
Abstract
Objectives:
To study the in vitro synergistic bactericidal activity of dual β-lactam antibiotics against KPC-2-producing Klebsiella pneumoniae and to explore the new therapeutic regimens for infections caused by carbapenem-resistant strains.
Materials and Methods:
The antimicrobial susceptibility testing of imipenem, meropenem, ceftazidime, and clavulanic acid on 40 clinically isolated strains of KPC-2-producing K. pneumoniae from 5 cities across the country was performed by microdilution broth method. The in vitro synergistic bactericidal activity of combined antibiotics mentioned above was determined at various concentrations using checkerboard techniques. The combination of antibiotics include imipenem with clavulanic acid, meropenem with clavulanic acid, imipenem with ceftazidime, meropenem with ceftazidime, and meropenem with imipenem. The combined effectiveness of synergistic, indifferent, or antagonistic was calculated by fractional inhibitory concentration indexes. Based on the results of synergistic bactericidal activity, 16 strains were selected for time-kill assays.
Results:
All 40 strains of K. pneumoniae were shown resistant to every single antimicrobial agent tested, with minimal inhibitory concentrations of carbapenems >32 mg/L in most isolates. None of the combinations was antagonistic. Synergies of combination of imipenem with clavulanic acid, or imipenem with ceftazidime were observed in 80% (32/40) and 7.5% (3/40) of strains, respectively; Combinations of meropenem and clavulanic acid, or meropenem and ceftazidime revealed a synergistic antibacterial activity on 25% (10/40) and 30% (12/40) of strains, respectively. Synergy of meropenem and imipenem combination was shown in 30% (12/40) of strains. Time-kill assays validated the data from checkerboard testing.
Conclusions:
The study strongly supported the hypothesis that combined dual β-lactam antibiotics might be effective in the treatment of infections caused by KPC-2-producing K. pneumoniae. The combination of imipenem and clavulanic acid possessed the best efficiency, followed by the regimens of combined meropenem–ceftazidime and imipenem–meropenem.
Introduction
In recent years, the incidence of carbapenem-resistant Enterobacteriaceae (CRE) infection is rapidly increasing year by year. The clinical isolates of Klebsiella pneumoniae carbapenemase-producing K. pneumoniae (KPC-KP) have wildly spread all over the world.1–4 According to the U.S. Centers for Disease Control and Prevention, the infection rate of CRE in the United States elevated from 1.2% in 2001 to 4.2% in 2011. Of the 140,000 cases with Enterobacteriaceae infection per year, 9,300 (6.6%) were infected by the CRE strain. 5 The results of 12-year bacterial resistance monitoring from China Antimicrobial Surveillance Network (CHINET) also disclosed the significant rising trend of K. pneumoniae resistance to imipenem or meropenem, from 2.4% in 2005 to 18.6% in 2016. 6
Since the CRE strain is commonly resistant to most antibiotics commonly used in clinical practice, patients are accompanied with a high morbidity and mortality. Therefore, it instigates a severe challenge for treating these infections. Although the results of antimicrobial susceptibility testing in vitro showed that the CRE strain was still highly sensitive to tigecycline and polymyxin, they had the disadvantages of low plasma concentration and being prone to initiating the drug resistance.7,8 Moreover, the resistance to polymyxins and tigecycline has been reported in previous literatures.9,10 Therefore, to avoid the over-reliance on tigecycline and polymyxins treatment, it is necessary to explore the new effective therapeutic regimens by recombination of other antibiotics to meet the growing needs for managing the CRE infection. 11 Recent studies have reported the efficacy of a double carbapenem combination including ertapenem in the treatment of carbapenem-resistant K. pneumoniae (CR-KP) infections.12,13 However, we found that the combination of double carbapenem may not fit the treatment of CR-KP strains isolated clinically in China. Our previous studies have indicated that the combination of carbapenem with ceftazidime or clavulanic acid was superior to the double carbapenem for treatment of CR-KP infections. 14 Thereupon, in this study, we aimed to determine the in vitro activity of these new combinations against KPC-KP.
Materials and Methods
Strains
All 40 nonduplicated KPC-KP clinical strains were collected from 5 cities over China. All K. pneumoniae were blaKPC-2-positive strains confirmed by PCR and DNA sequencing. Strains were identified by mass spectrometry. Escherichia coli ATCC 25922 were used as a quality control strain in antimicrobial susceptibility testing.
Determination of minimal inhibitory concentration and checkerboard synergy testing
The minimal inhibitory concentrations (MIC) of imipenem, meropenem, ceftazidime, and clavulanic acid against KPC-KP were determined using broth microdilution technique as recommended by the CLSI guidelines. 15 The testing concentration of each antimicrobial agent ranged from 0.25 to 512 mg/L. The in vitro synergistic bactericidal activity of dual β-lactam combinations was detected by checkerboard techniques including imipenem–clavulanic acid, meropenem–clavulanic acid, imipenem–ceftazidime, meropenem–ceftazidime, and meropenem–imipenem as previously described.16,17 The calculation and interpretation of fractional inhibitory concentration (FIC) referred to the document standards. 18 FIC indexes were calculated according to the formula: ΣFIC = FIC of drug A + FIC of drug B, where FIC of drug A or B = MIC of drug A or B in combination divided by the MIC of drug A or B alone. Interpretation of the results was based on the following descriptions: FIC values of ≤0.5 indicate synergy, FIC values of >0.5–1 indicate addition, FIC values of >1–2 indicate no interaction, and FIC values of >2 indicate antagonism.
Time-kill assays
In accordance with the results of checkerboard techniques, 16 strains of K. pneumoniae were randomly selected to conduct the synergistic bactericidal curves using time-kill assays.19,20 Killing effects were quantified by standard time-kill assays using effective carbapenem concentrations as suggested by checkerboard experimental data (Table 1). The operation procedure is briefly described as follows: Mueller–Hinton broth containing 1 × 105 CFU/mL bacteria was mixed with single or combined testing antibacterial agents and then incubated overnight with consecutive shacking at 35°C in atmospheric environment. Meanwhile, the same broth without antibiotics experienced identical procedure and served as a control. Incubated broth samples were serially diluted at time points of 0, 2, 4, 6, 8, and 10 hours and smeared on the Mueller–Hinton plate, respectively. After overnight incubation at 35°C, bacteria colonies were counted and the bactericidal profiles were plotted. If the reduction of survival bacterial number in sample treated with combined antibiotics was ≥2 log10 CFU/mL than that in the sample treated by single drug, it was considered to have a synergistic bactericidal effect.
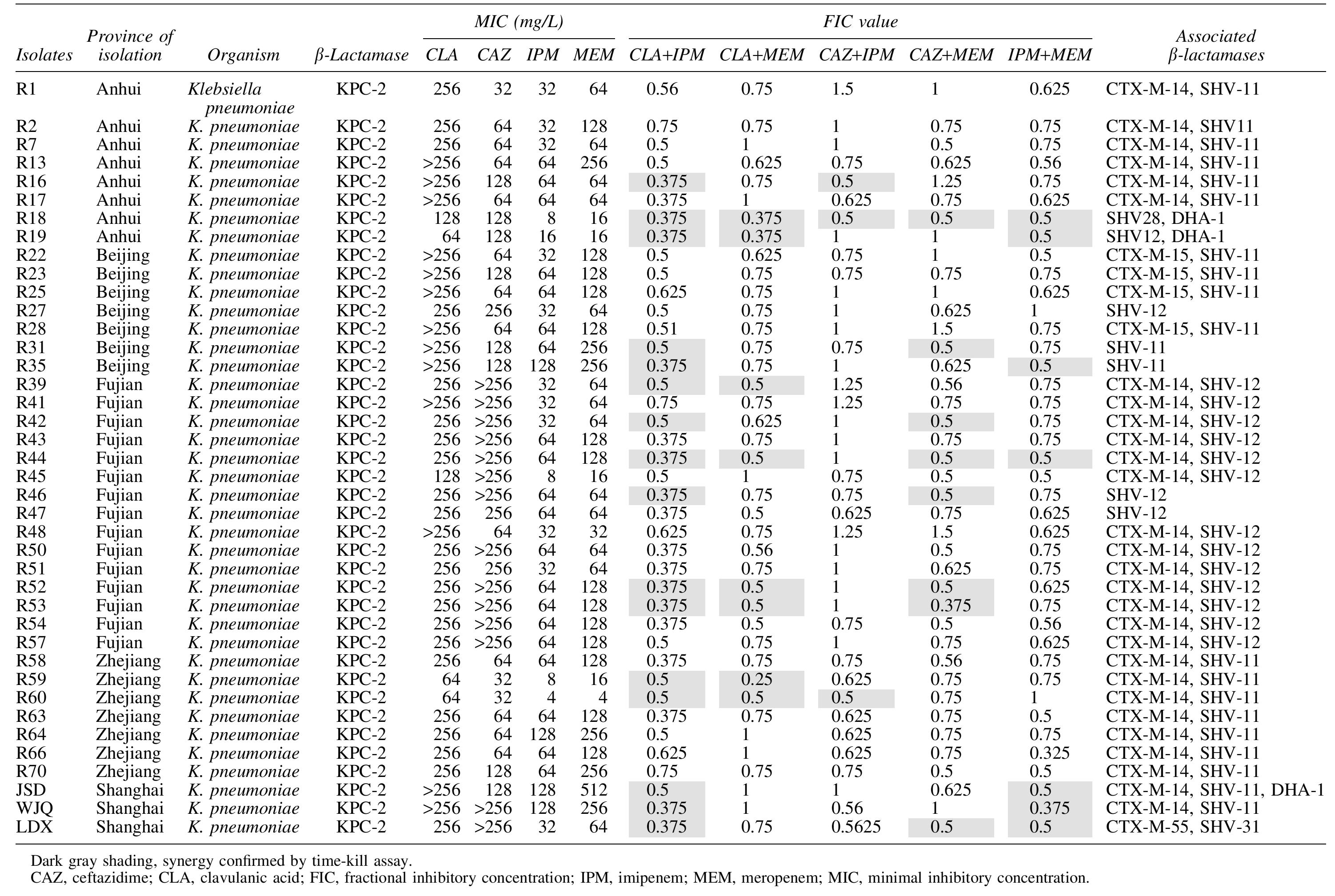
The Minimal Inhibitory Concentration and Synergistic Effect of Various Antibiotics to 40 blaKPC-2-Positive Klebsiella pneumoniae Clinical Isolates
Results
A total of 40 KPC-KP strains were shown resistant to ceftazidime, imipenem, and meropenem, with the MIC50 and MIC90 values of 128 and >256, 64 and 64, 128 and 256, respectively. The results of checkerboard testing suggested that five regimens of combined dual β-lactams were of synergistic effects. In which, the combination of imipenem and clavulanic acid showed the most efficient. Eighty percent (32/40) of strains treated with this regimen showed synergistic effects. Nevertheless, the combination of imipenem and ceftazidime showed synergistic effects only in three strains, whereas 82.5% (33/40) of strains showed additive effects and 10% (4/40) of strains showed irrelevant effects. The combination of meropenem and clavulanic acid, or meropenem and ceftazidime had a similar synergistic antibacterial effect against 25% (10/40) and 30% (12/40) of strains, respectively. None of the combinations of dual β-lactams described above exhibited the antagonistic effects (Table 1).
The results of time-kill assays revealed that if combined β-lactams showing a synergistic effect against 16 strains of K. pneumoniae in checkerboard testing, it could display the consistent synergistic bactericidal effectiveness as well within 4–6 hours after administration (Fig. 1). The bactericidal effects on 56.5% (9/16) of strains within 6 hours were observed in combined imipenem and clavulanic acid. In the combination of meropenem and clavulanic acid, the synergistic bactericidal effects against two strains were found in 4 hours. The best synergistic bactericidal effects of combined imipenem and ceftazidime were observed at the time point of 10 hours when the bacterial amounts of strains R18, R16, and R60 compared with the single dosing of imipenem or ceftazidime were reduced by an average of 8.6, 6.4, and 5.8 log10 CFU/mL, respectively.
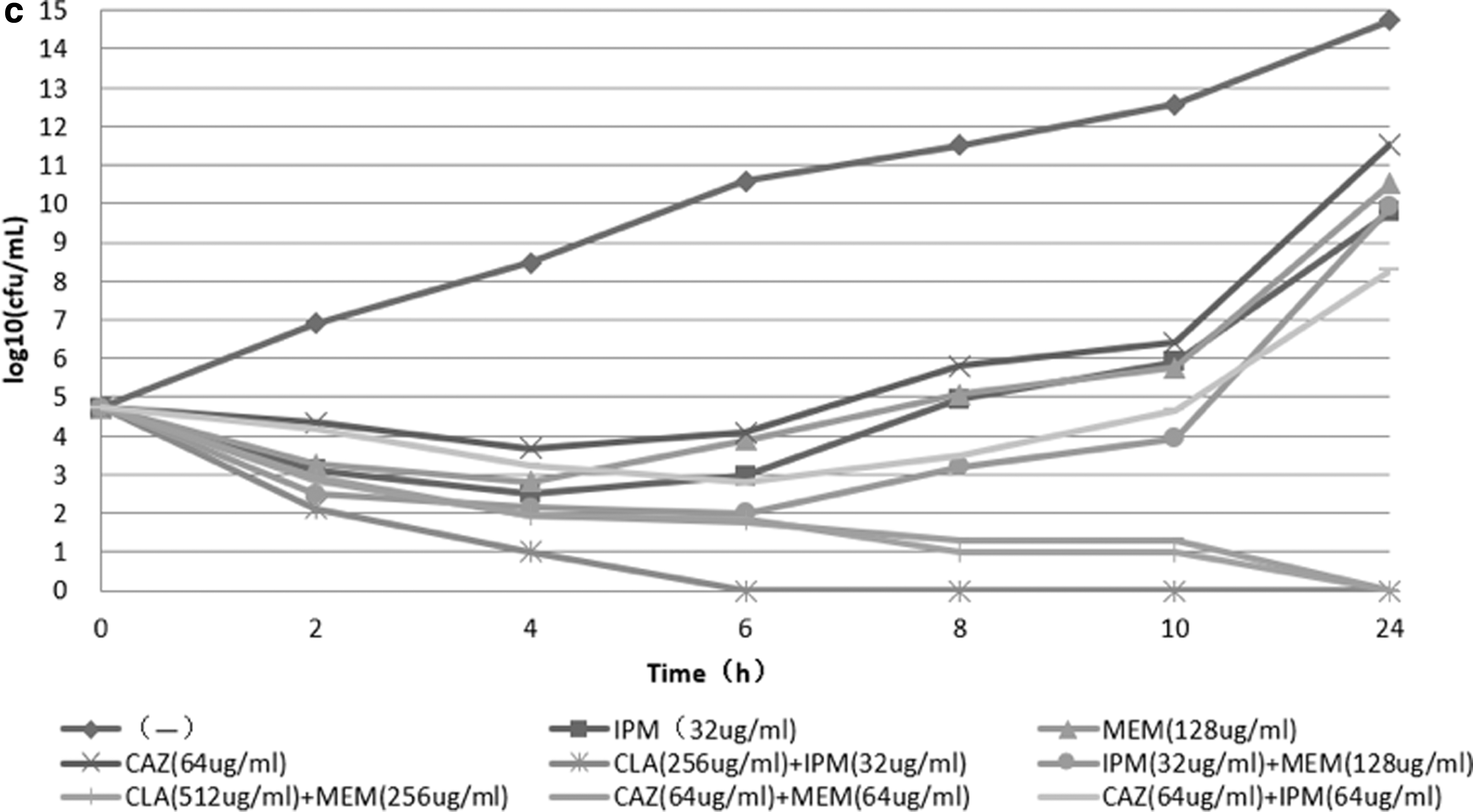
Time-kill assays of dual β-lactam antibiotics to KPC-KP clinical isolates.
Discussion
In the past years, the emergence of carbapenemase-producing K. pneumoniae featured with extensive resistance has become a serious problem in the fields of sanitation and health care all over the world. Attributable to lack of effective antibacterial agents, especially the development of the strains with high virulence and resistance, it commonly resulted in the failure of clinical treatment and increased the mortality of patients.21,22 Previous studies reported that the combination of carbapenems and other antibiotics for the treatment of carbapenems-resistant K. pneumoniae infection could significantly improve the prognosis of patient compared with those treated with carbapenems alone. 23 The combined regimens included carbapenems plus other various antimicrobial molecules such as polymyxin, tigecycline, amikacin, and fosfomycin.24–28 However, fewer were reported to involve the dual β-lactam antibiotics. Poirel et al. 12 proposed a combined curative protocol of dual carbapenems to provide a new solution for the CRE infection management. Since the clavulanic acid has the capability of partially inhibiting the KPC carbapenemase and weakly hydrolyzing the ceftazidime, we took the advantage to design the new therapeutic regimens of carbapenems in combination with clavulanic acid or ceftazidime, so as to meet the requirements in the treatment of KPC-2 carbapenemase-inducing infections in clinical practice.
The results of checkerboard synergy testing for five combined therapeutic regimens indicated that the combination of imipenem and clavulanic acid showed the best efficacy, of which the synergistic rate reached 80%, with the other 20% showing an additive effect. The combination of meropenem and clavulanic acid produced a synergistic antibacterial effect on 25% (10/40) of strains. As a weak inhibitor of KPC carbapenemase, high-dose clavulanic acid combined with carbapenem might be useful for the treatment of infections caused by KPC-KP, particularly when combined with imipenem. Recently, it has been reported that the polymyxin-resistant, KPC or OXA-48 carbapenemase-producing K. pneumoniae infections were successfully treated with enzyme inhibitor ceftazidime–avibactam compound. 29 Meantime, Gaibani et al. 30 verified that the synergistic effect of ceftazidime–avibactam plus imipenem on KPC-KP was superior to that plus any other antibiotics. In the combination of ceftazidime with imipenem or meropenem, the effects were better than that combined with meropenem, which had the synergistic antibacterial effect for 30% (12/40) of strains, but to three strains only when combined with imipenem. It is interesting that the combination with clavulanic acid demonstrated the different effects compared with those in the combination with ceftazidime (80% vs. 25%, 7.5% vs. 30%). The synergistic rate of dual carbapenems combined with imipenem and meropenem is 30%, similar to that reported by Poirel et al. 12
To validate the synergistic effects of checkerboard techniques, 16 KPC-KP strains were randomly selected for the time-kill assays, which proved the data assessed by checkerboard testing. The time of occurrence of combined bactericidal effects was different in various antibiotics combinations; the earliest one appeared after 4 hours of administration and was mainly shown in combined ceftazidime and meropenem or imipenem. The synergistic bactericidal effects should occur no later than 10 hours after antibiotics were applied. Different combinations of antibiotics produce different synergistic effective levels on different strains. The synergistic effects of clavulanic acid–carbapenems (imipenem and meropenem), and the combination of clavulanic acid with imipenem on strain R35 are evidently clear. At the time points of 6, 8, and 10 hours after treatment with combined antibiotics, no bacterial colony growth was found. The bacteria number was reduced by 8.8 log10 CFU/mL after 10 hours of treatment with dual combinations than that with imipenem alone. However, this strain did not show the synergistic effects after treated by clavulanic acid–meropenem. In the combination of ceftazidime and carbapenems (imipenem or meropenem), we found that only 3 of the 40 strains showed the synergistic effects when combined with imipenem, in which R18 and R16 strains showed the significant effect. The amount of CFU after 10 hours of treatment with combined antibiotics was reduced by 8.6 and 6.4 log10 CFU/mL than those treated with imipenem and ceftazidime alone, respectively. Lenhard, J.R et al. 31 utilized polymyxin B combined with four carbapenem antibiotics to evaluate the pharmacodynamics on Acinetobacter baumannii resistant to carbapenemases and found that doripenem in combination with polymyxin B showed the best bactericidal effects compared with other carbapenems.
In summary, the in vitro synergistic testing of antibiotics plays very important roles in the guidance of medical management, in particular for the infections caused by clinical strains of multidrug-resistant Enterobacteriaceae.12,13 Our study disclosed that the synergistic bactericidal effect of imipenem–clavulanic acid is an alternative regimen for the treatment of KPC-KP infections. In subsequent study, we will develop an experimental model with related infection to investigate the in vivo effectiveness of the dual β-lactam antibiotics in the treatment of KPC-KP infections, which will provide more convincing evidences for the therapy of infections caused by these isolates.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant No. 81871690).