
Abstract
Antimicrobial resistance represents the emerging problem of modern medicine. Despite the fact that Enterobacter spp. is one of the most resistant pathogens, there has been a paucity of data on molecular epidemiology and antimicrobial susceptibility of community isolates in European countries as well as in Serbia. This study was conducted in 2016 and 2017 with the aim to investigate the prevalence of carbapenem-resistant Enterobacter spp. community isolates, molecular determinants of carbapenem resistance, and their genetic relatedness. Seventeen (1.6%) of 1,040 isolates that were positive for carbapenemase screening in accordance with European Committee on Antimicrobial Susceptibility Testing (EUCAST) recommendations were included in the study. Minimum inhibitory concentrations for selected antimicrobials were determined by broth microdilution and by disk diffusion for chloramphenicol. Multiplex polymerase chain reactions (PCRs) for blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA-48-like carbapenemase genes were performed. Clonality was assessed by enterobacterial repetitive intergenic consensus (ERIC)-PCR analysis. All isolates were multidrug resistant. The most frequent carbapenemase gene found was blaNDM (70.6%), followed by isolates coharboring blaNDM and blaOXA-48-like genes (23.5%) and a single isolate with the blaOXA-48-like gene (5.9%). ERIC-PCR molecular typing showed six different clusters (A–F) with clonal relatedness among isolates from the same institution and association of clusters E and F with the blaNDM carbapenemase gene. Our results indicate the need for Enterobacter spp. surveillance both in the community and hospitals to prevent spreading of multiresistant clones.
Introduction
The prevalence of carbapenem-resistant Enterobacterales has increased over the last decade and it represents one of the major problems of modern medicine. 1 Resistance to carbapenems is mediated by β-lactamase activity, in combination with structural mutations that lead to membrane impermeability, or by production of carbapenemases.2,3 Carbapenemase genes are located mostly on plasmids that often harbor genes resistant to other antimicrobial agents, and these multidrug-resistant clones spread rapidly worldwide. 3
After the first report of carbapenemase-producing (CP) Enterobacterales in Japan more than two decades ago, 4 they have been detected in all inhabited continents, with defined endemic areas. 5 Several studies have shown that Balkan countries are reservoirs of carbapenemases, especially blaNDM-1.6–9 A recent European Survey of Carbapenemase-Producing Enterobacteriaceae (EuSCAPE) categorized Serbia as one of the countries with the highest prevalence rates of CP isolates of Klebsiella pneumoniae and Escherichia coli. 10 Despite the fact that Enterobacter spp. is one of the three most common CP Enterobacterales, molecular epidemiology data for this genus are limited. 9 Furthermore, the majority of reports refer to nosocomially acquired carbapenemases, but data from the community are unknown or underrepresented.11–13
Therefore, the aims of the present study were to estimate the prevalence of carbapenemase-producing (CP) Enterobacter spp. among community isolates in Belgrade, to identify the types of carbapenemases, and to determine genetic relatedness of these isolates.
Materials and Methods
Study design/bacterial isolates
This cross-sectional study was conducted in two community-serving microbiology laboratories: City Institute of Public Health of Belgrade (CIPH) and Institute for Laboratory Diagnostics “Konzilijum” (ILDK), Belgrade, Serbia, which receive samples from primary care settings for the local population of around 1.6 million.
Nonduplicated Enterobacter spp. isolates from different clinical samples that met European Committee on Antimicrobial Susceptibility Testing (EUCAST) criteria for screening carbapenemase production by the disk diffusion method with a meropenem (10 μg) disk (BioRad, Marnes-la-Coquette, France)14,15 were collected during a 12-month period (August 2016–July 2017). All isolates were identified using MALDI-TOF MS (Vitek MS; bioMérieux, Marcy-l'Étoile, France). No patient-level data were involved in this study, thus no informed consent was obtained.
Antimicrobial susceptibility testing
Minimum inhibitory concentrations (MICs) for piperacillin–tazobactam, ceftriaxone, ceftazidime, cefepime, ertapenem, imipenem, ciprofloxacin, levofloxacin, gentamicin, amikacin, trimethoprim–sulfamethoxazole, and tigecycline were determined by the AST-GN76 card with automated system Vitek 2 (bioMérieux). The disk diffusion method was applied for chloramphenicol, 30 μg (BioRad). Susceptibility to colistin was determined with the broth microdilution method (ComASP™ Colistin; Liofilchem®, Italy). Results were interpreted in accordance with EUCAST guidelines. 16
Detection of carbapenemase genes
For carbapenemase screening-positive isolates, whole-cell DNA extraction from overnight bacterial culture was carried out with the QIAamp® DNA Mini Kit (Qiagen GmbH, Hilden, Germany), following the manufacturer's protocol. DNA extracts were screened for blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA-48-like carbapenemase genes by multiplex endpoint polymerase chain reaction (PCR), according to previously described protocols.17–21
ERIC-PCR analysis
Molecular typing was done by enterobacterial repetitive intergenic consensus–PCR (ERIC-PCR) with ERIC-1R (5′-ATGTAAGCTCCTGGGGATTCAC-3′) and ERIC-2 (5′-AAGTAAGTGACTGGGGTGAGCG-3′) primers, as previously described. 22 The amplified products were separated in 2% agarose gel by electrophoresis. GelJ software, version 2.0, 23 was used for cluster analysis based on Pearson correlation coefficient pairwise pattern matching and the unweighted pair group method with arithmetic averages (UPGMA). Isolates with above 90% similarity were considered to be clonally related. 24
Statistical analysis
The data obtained in this study were analyzed using the SPSS Statistics program (IBM SPSS Statistics for Windows, Version 25.0; IBM Corp., Armonk, NY), using methods of descriptive statistics, chi-square test, and Mann–Whitney U test.
Results
During the study period, a total of 1,040 Enterobacter spp. isolates from different clinical samples were screened for carbapenemase production: 795 (76.4%) were obtained from CIPH and 245 (23.6%) from ILDK. Most of the isolates originated from superficial wound swabs (36.6%, 380/1,040) and urine samples (34.2%, 356/1,040). Other specimens (29.2%, 304/1,040) included sputum, ear swabs, and eye swabs.
Screening for carbapenemase production was positive for 17 (1.6%) strains, all isolated from urine samples and identified by MALDI-TOF MS as Enterobacter cloacae/asburiae. Ten (58.8%) isolates were obtained from ILDK and 7 (41.2%) from CIPH.
All isolates were multidrug resistant with acquired resistance to piperacillin–tazobactam, ceftriaxone, ceftazidime, cefepime, ertapenem, ciprofloxacin, levofloxacin, and gentamicin. High rates of nonsusceptibility (including both intermediate resistant and resistant isolates) to trimethoprim–sulfamethoxazole (94.1%), chloramphenicol (82.3%), amikacin (70.6%), and tigecycline (70.6%) were detected. All tested isolates were susceptible to colistin (MICs: ≤0.25–0.5 μg/mL, Table 1).
Minimum Inhibitory Concentrations, Distribution of Carbapenemase Genes, and Enterobacterial Repetitive Intergenic Consensus–Polymerase Chain Reaction Clusters of Carbapenemase-Producing Enterobacter cloacae/asburiae Community Isolates
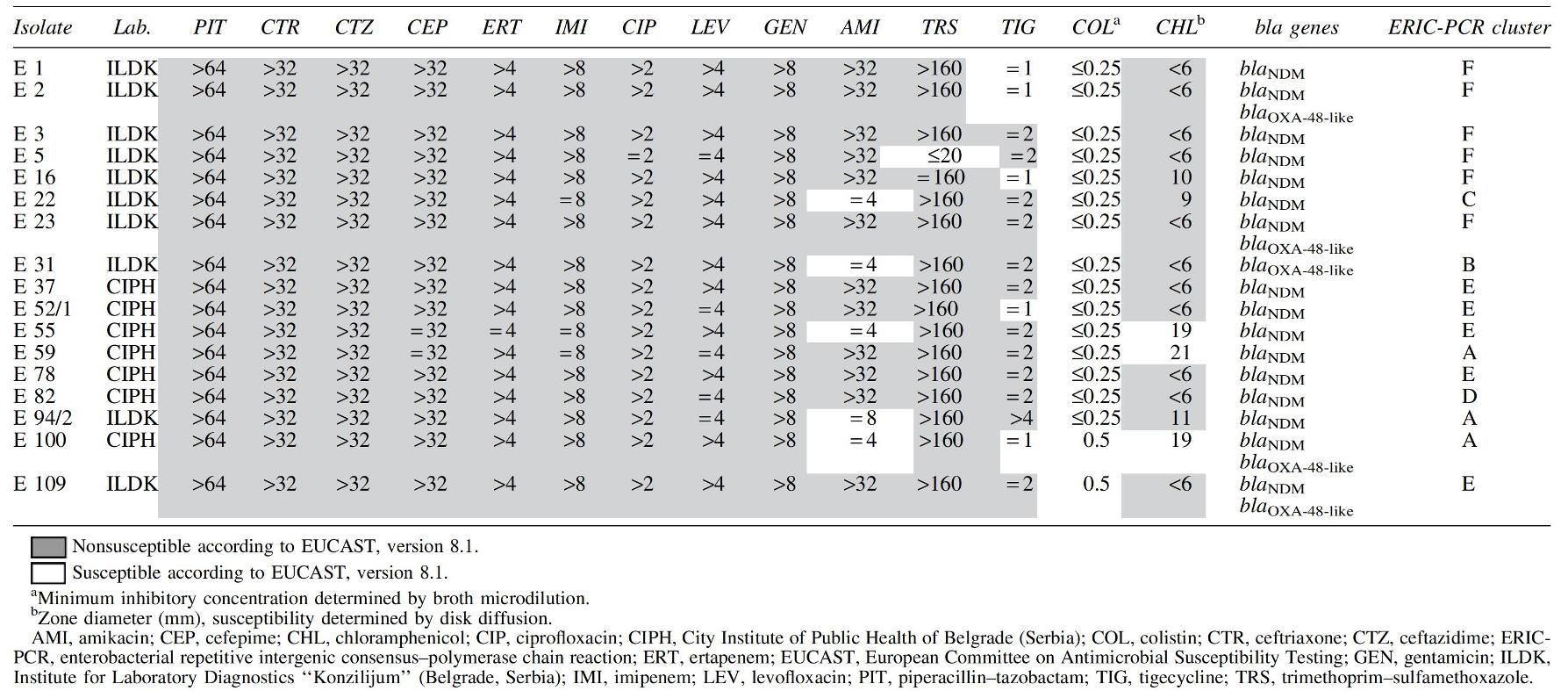
Carbapenemase-encoding genes were detected in all carbapenemase screening-positive E. cloacae/asburiae isolates, with 70.6% (12/17) of them harboring blaNDM, 23.5% (4/17) carrying both blaNDM and blaOXA-48-like, and one isolate (5.9%) harboring the blaOXA-48-like gene. A higher incidence of blaNDM-blaOXA48-like was detected in isolates obtained from ILDK (p < 0.05). Antimicrobial susceptibility and carbapenemase gene distribution are summarized in Table 1.
Molecular typing of the 17 CP E. cloacae/asburiae community isolates showed distribution in six clusters (A–F), three with a single isolate and three clusters with more than one isolate (Table 1, Fig. 1). A significant difference in frequency of clusters was noticed between isolates obtained from the different institutes: a higher frequency of cluster F was found in isolates from ILDK (p < 0.05) and a higher frequency of cluster E in isolates from CIPH (p < 0.05). Higher frequency of carbapenemase-encoding genes blaNDM-blaOXA48-like was associated with cluster F (p < 0.05) and higher frequency of blaNDM in E and F clusters, compared with all other clusters (p < 0.05).

Dendrogram and gel image obtained by enterobacterial repetitive intergenic consensus–polymerase chain reaction analysis of carbapenemase-producing Enterobacter cloacae/asburiae community isolates (n = 17). Six different clusters
Discussion
Several international studies and surveillance programs have observed a high rate of antimicrobial resistance (AMR) in invasive isolates of K. pneumoniae and Escherichia coli in Serbia,10,13 as well as one national investigation of hospital isolates of these bacteria. 25 To the best of our knowledge, there have been no AMR data on Enterobacter spp. in Serbia. In the present study, we determined the prevalence (1.6%) of CP E. cloacae/asburiae among community isolates in the Belgrade region. The overall number of studies based in community settings is limited. In a Belgian multicentric study, no CP Enterobacter spp. were found among isolates from community outpatients. 26 A similar Australian community-based survey reported only one carbapenemase-positive isolate of 239 Enterobacter spp. isolates. 27
A relatively high level of CP E. cloacae/asburiae community isolates in Serbia, all originating from urine samples, could be a consequence of overuse or misuse of antibiotics in treatment of urinary tract infections since these infections represent the main cause of antibiotic prescription and consumption in primary health care settings.28,29 However, results of our study could be in disagreement with the previous reports due to differences in study population, antimicrobial susceptibility testing methods, and carbapenem breakpoints.
The multiresistant phenotype is almost systematically associated with production of blaNDM carbapenemases,30,31 the most common carbapenemase found in Serbian E. cloacae/asburiae isolates. Our result is in accordance with findings of several case reports and studies from Serbia.32–35 Additionally, a single isolate harboring the blaOXA-48-like gene and four isolates carrying both blaNDM and blaOXA-48-like carbapenemase genes were detected. These findings represent the first report of the blaOXA-48-like-positive isolate of Enterobacter spp. in Serbia and of coexistence of the blaNDM and blaOXA-48-like genes.
It is believed that blaOXA-48-like carbapenemases originated in Turkey and have spread dominantly in Mediterranean countries. 31 Taking into account that Balkan countries lie on the major migration route from the Middle East and North Africa to Europe, dissemination of blaOXA-48-like genes and their occurrence in Serbia are expected. This is supported by results of the molecular epidemiology study on global collection of Enterobacter spp., which showed that blaNDM-positive isolates from Serbia and blaOXA-48-positive isolates from Middle East (Tunisia, Morocco, and Kuwait) belong to the same ST114A clade. 9
Dissemination of carbapenem-resistant E. cloacae/asburiae is associated with high clonal diversity accompanied by a variety of carbapenemase genes, e.g., there is no specific clone determined for blaNDM-harboring isolates on a global level.9,30,31 Annavajhala et al. emphasized underreporting of carbapenem-resistant E. cloacae/asburiae as one of the reasons for gaps in understanding its diversity. 31 Contrary to these results, Peirano et al. have shown local spreading of certain clones and clades, with specific genetic elements and carbapenemase genes. 9 In accordance with the last, a phylogenetic analysis of Serbian community E. cloacae/asburiae isolates showed clonal relatedness of the isolates from the same institution. These locally circulating clones were associated with the specific carbapenemase gene, blaNDM. Furthermore, cluster F has shown a higher frequency of isolates harboring both blaNDM and blaOXA48-like genes.
However, the major limitation of our study was the lack of clinical epidemiological data that would be of great value for analyzing the route of carbapenem-resistant E. cloacae/asburiae dissemination in community settings and from other countries. Since organization of the epidemiological survey was not feasible for a large number of patients, our study was designed as a cross-sectional study for preliminary screening of the epidemiological situation. Our results need further detailed population-level analysis with more specific typing methods.
In summary, our study represents the first analysis of Enterobacter spp. isolates in Serbia. Multidrug resistance and carbapenemase production with clonal dissemination observed among community isolates in Belgrade, Serbia, indicate a clear future need for carbapenemase surveillance of Enterobacter spp., both in community and hospital settings.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by internal funding.