
Abstract
Aims:
Acinetobacter baumannii is notorious for acquiring antibiotic resistance and causing nosocomial infections worldwide. This study aimed to investigate the prevalence and molecular characteristics of A. baumannii isolates obtained from inpatients and the intensive care unit (ICU) environment of a pediatric hospital in Shanghai, China.
Methods:
Between July 2017 and January 2018, a total of 88 A. baumannii isolates, including three obtained from ICU environmental specimens, were characterized by antibiotic susceptibility, multilocus sequence typing, and resistance genes.
Results:
Carbapenem-resistant A. baumannii (CRAB) isolates, which were resistant to all the antibiotics tested except colistin, accounted for 69.3% (61/88) of all isolates. Three sequence types (STs) were identified among the CRAB isolates, and the predominant clone was ST208 (93.4%, 57/61), which included three environmental isolates and 54 clinical isolates collected from ICU patients. Carbapenem-susceptible isolates, none of which was multidrug resistant (MDR), showed a more diverse genetic background with three known STs and 21 novel STs identified. Intrinsic blaOXA-51-like and blaAmpC were detected in all isolates, while blaOXA-23-like was only detected in all CRAB isolates. ISAba1-blaOXA-23-like, ISAba1-blaOXA-51-like, and ISAba1-blaAmpC were identified in 69.3% (all CRAB isolates), 0%, and 65.9% (58 CRAB isolates) of all isolates, respectively.
Conclusions:
A nosocomial outbreak of MDR A. baumannii ST208 producing OXA-23-like carbapenemase occurred, highlighting the necessity for strict infection control interventions in the ICU.
Introduction
Acinetobacter baumannii has become a major hospital-acquired pathogen worldwide, causing various nosocomial infections, for example, ventilator-associated pneumonia, bloodstream infection, central nervous system infection, wound infection, and urinary tract infection.1,2 Immunocompromised patients in intensive care units (ICUs) are extremely vulnerable to A. baumannii infections.1,2 Given their remarkable ability to acquire antibiotic resistance, multidrug-resistant (MDR) A. baumannii producing carbapenemases have dramatically increased.1,2 In China, the antimicrobial surveillance network found that less than 33% and 42% of A. baumannii isolates in 2005 were resistant to imipenem and meropenem, respectively, but nearly 80% of A. baumannii isolates in 2018 were resistant to both antibiotics. 3
MDR A. baumannii producing carbapenemase is included in the list of bacteria that pose the greatest threat to human health. 4 Carbapenem-hydrolyzing class D β-lactamases (CHDLs) are more commonly identified than metallo-β-lactamases (MBLs).1,2 The roles of most carbapenem-hydrolyzing oxacillinases (OXA-23 cluster, OXA-51 cluster, and OXA-58 cluster) in carbapenem resistance, as well as the role of AmpC cephalosporinase in extended-spectrum cephalosporin resistance, are associated with the presence of upstream insertion sequence (IS) elements. 1 ISAba1 is the shared promoter for blaOXA-23-like, blaOXA-51-like, blaOXA-58-like, and blaAmpC. 1 An amino acid substitution in the quinolone resistance-determining region (QRDR) of gyrA gene from Ser83 to Leu83 is associated with fluoroquinolone resistance.5,6
To develop effective preventative and therapeutic strategies against A. baumannii infections, it is essential to determine the prevalence and resistance profiles of A. baumannii isolates. The few studies on the molecular characterization of A. baumannii isolates obtained from children in mainland China had not investigated environmental specimens or sequence types (STs).7–9 Hence, the objectives of the present study were as follows: (1) to investigate the molecular epidemiology of carbapenem-resistant A. baumannii (CRAB) and carbapenem-susceptible A. baumannii (CSAB) isolates obtained from inpatients in a pediatric hospital in Shanghai, China; (2) to detect and evaluate environmental A. baumannii isolates; and (3) to characterize the antibiotic resistance mechanisms of the major epidemic MDR clones.
Materials and Methods
Bacterial isolates
Between July 2017 and January 2018, a total of 88 nonduplicate A. baumannii isolates were collected from the Shanghai Children's Medical Center, which is one of the top five pediatric hospitals in China with 604 beds, including 150 beds in neonatal ICU, pediatric ICU, cardiothoracic ICU, and emergency ICU, and ∼22,000 hospital discharges per year. Isolates obtained from outpatients and inpatients within 48 hours of hospitalization were excluded. The first isolate obtained from each patient was selected for analysis. All isolates, including clinical and environmental isolates, were initially identified by colony morphology, biochemical testing, and VITEK 2 GN ID cards (bioMérieux, Lyon, France), and subsequently confirmed by detection of the 16S-23S rRNA intergenic spacer region and the recA gene. 10
Ethical approval
The Ethics Committee of Shanghai Children's Medical Center exempted this study from review as it focused on bacteria.
Routine hand sampling and air monitoring
Health care workers' hands and the air in ICUs are sampled monthly by the nursing department. Moistened sterile cotton swabs collected from hands were incubated in Luria-Bertani agar in ambient air for 24–48 hours at 35 ± 0.5°C in an electrothermal incubator. Air specimens were collected by placing Luria-Bertani agar plates at a height of 0.8–1.5 m. 11
Environmental sampling in response to nosocomial infection outbreak
After detection of 15 CRAB nosocomial infection cases in an ICU in December 2017, an environmental sampling was performed by the hospital infection management department in this ward on January 08, 2018. The entire unit is cleaned daily. The sampling was carried out in the afternoon. Six rooms were sampled. Specimens were collected from potential contaminated sources, which were frequently touched by health care workers' hands, including doors, sinks, electric switches, telephones, bedrails, monitors, ventilator control panels, stethoscopes, and infusion pumps. All large and flat areas were sampled with sterile sponge swabs premoistened with a neutralizing solution, while uneven or complex surfaces were sampled with sterile cotton-tipped swabs premoistened with the neutralizing solution. The entire surfaces of door knobs (both sides of each door, n = 12), electric switches (n = 6), telephone receivers (n = 2), bedrails (n = 24), and stethoscopes (n = 12) were sampled. The sinks (n = 6), telephone keypads (n = 2), and hand-touched surfaces of monitors, ventilator control panels, and infusion pumps (n = 12, respectively) were sampled, 100 cm2 area, using a 5 × 5 cm sampling plate. 11 The potential hand-touched surfaces of both sides of each door were sampled, about 1 m2 area (n = 12). A total of 112 environmental specimens were inoculated onto blood agar and MacConkey agar, and incubated at 35°C for 24 hours.
Antibiotic susceptibility testing
Susceptibility testing to 16 antibiotics (ampicillin, cefazolin, cefotetan, ceftriaxone, ceftazidime, cefepime, aztreonam, ampicillin/sulbactam, piperacillin/tazobactam, levofloxacin, ciprofloxacin, trimethoprim/sulfamethoxazole, nitrofurantoin, gentamicin, tobramycin, and imipenem) was performed using the bioMérieux VITEK 2 system according to the manufacturer's instructions. The minimal inhibitory concentration (MIC) of colistin (colistin sulfate salt, Sigma-Aldrich) was determined by a broth dilution method. Results were interpreted in accordance with the Clinical and Laboratory Standards Institute guidelines (CLSI, 2017). Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as reference strains for susceptibility testing. MDR was defined as resistance to three or more antibiotic classes. 12
Multilocus sequence typing analysis
All clinical and environmental isolates were screened according to the Oxford scheme described on the A. baumannii multilocus sequence typing (MLST) website (http://pubmlst.org/abaumannii/) to detect the following seven housekeeping genes: gltA, gyrB, gdhB, recA, cpn60, gpi, and rpoD. 13 The sequences of the polymerase chain reaction (PCR) products were compared with the existing alleles available on the PubMLST database, and the allelic number (ST) was determined for each sequence. Clustering of related STs was determined using eBURST software. 14 Alleles and STs that had not been previously described were submitted to the curator of the database, and were assigned new designations.
Detection of antibiotic resistance genes
Two main MBL genes (blaIMP and blaVIM), four main CHDL gene groups (blaOXA-23-like, blaOXA-24-like, blaOXA-51-like, and blaOXA-58-like), and the cephalosporinase gene (blaAmpC) were detected by PCR using previously described primers.15–17 The presence of ISAba1 was examined by PCR, and the proximity of this element to blaAmpC, blaOXA-23-like, and blaOXA-51-like was detected as previously described.17,18 Amplification of the gyrA gene was performed as previously described. 5 The QRDR of gyrA gene, which was defined as gyrA nucleotide positions 241 to 243 in Acinetobacter spp., was amplified and sequenced by established procedures. 6
Statistical analyses
Antibiotic resistance rates were compared between CRAB and CSAB, clonal complex (CC) 92 and non-CC92, and between ST208 and non-ST208 using Fisher's exact test. Statistical analyses were performed by Stata software (version 10.1/SE; Stata Corp., College Station, TX). A p-value <0.05 was considered to indicate statistical significance.
Results
Clinical features
Between July 2017 and December 2017, a total of 85 consecutive A. baumannii isolates were obtained from hospitalized patients (44 males and 41 females, aged 5 days to 15 years), 88.2% (75/85) of whom were treated in ICUs. These isolates were obtained from sputum (80%, 68/85), bronchoalveolar lavage fluid (9.4%, 8/85), blood (5.9%, 5/85), catheters (3.5%, 3/85), and urine (1.2%, 1/85). The most prevalent diagnosis was pneumonia (89.4%, 76/85). In January 2018, three A. baumannii isolates were obtained from a telephone, an electric switch, and the outer surface of a door of the ICU, respectively. Monthly routine cultures of hands and air specimens were all negative.
MLST of CRAB and CSAB
The allelic profiles of all isolates and novel STs are listed in Table 1. CRAB accounted for 69.3% (61/88) of all isolates. Three STs, ST208, ST373, and ST369, were identified among the CRAB isolates. ST208 accounted for 93.4% (57/61) of all CRAB isolates, including 54 isolates recovered from ICU patients and three isolates recovered from ICU environmental specimens. Three (4.9%, 3/61) non-ST208 CRAB isolates belonged to ST373, and the other one belonged to ST369. In contrast, CSAB had a more diverse genetic background. A total of 24 different STs were identified among CSAB isolates, including three known STs and 21 novel STs. ST373 was the only clone identified among both CRAB and CSAB isolates. The eBURST algorithm clustered all 26 STs into four groups and 16 singletons (Fig. 1). ST208 and ST369, each a single-locus variant of ST92, have been reported to belong to CC92.19,20
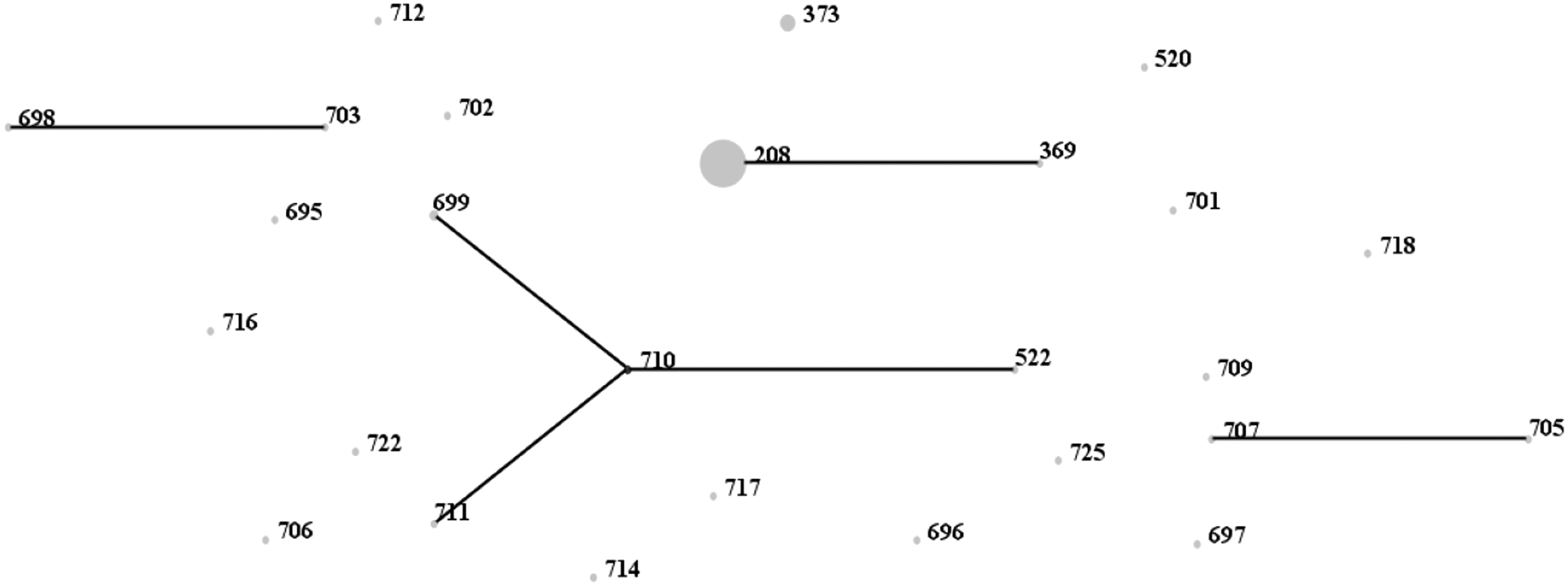
eBURST analysis of all Acinetobacter baumannii isolates in this study based on multilocus sequence typing data. The numbers represent STs. The size of each circle corresponds to the number of isolates. STs belonging to the same cluster are connected by a line. STs, sequence types.
Characteristics of 88 Acinetobacter baumannii Isolates Obtained from Pediatric Patients and Environmental Specimens
Novel ST.
ISAba1 was located upstream of blaOXA-23-like/blaOXA-51-like/blaAmpC.
IS, insertion sequence; ST, sequence type.
Antibiotic resistance profiles and distribution of antibiotic resistance genes
The antibiotic susceptibility of all isolates is summarized in Table 2. The MIC of colistin in all isolates was ≤2 μg/mL. None of the CSAB isolates was MDR, while the CRAB isolates were more frequently resistant to antibiotics. CC92 isolates and ST208 strains showed more significant drug resistance (Table 3).
Susceptibility of 88 Acinetobacter baumannii Isolates to 17 Antibiotic Agents
Antibiotic Resistance Rates of Different Clones of Acinetobacter baumannii Isolates
CRAB, carbapenem-resistant A. baumannii; CSAB, carbapenem-susceptible A. baumannii.
The distribution of antibiotic resistance genes is summarized in Table 1. Only blaOXA-51-like and blaOXA-23-like were detected, while blaIMP, blaVIM, blaOXA-24-like, and blaOXA-58-like were not detected in any isolate. The two intrinsic β-lactamase genes, blaOXA-51-like and blaAmpC, were detected in all isolates. blaOXA-23-like was detected in all CRAB isolates but not in any CSAB isolate. ISAba1 was upstream of blaOXA-23-like, but not upstream of blaOXA-51-like. blaAmpC with an upstream ISAba1 and Ser83Leu mutation in gyrA were both identified in 95.1% (58/61) of CRAB isolates. The 58 CRAB isolates belonged to CC92. Three CRAB ST373 strains without ISAba1 upstream of blaAmpC and without gyrA mutation were susceptible to ceftazidime, levofloxacin, and ciprofloxacin, but resistant to cefepime.
Discussion
A. baumannii is one of the most refractory pathogens worldwide. CC92 is by far the largest and most widely disseminated CC both in China and worldwide.21,22 The predominant clone in this study, ST208, also belongs to CC92.19,20 ST208 strains have been isolated from adult patients in several provinces of China since 2011.23,24 The ST208 genotype was shared by the majority of isolates (58.7%, 27/46) collected from three tertiary hospitals in Shanghai between 2011 and 2012. 25 In the present study, an outbreak of ST208 emerged in pediatric patients in the hospital environment, indicating that ST208 spreads rapidly. ST92 was reported to be the most prevalent and widely distributed clone in China (34.4%, 301/875 isolates collected from 27 provinces between January 2009 and December 2010). 22 However, due to the problems in the housekeeping genes gpi and cpn60, ST92 was found to be in fact ST208 when reexamined by whole-genome sequence data. 26 In this study, which began after the MLST database had changed the primers for amplifying the two genes, ST92 was not detected, and most isolates belonged to ST208. Therefore, ST208 is perhaps the real predominant clone in China since 2009.
Several factors are associated with the dissemination of ST208 in hospital settings. All ST208 isolates in this study showed resistance to all the tested antibiotics except colistin. MDR may confer a selective advantage on ST208 strains in a hospital environment, especially in the ICU, where bacteria encounter intense antibiotic selection pressure. Three ST208 isolates were obtained from environmental surfaces, which were outside the reach of patients. Since A. baumannii is not a typical environmental organism, 1 contamination of these high-touch surfaces was probably due to health care workers touching the surfaces with their contaminated hands. Moreover, health care workers could also acquire nosocomial pathogens on their hands after contact with contaminated environmental surfaces. 27 The findings of this study suggested reinforcement of hand hygiene.
The blaOXA-23 gene contributes to increasing carbapenem resistance in A. baumannii worldwide, and is the most commonly acquired gene associated with carbapenem resistance in China. 22 ST373 was observed in three carbapenem-susceptible isolates and three carbapenem-resistant isolates. The three CSAB strains without blaOXA-23-like were obtained in July and September, while the three CRAB strains harboring blaOXA-23-like were obtained in December. This potentially hinted at the evolution from CSAB to CRAB through horizontal transfer of blaOXA-23-like, as well as the insertion of ISAba1. Therefore, CSAB might be a potential reservoir of CRAB and should be monitored.
Sulbactam has clinically relevant intrinsic antibiotic activity against Acinetobacter spp. 1 and appears to be more efficacious than polymyxins to treat susceptible CRAB infections. 28 Ampicillin/sulbactam, cefoperazone/sulbactam, and sulbactam alone are the mainstay treatments of CRAB in mainland China. All patients who were infected with CRAB in the present study were treated with ampicillin/sulbactam plus cefoperazone/sulbactam or meropenem or imipenem/cilastatin plus ampicillin/sulbactam or cefoperazone/sulbactam. However, more than half of A. baumannii isolates obtained from lower respiratory tract, blood, and cerebrospinal fluid of patients in China are resistant to sulbactam, 3 and OXA-23, ISAba1-ampC, and blaTEM-1D represent the prevalent mechanisms contributing to sulbactam resistance.29,30 In this study, all the 61 CRAB isolates were resistant to ampicillin/sulbactam, implying that the combination therapy of β-lactam plus sulbactam was inadequate. Although no data are currently available on pharmacokinetics and safety in pediatric patients, 31 polymyxins-based combination regimens have been suggested as first-line therapies for CRAB infections in children. 32 In mainland China, where polymyxins were not commercially available until 2018, it is difficult to recommend polymyxins as first-line agents due to the high price (polymyxin B costs nearly USD500/50 mg and colistin costs about USD350/50 mg, both of which are not covered by health insurance). However, polymyxins should be considered last-resort for children with life-threatening infections caused by sulbactam-resistant CRAB. 33
Unlike ICUs, the general wards included in this study usually lacked routine culture monitoring for newly admitted patients, making it difficult to distinguish new cases who acquired A. baumannii in the hospital from imported cases who acquired A. baumannii before admission. However, as all ST208 clinical strains were obtained after 48 hours of ICU admission, this outbreak was a nosocomial CRAB infection outbreak that occurred in ICUs. Since no positive cultures were collected from monthly routine sampling, we were unable to infer health care workers' hand carriage to be the source of transmission of A. baumannii. As environmental investigation was conducted only once on a single day, and three environmental isolates were collected from different environmental surfaces, we were unable to identify whether a common environmental source was present. To observe actual patient care activities, the hospital infection management department did not carry out environmental investigation immediately after routine cleaning in the morning. Nonetheless, the investigation was not a surprise inspection. During a forewarned investigation, hand hygiene compliance rates might be higher, and environmental cleaning might be performed more carefully. We suspect that transient health care workers' hand carriage of A. baumannii and environmental contamination were missed by the surveillance cultures.
In summary, an outbreak of MDR A. baumannii ST208 producing OXA-23-like carbapenemase was identified in a children's hospital in Shanghai, China, highlighting the necessity for developing strict infection control interventions in the ICU. Both molecular epidemiological investigations and environmental cultures are helpful and essential to survey A. baumannii outbreaks.
Footnotes
Acknowledgments
The authors thank all the patients who contributed their specimens and clinical data for this study. They also thank the microbiologists and technical staff of Shanghai Children's Medical Center for collecting the bacterial isolates and for laboratory testing.
Disclosure Statement
The authors have no commercial associations that might create a conflict of interest related to the submitted article.
Funding Information
This study was supported by the National Natural Science Foundation of China (grant 81301392) and the Training Program for Clinical Medical Young Talents in Shanghai (HYWJ201605).