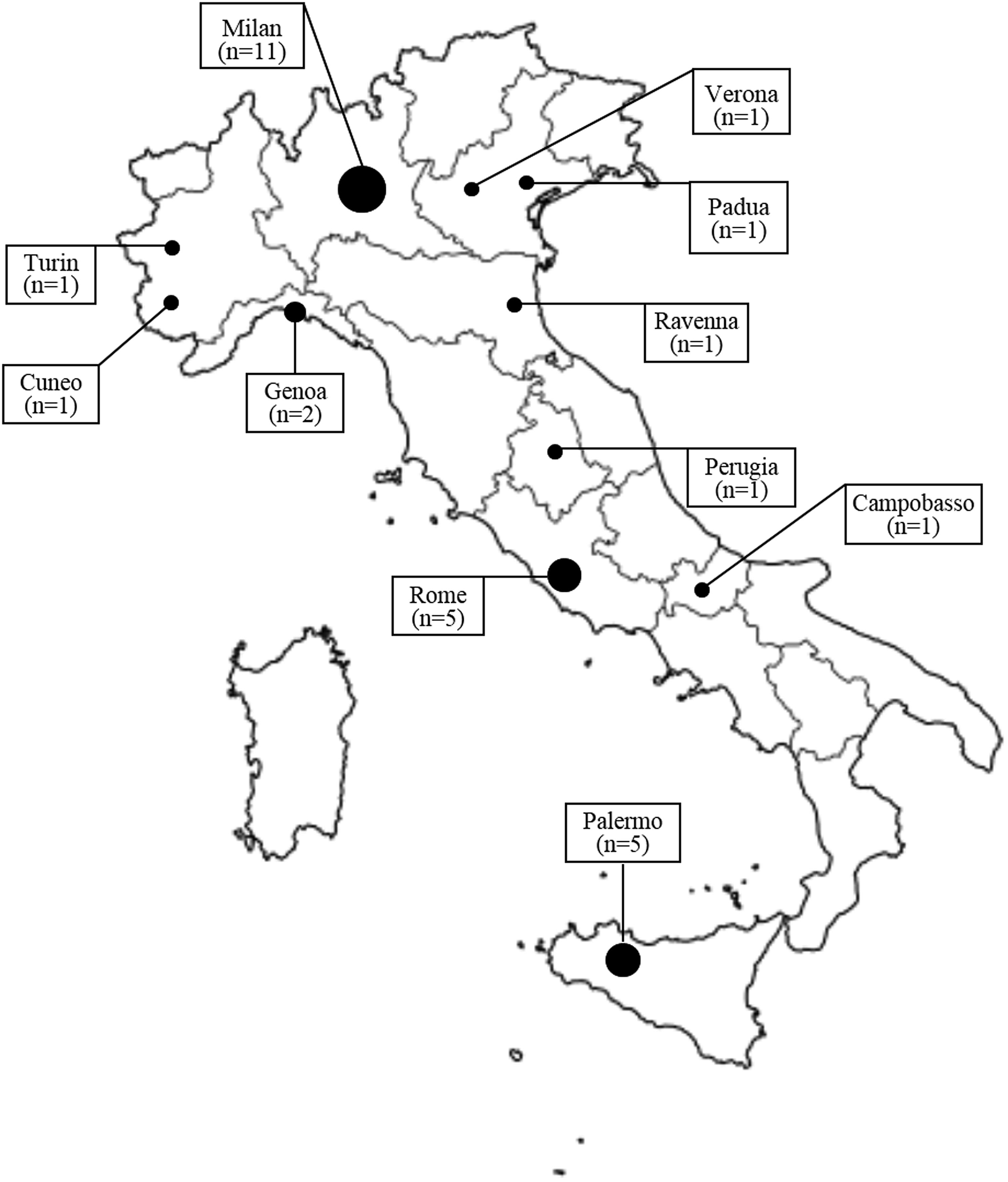
Geographical distribution of a total of 30 KPC-producing E. coli strains reported in Italy since 2010 to date.
In this context, it should be considered that identification of the KPC production at phenotypic level is still a challenge and has likely contributed to the rapid spread of this carbapenemase. Only molecular methodologies can quickly and comprehensively detect the presence of blaKPC in clinical isolates, whose routine identification should be considered as necessary for all bacterial species exhibiting this resistance mechanism, to optimize antibiotic therapy, limit KPC-mediated resistance to carbapenems and increase patient survival.
The reinforcement of antimicrobial stewardship programs at both local and national levels, as well as the support for research and development of novel antibiotic molecules, is required. This is considered necessary taking into account that E. coli resistance toward third-generation cephalosporins is estimated as 77% in 2030 compared to 64.5% in 2015, and toward carbapenems as 11.8% compared to 5.8%. 34
Furthermore, such measures significantly contribute to reduce the likelihood of occurrence of infections by CRE organisms, and should be part of the implementation of multimodal strategies (bundles) of infection/colonization control to avoid transmission, in agreement with the globally developed evidence-based recommendations, 35 and taking into account their high capabilities of clonal expansion. 31
This report draws attention on the concrete risk of the spread of KPC enzymes producing E. coli, as well as the likelihood of a rapid dissemination due to the genetic characteristics, particularly related to ST131 high-risk clone circulation, and its potential of spreading resistance. Since ST131 has markedly contributed to an increased prevalence of antimicrobial resistance among E. coli isolates, targeted and direct interventional measures are required to prevent the spread of these epidemiologically successful strains.
Footnotes
Acknowledgments
We thank Dr. Jim McLauchlin, Public Health England, London, United Kingdom, for the helpful comments provided to the article and Dr. Giuliana Guerrizio for supporting the molecular laboratory investigations.
Authors' Contributions
G.R., M.L.S., and M.T. drafted the article and conducted molecular data analysis. M.S. and V.F. isolated and provided the strain with routine phenotypical data.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.