
Abstract
During 2014–2016, a total of 248 carbapenem-resistant Klebsiella pneumoniae (CARB-R Kp) were recovered in a Greek intensive care unit (ICU), the colistin resistance (COL-R) rates among CARB-R Kp from bloodstream infections (BSIs) were determined, and molecular characterization and the in vitro susceptibility of CARB-R+COL-R Kp to ceftazidime/avibactam were performed. The majority of CARB-R Kp from BSIs (n = 53) were OXA-48 (43.4%) and KPC (33.9%) producers, but no statistically significant differences were observed for the clinical characteristics of ICU patients affected by OXA-48 and other carbapenemase-producing K. pneumoniae. CARB-R+COL-R Kp (n = 28) represented 52.8% of 53 CARB-R Kp recovered from BSIs. The increase in the COL-R rates from 2014 to 2015 was mainly associated with the diffusion of extensively drug-resistant
Introduction
The alarming increase in the incidence of carbapenemase-producing Enterobacteriaceae (CRE) in health care settings globally, the development of resistance to most available antibiotics and the increased morbidity and mortality caused by these bacteria have been major challenges for the treatment of CRE infections.1,2 CRE are primarily identified among patients with health care exposure, but there is potential for CRE to spread outside of health care settings. Source control and strict infection control measures are essential for the effective management of CRE infections.3,4 Klebsiella pneumoniae is a common pathogen causing bloodstream infections (BSIs) and patients with BSIs due to carbapenem-resistant K. pneumoniae (CARB-R Kp) should receive active therapy as soon as they are diagnosed.5–12 Empirical combination therapy (usually including colistin, a carbapenem, or an aminoglycoside) is considered to improve chances of clinical cure and survival in CRE infection, and monotherapy should be considered for those in the low-mortality-score stratum. 8
Colistin is a polycationic antimicrobial peptide that is currently administrated as one of the last-resort antibiotics for the treatment of multidrug-resistant Gram-negative bacterial infections. The reintroduction of colistin for antimicrobial therapy has been followed by an increase in the colistin resistance (COL-R) rates among Gram-negative bacteria.13–17 Ceftazidime/avibactam is a novel β-lactam (ceftazidime) and β-lactamase inhibitor (avibactam) combination that inactivates the active site of serine-β-lactamases, including Ambler class A extended-spectrum β-lactamases (ESBLs), Ambler class C AmpC β-lactamases, the class A carbapenemases, and some class D carbapenemases.18,19 The Ambler class B β-lactamases or metallo-β-lactamases (MBLs) are resistant to avibactam-mediated inhibition.
Optimal treatment of CRE infections should be based on the local resistance epidemiology. Carbapenemase-producing K. pneumoniae have become endemic in some countries, such as Greece.20–22 The first occurrence of VIM- and KPC-2-producing K. pneumoniae was reported in 2005 and 2008, respectively.23,24 Although KPC and VIM producers have been reported more frequently, outbreaks of OXA-48 producers have been documented and NDM producers were isolated in Greek hospitals recently.25–30 We have previously reported the rise in the incidence of the colistin-resistant KPC-producing K. pneumoniae belonging to the international clone multilocus-sequence typing (MLST) ST258 during 2012–2013 at the general hospital of N. Ionia “Konstantopouleio-Patission,” Athens, Greece. 31 The purpose of this study was the determination of the COL-R rates among CARB-R Kp from 2014 to 2016, the characterization of CARB-R+COL-R Kp from BSIs and the investigation of their in vitro susceptibility to ceftazidime/avibactam.
Materials and Methods
Setting
“Konstantopouleio-Patission” is a 280-bed general hospital (including a nine-bed intensive care unit [ICU], internal medicine, surgical, urology, and other wards) located at the capital city of Greece, Athens, with approximately three million inhabitants. During the study period, infected patients with CARB-R Kp were isolated, whereas in some instances a cohorting policy of patients according to the type of carbapenemases of CARB-R Kp was implemented. In the ICU, surveillance rectal swab cultures were routinely collected within 24 hr from all newly admitted patients.
Bacterial isolates and antimicrobial susceptibility testing
Identification of the isolates and antimicrobial susceptibility testing were performed by the MicroScan® (Siemens Healthcare, PA), according to the Clinical and Laboratory Standards Institute (CLSI) interpretive standards. 32 The minimum inhibitory concentrations (MICs) of the isolates were additionally determined using the MIC Test Strips (Liofilchem S.R.L, Italy) on Mueller Hinton (MH) Agar plates for imipenem, meropenem, colistin, tigecycline, and ceftazidime/avibactam. For colistin-resistant or isolates with discrepant results, the MICs for colistin were also confirmed by the SensiTest Colistin (Liofilchem S.R.L) and the MIC-Strip Colistin (Merlin, Diagnostika, GmbH, Germany) broth microdilution methods, according to the instruction of the manufacturers.
K. pneumoniae isolates with MICs of imipenem and meropenem >2 mg/L and ceftazidime/avibactam >8 mg/L were categorized as resistant, following the CLSI interpretive standards. K. pneumoniae isolates with MICs of colistin and tigecycline >2 mg/L were categorized as resistant, according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) interpretive criteria (www.eucast.org). The first CARB-R Kp bloodstream isolate of each patient was collected and stored on glycerol culture broth at −80°C for further analysis.
Phenotypic and molecular determination of carbapenemase and ESBL production
The combined-disk tests were used by applying meropenem disks alone and with 400 μg of phenylboronic acid (PBA) or 292 μg of ethylenediaminetetraacetic acid (EDTA) or both (400 μg of PBA and 292 μg of EDTA) on MH Agar plates for the phenotypic detection of carbapenemase production and the differentiation of KPC and MBL enzymes, as described previously. 33 Τhe modified CLSI ESBL confirmatory test was used for phenotypic detection of ESBLs among carbapenemase producers. 34 The production of KPC, OXA-48, VIM, and NDM carbapenemases was determined by the immunochromatographic tests KPC K-SeT, OXA-48 K-SeT, and RESIST-4 O.K.N.V., CORIS, BioConcept, Belgium.35,36 DNA extraction was carried out using the QIAcube system (Qiagen, Düsseldorf, Germany), according to the instructions of the manufacturer. Carbapenemase- (blaKPC, blaOXA-48, blaVIM, and blaNDM)28,31 and ESBL-encoding genes (blaSHV-12 and blaCTX-M-15 type) 37 were detected by PCR using specific primers, as described previously.
Molecular typing and sequence analysis of the mgrB gene
Genotyping of the isolates was performed by MLST using seven housekeeping loci (rpoB, gapA, mdh, pgi, phoE, infB, and tonB) and sequence types were determined using the K. pneumoniae MLST website, according to the scheme developed by Diancourt et al. 38 PCR amplification and sequencing of the mgrB gene for selected isolates was performed, as described previously. 31
Definition of cases, collection of clinical data, and statistical analysis
During the first semester (6 months' period) of 2015, four K. pneumoniae isolates recovered in the ICU showed an extensively drug-resistant (XDR) phenotype, 39 that is, nonsusceptibility to ≥1 agent in all but ≤2 categories, with variable decreased susceptibility or resistance to carbapenems, accompanied with resistance to penicillins, cephalosporins, cephamycins, penicillins/β-lactamase inhibitor combinations, fluoroquinolones, aminoglycosides, folate pathway inhibitors (trimethoprim/sulfamethoxazole combination), and polymyxins. The four XDR Kp isolates were positive for carbapenemase production, as shown by the modified Hodge test, but negative for KPC and/or MBL production by using the meropenem with PBA, EDTA, and PBA+EDTA combined disk tests. All isolates carried the blaOXA-48 gene, as shown by PCR. Since OXA-48 producers are difficult to detect, all available frozen K. pneumoniae isolates from BSIs recovered since January 2014 were tested for the presence blaOXA-48 by PCR.
An epidemiological study was conducted, and cases were defined as any in-patient with positive blood cultures for OXA-48-producing K. pneumoniae. All patients affected by blaOXA-48 producers were put under strict contact isolation or cohort care, along with appropriate infection control measures. Clinical and epidemiological data of ICU patients were reviewed retrospectively, including gender, age, surgical procedures, length of stay (LOS) in the ICU, previous history of hospitalization, initial diagnosis, ventilator-associated pneumonia (VAP), outcome, previous antibiotic treatment with carbapenems and/or colistin, and fecal carriage of CARB-R Kp upon admission in the ICU. Statistical analysis was performed using the Fisher's exact test for categorical variables and the Mann–Whitney U test for continuous variables (statistical tools available at https://www.socscistatistics.com/).
Results
Antibiotic susceptibility testing and carbapenemase content of bloodstream CARB-R Kp
During January 2014–December 2016, a total of 248 CARB-R Kp were isolated mainly from bronchial secretions (n = 105, 42.3%), blood (n = 53, 21.8%), central venous catheters (n = 39, 15.7%), and urine (n = 28, 11.3%) of patients admitted to the ICU. During the study period, co-resistant to carbapenems and colistin (CARB-R+COL-R) Kp (n = 28) represented 52.8% of 53 CARB-R Kp recovered from BSIs. A gradual increase was observed in the incidence of bloodstream CARB-R+COL-R Kp from 33.3% on the first semester of 2014 to 80% on the second semester of 2015, but it has decreased to 41.7% on the second semester of 2016, as shown in Fig. 1.

Percentage (%) of COL-R and COL-S Kp among CARB-R Kp (n = 53) recovered per semester from BSIs in the ICU during 2014–2016. BSI, bloodstream infection; CARB-R Kp, carbapenem-resistant Klebsiella pneumoniae; COL-R, colistin resistance; COL-R Kp, colistin-resistant Klebsiella pneumoniae; COL-S Kp, colistin-susceptible Klebsiella pneumoniae; ICU, intensive care unit.
CARB-R Kp isolates recovered from BSIs were screened for the presence of carbapenemases by the boronic acid/EDTA test using meropenem as substrate, the immunochromatographic tests, and confirmed by PCR. The carbapenemase content of CARB-R Kp (n = 53) recovered per semester during the study period is presented in Fig. 2. The majority of CARB-R Kp from BSIs were OXA-48 producers (n = 23, 43.4%) and KPC producers (n = 18, 33.9%), whereas the remaining 12 isolates (22.6%) produced and/or MBL types of carbapenemases (6 VIM, 3 OXA-48+VIM, and 3 NDM producers). During the study period, the highest rates of COL-R were observed among OXA-48 producers (22 out of 23 isolates, 95.6%). Of the 18 KPC and the remaining 12 carbapenemase producers, 5 (27.8%) and 1 (8.3%) isolates, respectively, were COL-R.
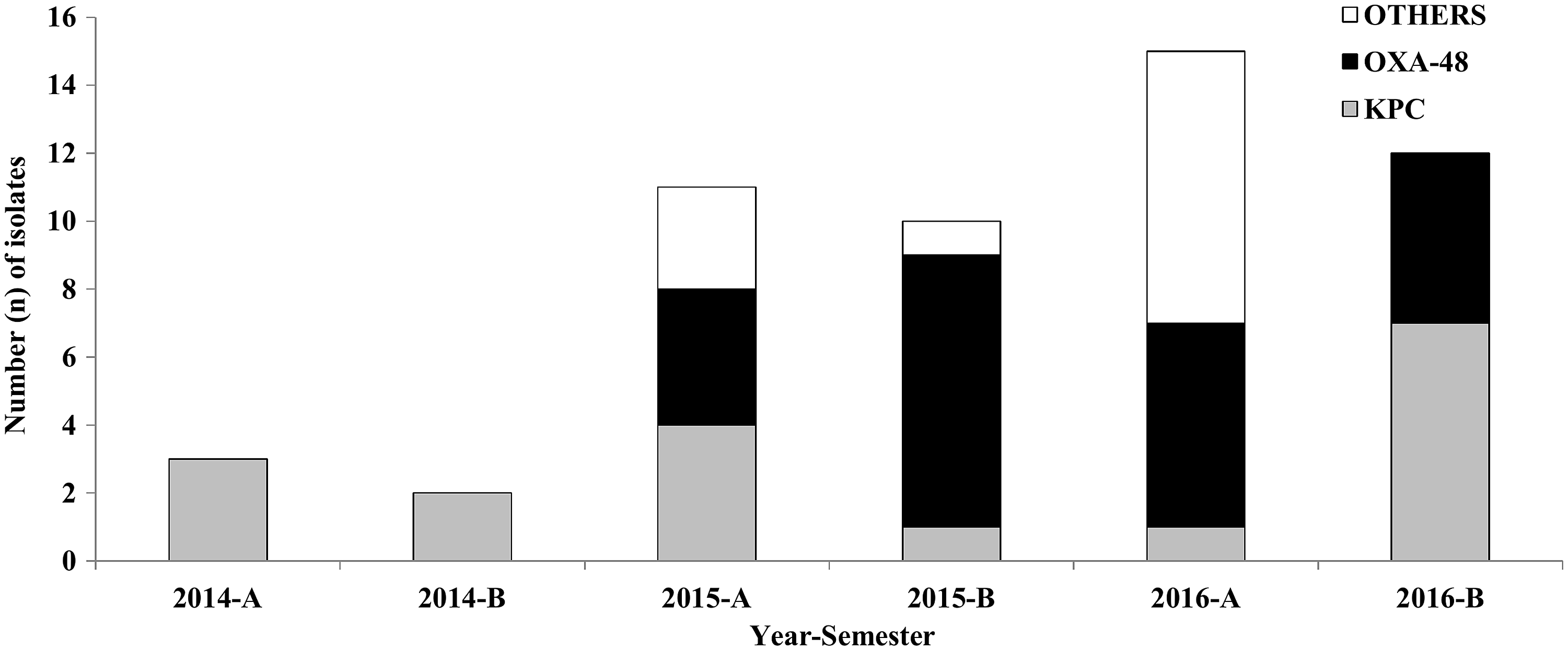
Carbapenemase content of CARB-R Kp (n = 53) recovered from BSIs per semester during 2014–2016.
From the first to the second semester of 2015, a rapid increase in the rates of isolation of OXA-48 producers was observed from 36.3% (4 OXA-48 producers out of 11 CARB-R Kp) to 80% (8 OXA-48 producers out of 10 CARB-R Kp) (Fig. 2). On the second semester of 2016, the incidence OXA-48 producers has decreased to 41.6% (5 out of 12 CARB-R Kp were OXA-48 producers). During January 2017–June 2018, out of 15 CARB-R Kp isolates recovered from BSIs in the ICU, only 1 COL-R OXA-48 producer was isolated (6.7%); thus, we assume that the outbreak was successfully controlled.
Antibiotic resistance patterns and molecular characterization of CARB-R+COL-R from ICU patients
The microbiological and molecular characteristics of CARB-R+COL-R Kp recovered from the bloodstream of ICU patients during the study period are presented in Table 1. During 2014, only two CARB-R+COL-R Kp isolates were recovered, which were KPC producers of MLST ST258. The first COL-R OXA-48 producer of MLST ST101 (allelic profile: 2-6-1-5-4-1-6) was isolated on February 2015. All OXA-48 Kp (n = 22) belonged to MLST ST101 and coproduced CTX-M-15-like enzymes. All COL-R OXA-48 producers were characterized as XDR, but they were susceptible to tigecycline. During the study period, only one susceptible to colistin OXA-48 producer of MLST ST1593 (allelic profile: 4-1-11-1-9-4-59) was isolated during 2016 in the ICU, after the onset of the outbreak. Thus, blaOXA-48 has been transferred to different K. pneumoniae strains with variable susceptibility to colistin. All KPC-producing K. pneumoniae (n = 5) belonged to MLST ST258 and two of them coproduced SHV-12-like enzymes. Among the CARB-R+COL-R Kp, there was an NDM coproducing CTX-M-15-like K. pneumoniae of MLST ST11. Excluding one NDM producer, all KPC and OXA-48 producers were susceptible to ceftazidime/avibactam.
Microbiological and Molecular Characteristics of Bloodstream CARB-R+COL-R Kp (n = 28 Isolates) from Intensive Care Unit Patients During 2014–2016
AK, amikacin; AMP/SUL, ampicillin/sulbactam; CAZ, ceftazidime; CIP, ciprofloxacin; CZA, ceftazidime/avibactam; ESBL, extended-spectrum β-lactamase; FEP, cefepime; GM, gentamicin; IMP, imipenem; MER, meropenem; MIC, minimum inhibitory concentration; MLST, multilocus-sequence typing; NA, not amplified; S, susceptible; SXT, trimethoprim/sulfamethoxazole; TOB, tobramycin; TZP, piperacillin/tazobactam.
PCR amplification of mgrB was carried out for all 28 CARB-R+COL-R Kp recovered in the ICU (Table 1). Of the 28 isolates, PCR products of ∼1400 bp were obtained from 12 OXA-48, 2 KPC, and 1 NDM producers, indicating that an insertion event has occurred in the ∼150 bp wild-type (WT) mgrB locus. Besides several attempts, no PCR amplification products were obtained from 10 OXA-48 producers and 1 KPC producer, indicating that a deletion may have occurred in the mgrB locus, as reported for other COL-R Kp previously. 35 PCR products of the WT size of the mgrB locus (150 bp) were obtained from two KPC producers.
Sequencing analysis of the PCR products from two COL-R OXA-48 producers (isolates AO-1831 and AO-1864) has revealed an insertional inactivation of the mgrB locus by an IS5-like element, showing 100% nucleotide sequence similarity with the mgrB locus of the colistin-resistant strain KKBO-4 (GenBank accession no. HG008893) recovered in an Italian ICU. 40 Insertional inactivation of the mgrB locus by an IS5-like element of a KPC producer (isolate AO-1770) was also revealed, which showed 100% nucleotide sequence similarity with a previously described sequence obtained from a COL-R KPC producer in our hospital (GenBank accession no. KP967591). 31 The COL-R NDM producer possessed an inactivated mgrB locus by an IS903.B transposase, showing 100% nucleotide sequence similarity with isolate Lar-Kpn3028 recovered in another Greek hospital (GenBank accession no. KP861895).
Clinical characteristics and statistical analysis of OXA-48 producers from ICU patients
The epidemiological and clinical characteristics of ICU patients with OXA-48 producers (n = 23) were compared with those of ICU patients with CARB-R Kp that produced other types of carbapenemases (n = 30; 18 KPC, 6 VIM, 3 NDM, and 3 OXA-48+VIM producers), as shown in Table 2. The ICU patients with OXA-48 producers were 23–85 years old (mean of ranks: 30.72 years), 10 of them (43.5%) were subjected to surgical procedures, 2 of them (8.7%) were diagnosed with VAP infection, showed APACHE II scores of medium severity (range: 13–37, mean of ranks: 29.2), mortality rates of 43.5% (10 out of 23 patients have expired), and 2–89 days (mean of ranks: 23.74 days) LOS in the ICU. Out of 18 ICU patients with OXA-48 producers tested, 7 patients (38.9%) were positive for CARB-R Kp from rectal swab cultures upon admission, indicating that in these cases the COL-R OXA-48 Kp were imported in the ICU. A COL-R OXA-48 Kp isolate was recovered from a clinical specimen (including blood) within 48 hr upon admission in the ICU in four out of 22 patients (18.1%). No statistical significant differences were observed for the clinical characteristics between the OXA-48 producers and other carbapenemase producers (Table 2).
Clinical Characteristics of OXA-48 and Other Carbapenemase-Producing Klebsiella pneumoniae in the Intensive Care Unit During 2014–2016
Statistical significant results at level p < 0.05.
Mean of ranks.
CARB, carbapenem; COL, colistin; ICU, intensive care unit; VAP, ventilator-associated pneumonia.
Discussion
Carbapenemase-producing K. pneumoniae have become endemic in Greece during the past decade.23–27 In this study, we report an outbreak of colistin-resistant OXA-48 and CTX-M-15-like-producing K. pneumoniae from BSIs, assigned to MLST ST101 in the ICU of the General Hospital of N. Ionia, Athens, Greece, which was associated with an increase in the COL-R rates among CARB-R Kp during 2014–2016. COL-R was associated with alterations in the mgrB locus. In addition, a colistin-susceptible OXA-48 producer of an unrelated MLST ST (ST1593) than the outbreak strain (ST101) has been identified. No statistically significant differences were observed for the clinical characteristics of OXA-48 and other carbapenemase-producing K. pneumoniae (KPC and MBL producers).
The rate of isolation of OXA-48 producers has increased rapidly from the first to the second semester of 2015, but it has decreased during the second semester of 2016, and the period January 2017–June 2018. The successful control of the outbreak may be attributed to the enhanced surveillance of BSIs from multidrug-resistant bacteria, implementation of strict infection control measures, and an intensive educational program toward all aspects of infection control in the ICU, particularly hand hygiene along with proper CVCs maintenance and accession, utilization of the same multiple-dose bottle of heparin and disinfectants for 2–3 patients that changed to single-patient use of these vials.
The first outbreak of OXA-48-producing K. pneumoniae of MLST ST11 has been reported in 2013, whereas a second outbreak of OXA-48-producers also assigned to MLST ST101 has occurred during 2014–2016 at the Tzaneio Hospital, Athens, Greece. 28 Sporadic OXA-48-producing K. pneumoniae have also reported in other Greek hospitals.27,29 These data reveal the diffusion of these strains in different Greek hospitals, imposing an additional threat for combating CRE infections in Greece. blaOXA-48 can be transferred in different K. pneumoniae strains as it is usually located on a plasmid, but may also be integrated chromosomally. MLST ST101 has been previously reported among CTX-M-15 producers in Greece. 37 Therefore, blaOXA-48 has been transferred in different K. pneumoniae strains in Greece. OXA-48-producing K. pneumoniae strains have caused outbreaks worldwide, particularly in the Mediterranean area (France, Turkey, North Africa, and the Middle East).41–44 MLST ST101 has been also reported among OXA-48 producers in other countries, such as Turkey, Egypt, and France.
OXA-48 and its variants are unique carbapenemases with low-level hydrolytic activity toward carbapenems, but no intrinsic activity against expanded spectrum cephalosporins. Coproduction of OXA-48 and CTX-M-type ESBLs confers resistance to extended-spectrum cephalosporins, such as ceftazidime and cefepime. Therefore, OXA-48 producers impose another therapeutic challenge for combating CRE infections.45–48 In this study, high rates of COL-R were observed among OXA-48 producers (95.6%), mainly due to inactivation of the mgrB locus. Thus, colistin could not be used for targeted therapy of BSIs in these cases. Besides, XDR OXA-48-and KPC producers predominated among CARB-R+COL-R Kp, which were susceptible to ceftazidime/avibactam. Recent studies have shown successful outcomes of ceftazidime/avibactam monotherapy in ∼70% of patients with infections caused by OXA-48-producing Enterobacteriaceae. 46 Nevertheless, ceftazidime/avibactam-resistant K. pneumoniae isolates with modified KPC enzymes have been reported to emerge during therapy recently. 49
In conclusion, the diffusion of CARB-R+COL-R Kp limits the therapeutic options for combating carbapenemase producers from BSIs. Furthermore, the spread of XDR Kp possessing different types of carbapenemases further complicates the infection control strategies for the management of CRE. Ceftazidime/avibactam may be a reasonable alternative to colistin for the treatment of XDR Kp from BSIs and colistin-resistant KPC- and OXA-48 producers in settings with low prevalence of MBL-producing K. pneumoniae. Nonetheless, the use of ceftazidime/avibactam may favor the selection of ceftazidime/avibactam-resistant strains.
Footnotes
Acknowledgment
The authors thank Ms Rania Kordanouli for excellent technical assistance.
Disclosure Statement
No competing financial interests exist.